Article Text

Abstract
Objective Atrial dilation is known to be a poor prognostic indicator. However, its clinical, functional and prognostic implications have not been thoroughly explored in secondary mitral regurgitation (SMR). We sought to describe the implications of severe atrial dilation (SAD) in SMR.
Methods We included all adult patients with severe SMR due to left ventricle dysfunction (with no organic mitral valve disease) who underwent transthoracic echocardiography between January 2012 and March 2021 at our institution. The concomitant presence of severe left atrial (LA) dilation (>48 mL/m2) defined SADMR (SAD in SMR), and these patients were compared with those without SAD.
Results A total of 2011 patients were included (mean age 70% and 41% females), with 71% having SADMR. MR severity and ejection fraction were similar between both groups. Patients with SADMR were older, less females and had more diabetes, but similar rates of atrial fibrillation. Mechanistically, they had lower A wave velocity (0.61 vs 0.72 cm/sec, p<0.001) and more impaired LA reservoir strain (9.7% vs 15.5%, p<0.001). Geometrically, SADMR had shallower leaflets’ angulations, lower tenting height, larger annuli and smaller leaflet length/annular diameter ratios (all p<0.001). They underwent fewer MV interventions, although these were associated with better outcomes (log-rank p<0.001). Over the study period, SAD was an independent predictor of mortality (HR 1.26, p=0.04).
Conclusion SADMR is associated with specific mechanistic and functional alterations and confers a worse prognosis.
- mitral valve insufficiency
- echocardiography
- outcome assessment, health care
Data availability statement
No data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Atrial dilation is a known predictor of poor outcomes in a myriad of cardiovascular diseases, and had been thoroughly studied in primary mitral regurgitation.
What does this study add?
Severe atrial dilation implies geometrical alterations of the mitral valve in ventricular secondary mitral regurgitation, and is correlated with worse clinical outcomes and mitral valve interventions, despite positive impact of these interventions on overall mortality.
How might this impact on clinical practice?
Invasive and/or medical treatment of patients with secondary mitral regurgitation prior to the onset of severe atriald dilation, may potentially extend overall survival of these patients.
Introduction
Mitral regurgitation (MR) is very common, affecting 22% of people over 65 years with a 2.3% prevalence of significant (moderate/severe) disease.1 2 It is classically categorised as either primary when driven by valvular pathology, or secondary MR (SMR) when due to left ventricle (LV) dysfunction.3–5 The regurgitant MR jet leads to left atrial (LA) volume overload which, over time, can lead to LA remodelling and severe atrial dilation (SAD). SAD has been previously shown to be predictive of adverse outcomes in patients with primary MR.6–8 However, its clinical and prognostic implications, in addition to the mitral apparatus’ functional/geometric alterations that occur with SAD, have not been explored in SMR. With the increasing number of mitral transcatheter technologies,9 10 such information may be useful in patient selection, device choice and timing of intervention.
We sought to define and describe the prevalence, clinical and echocardiographic characteristics of patients with SAD in the setting of severe SMR (SADMR) and explore the therapeutic and prognostic implications.
