Article Text

Abstract
Objective To evaluate the prognostic performance of high-sensitivity cardiac troponin T (hs-cTnT) compared with the ESC-SCORE.
Methods We included low-risk outpatients with stable cardiovascular (CV) disease categorised into need for non-secondary and secondary prevention. The prognostication of hs-cTnT at index visit was compared with the European Society of Cardiology-Systematic COronary Risk Evaluation (ESC-SCORE) with respect to all-cause mortality (ACM) and two composite endpoints (ACM, acute myocardial infarction (AMI) and stroke and ACM, AMI, stroke and rehospitalisation for acute coronary syndrome (ACS) and decompensated heart failure (DHF)).
Results Within a median follow-up of 796 days, a total of 16 deaths, 32 composite endpoints of ACM, AMI and stroke and 83 composite endpoints of ACM, AMI, stroke, rehospitalisation for ACS and DHF were observed among 693 stable low-risk outpatients. Using C-statistics, measurement of hs-cTnT alone outperformed the ESC-SCORE for the prediction of ACM in the entire study population (Δarea under the curve (AUC) 0.221, p=0.0039) and both prevention groups (non-secondary: ΔAUC 0.164, p=0.0208; secondary: ΔAUC 0.264, p=0.0134). For the prediction of all other secondary endpoints, hs-cTnT was at least as effective as the ESC-SCORE, both in secondary and non-secondary prevention. Using continuous and categorical net reclassification improvement and integrated discrimination improvement, hs-cTnT significantly improved reclassification regarding all endpoints in the entire population and in the secondary prevention cohort. In non-secondary prevention, hs-cTnT improved reclassification only for ACM. The results were confirmed in an independent external cohort on 2046 patients.
Conclusions Hs-cTnT is superior to the multivariable ESC-SCORE for the prediction of ACM and a composite endpoint in stable outpatients with and without relevant CV disease.
Trial registration number NCT01954303; Pre-results.
- coronary artery disease
- risk factors
- prevention
- troponin
- score
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Elevated values of high sensitivity troponins are indicative of adverse outcome irrespective of the underlying reason.
What does this study add?
This study compares for the first time the prognostic value of high sensitivity cardiac troponin T in relation to the European Society of Cardiology-Systematic COronary Risk Evaluation.
How might this impact on clinical practice?
Multivariable risk scores are rarely used in daily clinical practice due to inconvenience.
In contrast, high sensitivity troponins are widely available and provide an easy-to-use risk stratification tool.
They might therefore facilitate risk stratification with a better acceptance in daily clinical practice.
Introduction
Cardiac troponins are recommended as the preferred biomarkers for the diagnosis of acute myocardial infarction (AMI1). After more sensitive and highly sensitive troponin assays replaced conventional cardiac troponin assays almost 10 years ago, AMI could be diagnosed earlier with a more accurate discrimination between unstable angina (UA) and non-ST elevation myocardial infarction.2 3 Furthermore, a higher prevalence of elevated troponins due to myocardial injury for non-coronary and non-cardiac reasons is observed.4 5 Irrespective of the underlying release mechanism, elevated troponin levels were found to be highly predictive for cardiovascular (CV) endpoints including mortality.6–8 A high predictive value of cardiac troponin has also been confirmed in stable coronary artery disease in large trials like the Prevention of Events with ACE Inhibition (PEACE)9 or the Heart Outcomes Prevention Evaluation (HOPE) study.10
While several multivariable clinical risk scores have been prospectively validated for the risk stratification of patients with an acute coronary syndrome (ACS),11 12 there is no clinical risk score for individualising secondary prevention in patients with coronary artery disease (CAD), CV disease, peripheral artery disease (PAD) or with a history of remote AMI. In contrast, several risk scores have been developed and validated for risk assessment in primary prevention such as the Framingham Score13 and the European Society of Cardiology-Systematic COronary Risk Evaluation (ESC-SCORE)14 which are recommended by European guidelines.15 The ESC-SCORE has been validated in a large cohort of patients, ethnicities and for the endpoint CV mortality.14 Unfortunately, these multivariable scores are rarely used in clinical routine.16 17
Cardiac troponins are widely available in primary care and in hospitalised patients, provide plausible biological information on underlying pathophysiology, are established in the diagnosis of ACS,1 improve risk assessment in ACS,18 atrial fibrillation19 and pulmonary embolism20 and may guide therapeutic management in several acute and chronic diseases. It is tempting to speculate that a single biomarker-based risk prediction tool may be better adopted for prognostication than a complex multivariate score. Therefore, the aim of this study was to compare the performance of high-sensitivity cardiac troponin T (hs-cTnT) alone against the European guideline recommended ESC-SCORE in a stable outpatient population presenting with or without relevant CV disease, that is, patients who require secondary prevention measures or not.
Methods
Study population
We screened 965 individuals presenting to the outpatient unit of Hugo A Katus at the Department of Cardiology of the University Hospital of Heidelberg between June 2009 and June 2010. These patients were either healthy (almost healthy with minor manifestation of CV disease) or asymptomatic with or without stable symptoms or signs of CV disease. Patients without obvious CV disease, those with chronic arrhythmias like atrial fibrillation, pacemaker follow-up visits or arterial hypertension were summarised into the non-secondary prevention group, whereas patients with a history of documented AMI, previous percutaneous coronary intervention (PCI), previous coronary artery bypass graft (CABG), angiographically confirmed CAD (defined as >50% luminal obstruction), asymptomatic or symptomatic peripheral arterial disease (PAD), previous transient ischemic attack (TIA) or stroke were categorised into secondary prevention. Individuals who were potentially belonging to both groups were classified as secondary prevention. Patients received routinely ECG, carotid scan, blood testing and stress tests. The latter included exercise ECG, stress echocardiography and stress MRI. Imaging tests were performed at the discretion of the attending cardiologist including coronary CT, cardiac MRI, pulmonary function tests and Ankle-Brachial-Index measurements.
All patients with acute manifestations of CV disease such as recent ACS or acute heart failure were excluded to avoid a confounding effect of acute hs-cTnT elevation.
The diagnostic workup comprised a 12-lead-ECG, stress testing (ECG, echocardiography or MRI), carotid ultrasonography, CT coronary angiography, cardiac MRI, pulmonary function testing as well as Holter ECG and 24 hours blood pressure recording at the discretion of the treating physician. Furthermore, laboratory testing including hs-cTnT, blood count, clinical chemistry and coagulation tests were performed. A detailed description of the study population is available elsewhere.21
Left ventricular (LV) function was determined via echocardiography and categorised according to the ejection fraction (EF) into normal (≥55%), mildly reduced (45%–54%), moderately reduced (30%–44%) and severely reduced (<30%). If available, MRI was used to determine LV function. Pulmonary artery pressure was measured by echocardiography or right heart catheterisation. Aortic valve stenosis was quantified by two-dimensional echocardiography or heart catheterisation.
All patients of the original cohort were seen by the same physicians (HAK and EG) and treated according to the current guidelines. Inclusion criteria were a stable clinical course, a documented hs-cTnT value on index visit and at least one follow-up visit. Stable disease was defined by the absence of recent ACS, coronary intervention or acute cardiac decompensation since the previous visit. Patients with a history of heart transplantation were excluded.
Follow-up was accomplished by hospital records, questionnaires, phone calls and death certificates. All scheduled and unscheduled visits or hospital admissions were recorded during follow-up. Due to the retrospective character of this analysis, informed consent was not possible and had not to be obtained according to a statement of the ethics committee of the University of Heidelberg.
EXCELSIOR cohort
The main findings of the original study cohort were tested in an independent cohort of 2046 stable patients of the Effect of Clopidogrel Loading and Risk of PCI (EXCELSIOR) trial. A detailed description of the methodology and patient characteristics have been published by Hochholzer et al.22 In this study, subjects were recruited from consecutive patients referred for an elective invasive coronary angiography due to suspected stable CAD. Individuals were then categorised into a secondary and non-secondary prevention category according to the presence or absence of significant coronary artery stenosis >50% (see online supplementary file 1).
Supplementary file 1
Outcome measures
Three prognostic endpoints were defined: (1) all-cause mortality (ACM); (2) a composite of ACM, AMI and stroke and (3) a composite of ACM, AMI, stroke and rehospitalisation for ACS and decompensated heart failure (DHF). ACM was defined as death from any cause including CV and non-CV conditions. AMI was defined according to the European Society of Cardiology third universal definition of myocardial infaction1 including ST-segment elevation and non-ST-segment elevation myocardial infarction. Stroke was defined according to the Updated definition of stroke for the 21st century of the American Heart Association/American Stroke Association.23 ACS was defined according to the European Society of Cardiology Guidelines on the management of ACSs in patients presenting without persistent ST-segment elevation24 and the European Society of Cardiology Guidelines for the management of AMI in patients presenting with ST-segment elevation.25 DHF was defined by presentation to the emergency department with symptoms of heart failure including angina or dyspnoea requiring diuretic therapy.