Methods
Patient population
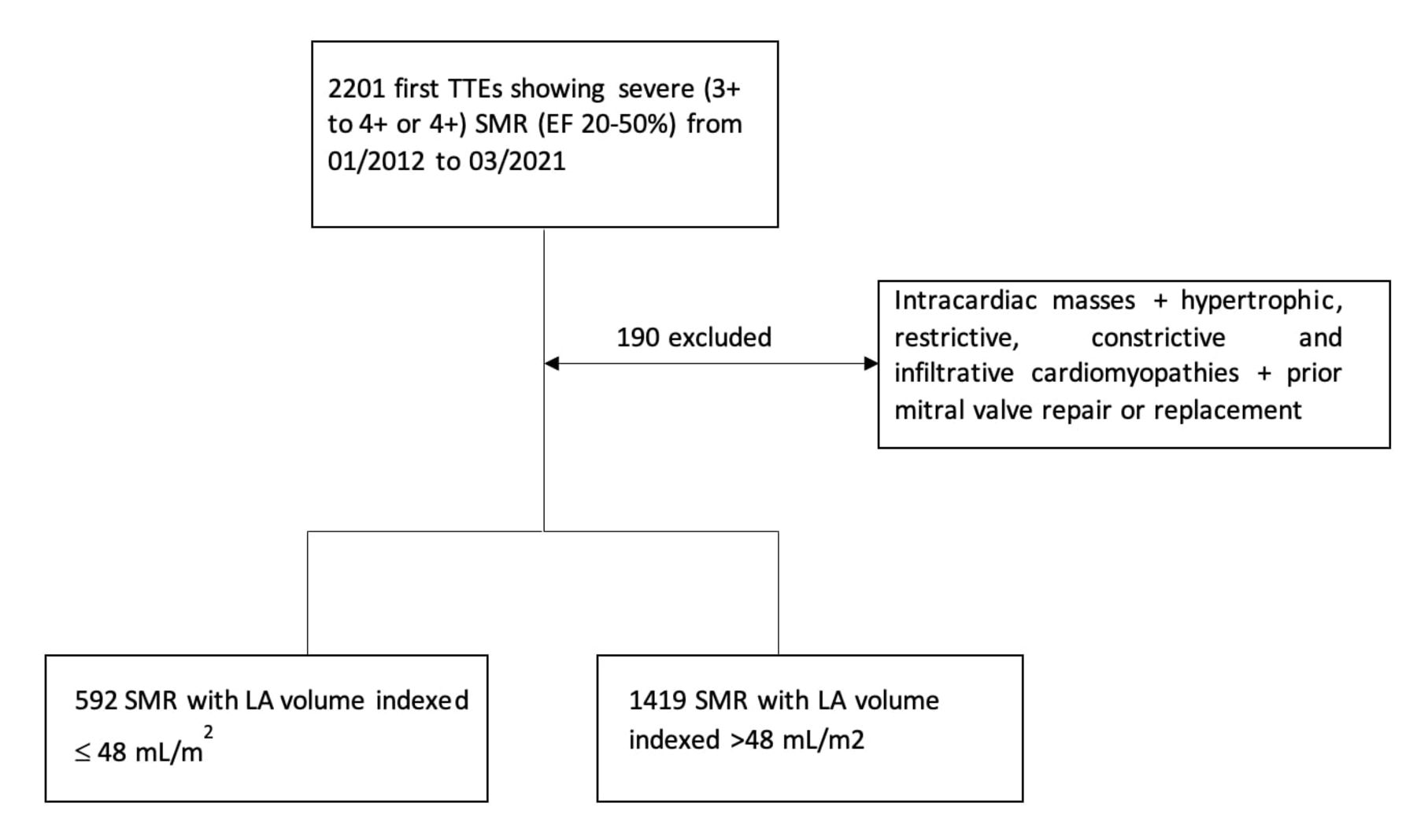
All adult patients (≥18 years old) who underwent transthoracic echocardiography (TTE) at the Cleveland Clinic from January 2012 to March 2021 were screened. We included the first TTE showing severe SMR, defined as 3+to 4+or 4+MR with a left ventricular ejection fraction (LVEF) of 20% to 50% in the absence of leaflet pathology (flail, endocarditis, prolapse, rheumatic and calcific mitral valve disease). We excluded patients with intracardiac masses (thrombus, vegetation, tumour), hypertrophic, restrictive, constrictive and infiltrative cardiomyopathies, and patients with prior mitral valve repair or replacement.11 Also, a minimum of 1 month of follow-up was required for inclusion. Based on the degree of concomitant LA enlargement, the 2011 remaining patients were divided into two: (1) those with SADMR, defined as SMR with severe LA dilation (ie, indexed LA volume >48 mL/m2 according to the American Society of Echocardiography (ASE) guidelines12) and (2) those without SADMR, defined by SMR with non-severe LA dilation (ie, LA volume indexed ≤48 mL/m2) (figure 1).