Laboratory measurements
Only troponin measurements during routine presentations were considered. Hs-cTnT concentrations were tested immediately from fresh blood samples. Cardiac troponin was measured in serum on a COBAS E411 using the hs-cTnT assay by Roche Diagnostics. The limit of blank and limit of detection have been determined to be 3 ng/L and 5 ng/L.26 The 10% CV was determined at 13 ng/L in 100 measurements in the authors’ laboratory. The interassay CV was 8% at 10 ng/L and 2.5% at 100 ng/L. The intra-assay CV was 5% at 10 ng/L and 1% at 100 ng/L. The hs-cTnT assays were not affected by a lot to lot variation that occurred in 2009 and 2010.27
ESC-SCORE
The CV risk was calculated for every patient according to the original publication of the ESC-SCORE14 considering the risk variables at index visit. Individual risk was calculated according to the ESC-SCORE charts expressed by the 10-year risk for a fatal CV event. The recalibrated low risk chart was used in this population as recommended by the guidelines.15
Statistical analysis
Due to the pilot character of this observational study with a prespecified recruitment period of 12 months that was defined by the implementation of hs-cTnT as the routine laboratory troponin assay at the University of Heidelberg, a sample size calculation was not performed.
Variables were tested for normal distribution using the D’Agostino-Pearson test and were presented either as means±SD deviation, or as medians with 25th and 75th percentiles. Discrete variables were compared using Χ2 or Fisher’s exact test. Continuous variables were compared using either Student’s t-test for parametric or Mann-Whitney U test for non-parametric variables. Alternatively, we used analysis of variance (ANOVA) after logarithmic transformation of the data. If the ANOVA test was found positive (p<0.05), then the Student-Newman-Keuls test for pairwise comparison of subgroups was applied.
We defined three endpoints to assess the prognostic performance: (1) ACM, (2) a composite endpoint of ACM, recurrent AMI and stroke and (3) a composite endpoint of ACM, recurrent AMI, stroke and hospitalisation for ACS or DHF.
The prognostic performance of the ESC-SCORE and hs-cTnT for the defined endpoints was evaluated by C-statistics plotting and receiver operating characteristic (ROC) curves comparing the differences of the areas under the curve (AUC). The risk was determined by the 10-year risk for a fatal CV event as indicated by the ESC-SCORE charts and the hs-cTnT value on index visit. AUCs were compared using the test of DeLong et al.28
To determine the additional value of hs-cTnT in the prediction of the defined endpoints, we performed a logistic regression analysis and compared the prognostic performance of the combined variable (hs-cTnT+ESC-SCORE) with the performance of the ESC-SCORE in an ROC analysis.
In order to evaluate benefits in risk prediction, reclassification analyses were performed to quantify improvements in model performance (in terms of correct reclassification to respective risk categories) after addition of hs-cTnT.29 Therefore, the categorical and the continuous net reclassification improvement (NRI) and the integrated discrimination improvement (IDI) were calculated. Risk categories for the respective endpoint were set as 0%–10% for low risk, 10%–20% for intermediate risk and ≥20% for high risk according to the recommendations of the National Cholesterol Education Programme.30 Statistical analyses were performed with SPSS V.20.0, MedCalc V.11.1 (MedCalc software, Mariakerke, Belgium), R V.3.1.2 (R Core Team, Vienna, Austria), as well as the R package ‘PredictABEL’.31 32 All tests were two-tailed and a p value of <0.05 was considered statistically significant.
Results
Baseline characteristics
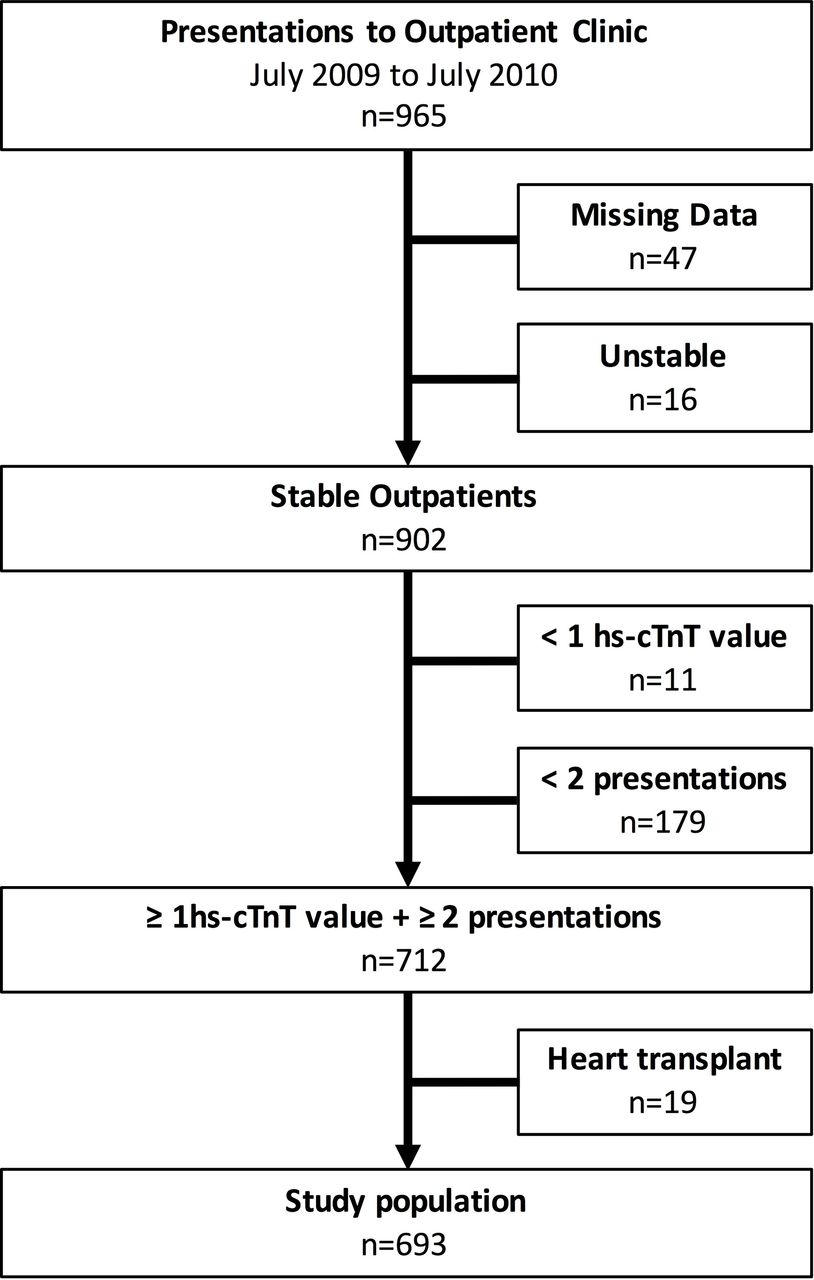
We screened 965 patients presenting to the outpatient clinic of HAK. A total of 63 subjects were excluded due to missing data (n=47) or an unstable clinical course (n=16). Of the remaining 902 stable outpatients, 11 individuals were excluded due to a missing hs-cTnT value and 179 patients could not be included because of less than two visits to the outpatient clinic. Finally, 19 patients were not recruited since they had a history of heart transplantation (figure 1). The final study cohort comprised 693 patients, of which 333 were classified as non-secondary prevention and 360 as secondary prevention.
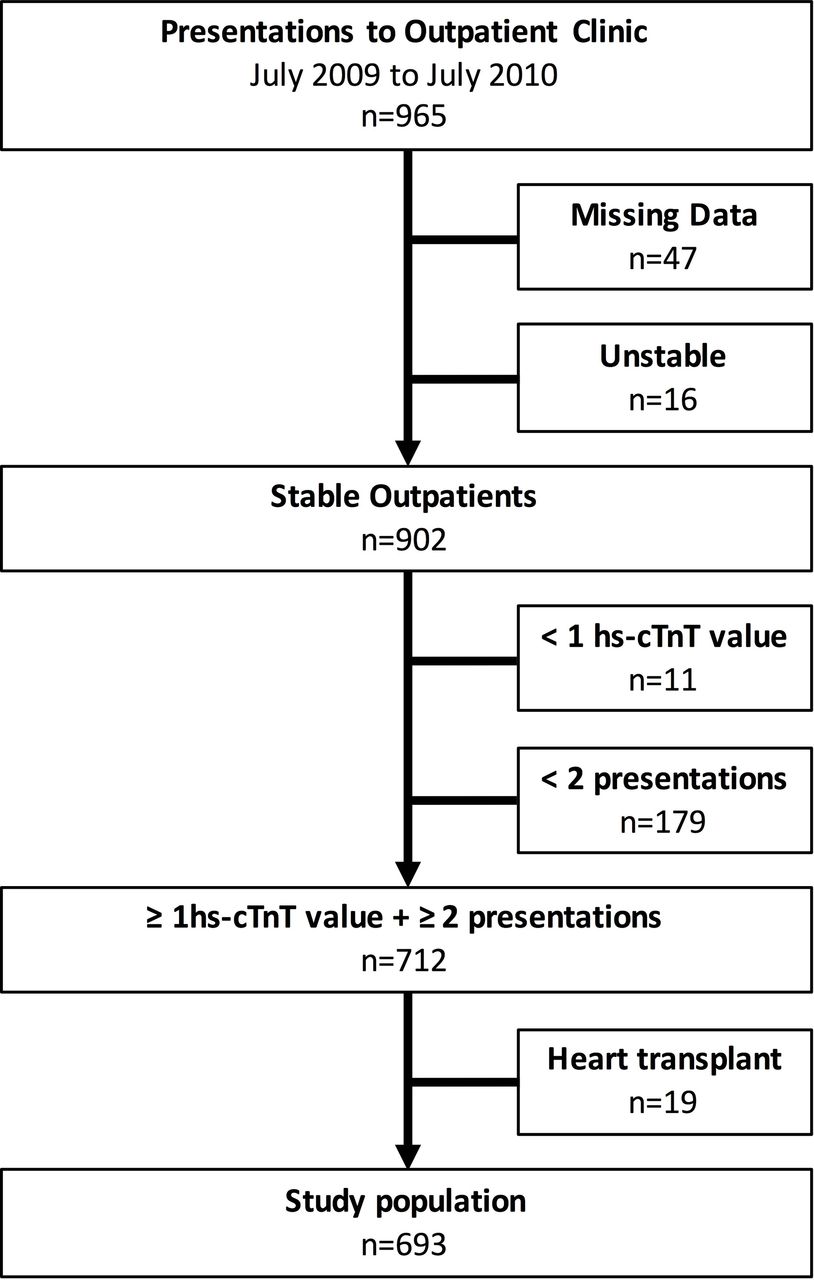
Study population.
Follow-up was available in 686 patients (98.9%) with a median time of 796 days (25th; 75th percentile: 631–935 days). A median of three (25th; 75th percentile: 2–4) scheduled ambulatory visits with a median of three (25th; 75th percentile: 2–4) hs-cTnT measurements were documented. hs-cTnT levels exceeding the 99th percentile (ie, 14 ng/L) on index visit were found in 146 patients (21.1%). A history of an ACS was documented in 27% of all patients. Seven out of 693 patients (1%) had an AMI within 6 months before index visit with a median time since last AMI of 62.6 months (95% CI 48.5 to 79.2) before index visit.
The baseline characteristics split by cardiac troponin below or exceeding the 99th percentile are displayed in table 1. Most baseline characteristics differed significantly. Patients with values >14 ng/L were older, were more likely to be male, had more often CV risk factors such as diabetes mellitus or arterial hypertension and were more often smokers. In addition, they had more often a history of CAD, AMI, CABG, cardiomyopathy, heart failure, arrhythmias, valvular heart disease, vascular and pulmonary diseases, renal failure and stroke/TIA. Patients with hs-cTnT values exceeding the 99th percentile had a higher CV risk as indicated by the ESC-SCORE. Most patients were seen because of a former ACS (25.4%, median time since last ACS: 62.5 months, 95% CI 28.9 to 160.9 months) or stable angiographically confirmed significant CAD with or without a history of elective coronary revascularisation (26.4%). Five patients (0.7%) were seen following a cerebrovascular event (TIA/stroke). Echocardiography (92.6%) and ECG (94.1%) were performed in almost every patient, and an ECG stress test (64.4%) was performed in the majority of patients.
Baseline characteristics according to troponin status
General outcome characteristics
In the overall cohort, we observed 16 deaths (ACM), 32 patients with ACM, AMI or stroke and 83 patients with ACM, AMI, stroke and rehospitalisation for ACS or DHF. Total mortality of the entire cohort was 2.03% during follow-up (796 days) corresponding to a total annual mortality rate of 0.93%.
The prognostic performance of the ESC-SCORE and hs-cTnT in secondary and non-secondary prevention is displayed in table 2.
Prognostic performance of the ESC-SCORE and high-sensitivity cardiac troponin T in non-secondary and secondary prevention
The ESC-SCORE performed superior regarding the prediction of ACM in the non-secondary prevention group compared with the secondary prevention group (figure 2A). Regarding the composite endpoint of ACM, AMI and stroke, we also observed a better performance of the ESC-SCORE in non-secondary prevention compared with secondary prevention patients (figure 2B), whereas the prognostic performance for the prediction of the composite endpoint ACM, AMI, stroke, rehospitalisation for ACS or DHF was comparable between both groups (figure 2C).

Prognostic performance of the ESC-SCORE for different outcomes in non-secondary and secondary prevention.
Hs-cTnT performed better in the prediction of ACM in the non-secondary prevention group compared with the secondary prevention group, whereas the prognostication of the composite endpoints of ACM, AMI and stroke and ACM, AMI, stroke, rehospitalisation for ACS or DHF was comparable.
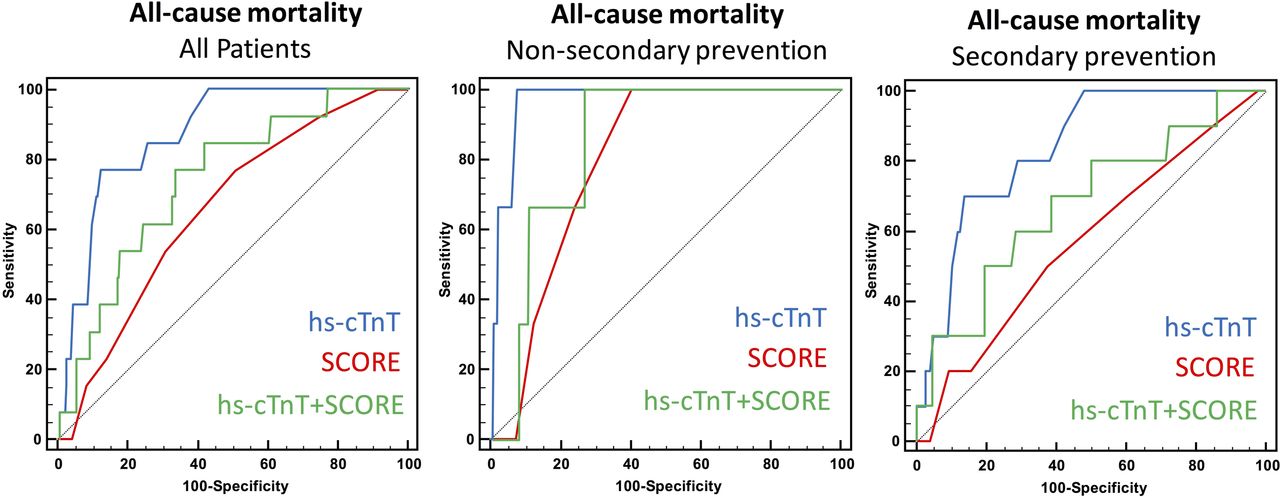
In the prediction of ACM, the hs-cTnT value on index visit (AUC 0.878, 95% CI 0.805 to 0.950) outperformed the ESC-SCORE (AUC 0.657, 95% CI 0.526 to 0.789) in the overall study population (ΔAUC 0.221, p=0.0039, figure 3A). Hs-cTnT was also superior to the ESC-SCORE in the prediction of ACM in non-secondary prevention (hs-cTnT: AUC 0.962, 95% CI 0.924 to 1.000; ESC-SCORE: AUC 0.798, 95% CI 0.664 to 0.931; ΔAUC 0.164, p=0.0208, figure 3B). In secondary prevention, with 0.264 (p=0.0134, figure 3C) the delta between hs-cTnT (AUC 0.836, 95% CI 0.734 to 0.937) and the ESC-SCORE (AUC 0.572, 95% CI 0.389 to 0.755) was even higher.

{kind=link}
{kind=link}
{kind=link}
Prognostic performance of high-sensitivity cardiac troponin T (hs-cTnT) compared with the European Society of Cardiology-Systematic COronary Risk Evaluation (ESC-SCORE) in the prediction of all-cause mortality in non-secondary and secondary prevention.
Hs-cTnT and the ESC-SCORE had a comparable performance regarding the prediction of the composite endpoint ACM, AMI and stroke in secondary (ΔAUC hs-cTnT vs ESC-SCORE: 0.110, p=NS, online supplementary figure 1) and non-secondary prevention (ΔAUC hs-cTnT vs ESC-SCORE: 0.119, p=NS, online supplementary figure 2).
Supplementary file 2
![[openhrt-2017-000710-SP2.jpg]](https://openheart.bmj.com/content/openhrt/5/1/e000710/DC2/embed/inline-supplementary-material-2.jpg?download=true){kind=link}
Supplementary file 3
![[openhrt-2017-000710-SP3.jpg]](https://openheart.bmj.com/content/openhrt/5/1/e000710/DC3/embed/inline-supplementary-material-3.jpg?download=true){kind=link}
The prognostic performance of hs-cTnT to predict the composite endpoint ACM, AMI, stroke, rehospitalisation for ACS or DHF was higher in the secondary prevention group (ΔAUC hs-cTnT vs ESC-SCORE: 0.136, p=0.02), whereas no difference was observed in the non-secondary prevention group (ΔAUC hs-cTnT vs ESC-SCORE: 0.077, p=NS).
Reclassification analysis according to hs-cTnT status (>14 ng/L at index visit) is displayed for the entire population as well as the secondary and non-secondary prevention group in the online supplementary table 1. Briefly, hs-cTnT significantly improved reclassification regarding all endpoints in the overall population and in the secondary prevention cohort. In non-secondary prevention, hs-cTnT improved reclassification only for ACM.
Supplementary file 4
We found no statistically significant difference of hs-cTnT concentrations in men compared with women regarding all endpoints (ACM: men: 49.2±95.1 ng/L, women: 26.0±20.3 ng/L, p=NS; ACM, AMI, stroke: men: 30.0±65.6, women: 16.8±19.1, p=NS; ACM, AMI, stroke, rehospitalisation for ACS or DHF: men: 23.4±44.7, women: 8.7±7.4, p=NS).
Discussion
Our study provides several important findings and supports the significant predictive role of hs-cTnT for risk stratification of patients with stable CAD. First, hs-cTnT outperformed the multivariable ESC-SCORE for the prediction of ACM in non-secondary as well as in secondary prevention. Second, hs-cTnT provides reliable prognostic information on composite endpoints that also include soft outcome measures like readmission with ACS or DHF. Third, hs-cTnT provided consistent prognostic information in an external cohort with a different baseline risk.
We decided to compare the prognostication of hs-cTnT to the ESC-SCORE because it is validated in a large cohort across different countries for the occurrence of CV mortality as an objective and robust endpoint14 and is therefore recommended by ESC guidelines.15 The high prognostic performance of hs-cTnT in stable CV disease has been reported in many studies including large multicenter trials like the PEACE9 or the HOPE study.10
Our group had recently reported about the strong independent predictive value of hs-cTnT in the same low risk cohort of asymptomatic or stable patients with a broad spectrum of CV diseases visiting an outpatient clinic for routine regular check-ups.21 In another recently published analysis, we reported on the performance of hs-cTnT compared with established multivariable scores that are used in some European regions (Prospective Cardiovascular Münster Study (PROCAM) Score) or in the US (Framingham Scores) in primary prevention.33 In consistency with the both previous studies, hs-cTnT predicted ACM with an AUC of 0.878 and thus—as expected—significantly better than the ESC-SCORE in secondary prevention. To our surprise, hs-cTnT also performed significantly better in non-secondary prevention, which is the domain of CV risk scores including the ESC-SCORE. Although our findings need to be confirmed in larger prospective cohorts, our results provide a strong hypothesis generating finding that could improve adoption of risk stratification tools both in primary and secondary prevention. For the latter, there is no universally established risk stratification tool that allows risk estimation after the subacute phase of ACS or after diagnosis of a relevant CV or cerebrovascular disease manifestation.
Although the ESC-SCORE has not been validated for soft endpoints such as rehospitalisation for DHF, AMI or recurrent ACS, we compared the prognostic information incorporated in a single hs-cTnT value as compared with a multivariable score and consistently confirmed our findings on the role of hs-cTnT to predict ACM. In agreement with the previous findings6 34 35 and our own published work on this low risk cohort,21 the prognostic performance of hs-cTnT to predict a variety of softer endpoints than ACM was only moderate with an AUC of only 0.707 for the composite endpoint of ACM, AMI and stroke, and 0.671 for the combined endpoint of ACM, AMI, stroke and rehospitalisation for DHF or ACS. Our results using traditional C-statistics were substantiated by reclassification analyses including continuous and categorical NRI as well as IDI.
A general shortcoming of CV risk scores is that their predictive performance strongly depends on the similarity of the population in which they are applied to the original derivation cohort. An impaired performance has been reported particularly when the baseline risk differs from the original population.36–38 European guidelines therefore recommend the use of national recalibrations of the ESC-SCORE that consider the general population’s risk.15 Nevertheless, this score has not been evaluated in non-caucasian populations and predicts only the endpoint 10-year CV mortality.14 In contrast, the predictive ability of hs-cTnT is more consistent showing an excellent performance across a broad spectrum of stable or asymptomatic patients including low-risk cohorts,39–41 chronic heart failure,42 asymptomatic high risk patients10 and in the general population.7 8 Since risk scores are only rarely used in daily clinical practice,16 17 the use of hs-cTnT within a single-biomarker strategy may facilitate the prognostication of low-risk patients and increase the acceptance of risk stratification in daily practice. Nevertheless, although higher hs-cTnT values have been associated with an increased risk for CV endpoints, it may not be directly modified by lifestyle changes in contrast to some of the variables of the ESC-SCORE like hypertension or smoking status.
Our results were validated in a large independent study cohort of 2046 stable patients with documented coronary anatomy from the EXCELSIOR trial.22 In the EXCELSIOR cohort, a lower prognostic performance of hs-cTnT for the prediction of ACM as compared with our study cohort was found (AUC 0.759, 95% CI 0.740 to 0.777 vs AUC 0.878 95% CI0.805 to 0.950). A reason for this observation might be the higher baseline risk since all individuals of the EXCELSIOR cohort underwent coronary angiography. Furthermore, the annual mortality was more than twice as high compared with our cohort (2.1 vs 0.9%). Irrespective of the higher baseline risk, hs-cTnT also outperformed the ESC-SCORE in the prediction of ACM and non-fatal AMI in the EXCELSIOR trial. The use of hs-cTnT in addition to the ESC-SCORE could significantly improve risk classification of patients. Multiple subgroup analyses of this cohort demonstrated that this finding was consistent throughout the whole population of this study. We therefore assume that our results may also be applied to other cohorts including populations at higher baseline risk.
In conclusion, our study suggests that hs-cTnT is a reliable and convenient risk predictor with a superior performance compared with the ESC-SCORE in non-secondary and secondary prevention that may be applied in a broad spectrum of patients in primary care. It is thereby easier and more convenient to use in daily clinical practice.
Limitations
The findings of this registry are limited by a relatively small sample size and small event rates, particularly occurrence of few all-cause deaths. However, our findings are consistent with the previous findings across the spectrum of stable CV disease and plausible due to the comprehensive integration of different pathophysiological aspects reflected by elevated cardiac troponin in blood. Our findings were validated in an independent large registry consistently confirming our results. Nevertheless, we believe that our results are hypothesis generating and would benefit from additional external validation in prospective trials or registries. Furthermore, there is large controversy regarding the role of sex-specific cut-offs that are being recommended by the Universal Myocardial Infarction Definition Task Force.1 Currently, sex-specific cut-offs have neither been recommended by ESC guidelines nor have they been validated prospectively. In the absence of convincing data supporting an improvement of diagnostic and prognostic reclassification,43 we preferred to use a single, sex-independent cut-off at the 99th percentile of a healthy reference population.26
Acknowledgments
We thank Mrs Heidi Deigentasch, Mrs Melanie Hütter, Mrs Elisabeth Mertz and Mrs Monika Arnold for their valuable support regarding data management and follow-up.
References
Footnotes
Contributors All authors contributed to the manuscript.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Ethics approval Ethics Committee, University Hospital Heidelberg.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.