Study flow chart of the patient population. EF, ejection fraction; LA, left ventricle; SMR, secondary mitral regurgitation; TTEs, transthoracic echocardiography.
Clinical data
Clinical variables were collected by chart review and included age, sex, body mass index (BMI), New York Heart Association (NYHA) class, medications and comorbidities (hypertension, hyperlipidaemia, coronary artery disease, diabetes and atrial fibrillation/flutter) at time of TTE.
Echocardiography
Standard TTE examinations were performed and interpreted by experienced cardiologists in compliance with the guidelines.13 14 The severity of MR was graded using a multiparametric approach as advocated by the ASE, including calculating the effective regurgitant orifice area (EROA) using the proximal iso-velocity surface area method. Concomitant tricuspid valve regurgitation (TR) was noted. Cardiac chambers’ size and function were also quantified by standard ASE recommendations.12 The systolic pulmonary arterial pressure (SPAP) was estimated based on the TR jet maximum velocity and the estimated right atrial pressure.15 As for diastology data, tissue Doppler and pulse wave Doppler were obtained according to guidelines,16 and the following variables were recorded: E wave, A wave (in patients with sinus rhythm), the average of lateral and medial E/e’ ratios, and the MV deceleration time.
Strain and mitral valve geometrical measurements
LA and LV strains were not routinely reported. Therefore, we performed manual strain analysis on matched samples from both groups. For that purpose, 200 patients with SADMR were randomly chosen, and then 200 patients without SADMR were matched using a propensity score based on age, sex, and BMI with a 1:1 ratio to the nearest neighbour (calibre of 0.1 on a scale of 0–100) (online supplemental table 1). For further adjustments to LV end-diastolic volume (LVEDV) and LV end-systolic volume (LVESV), we employed a second propensity score matching model including age, sex, body surface area (BSA), LVEDV and LVESV (online supplemental table 2).
Supplemental material
We performed an offline analysis of speckle tracking echocardiography using Velocity Vector Imaging (2.0; Siemens, Erlangen, Germany) on both groups. To measure the LA longitudinal reservoir strain function, we used the QRS complex (end-diastole) as the zero reference. The LA strain curve’s peak systolic values from the apical four-chamber and two-chamber views were averaged. For the LV global longitudinal strain (LVGLS), the endocardial borders were automatically tracked throughout the cardiac cycle and adjusted manually where required.
Using the same samples of 200 patients each, we also compared the following MV anatomic features measured on an apical three-chamber view: anteroposterior annular diameter, anterior and posterior leaflet angles, leaflet length/annular diameter ratio, and tenting height. To adjust for LV volumes, we compared the same variables on a second propensity score matching model based on age, sex, BSA, LVEDV and LVESV.
Follow-up
Patients were followed for the occurrence of mitral valve interventions including surgeries (repair or replacement) or transcutaneous edge-to-edge repair (TEER), and LV assistance device (LVAD) implantation or heart transplantation. We also recorded electrophysiology arrhythmias ablations, pacemaker and intracardiac defibrillator implantations, and LA appendage occlusion procedures.
Endpoints
The primary outcome was defined as all-cause mortality. To control for interfering interventions, patients who underwent mitral valve surgeries or TEER, LVAD or heart transplantation were excluded from the survival analysis. In addition, for those who had TEER, we defined significant residual MR as >2+ on the postprocedural TTE17 and compared its occurrence between both SMR groups.
Statistical analysis
Categorical variables are presented as percentages, whereas continuous variables are presented as mean with SD in case of a normal distribution and median with the IQR when not normally distributed. Categorical variables are compared using Pearson’s χ2 test for independence, and continuous variables are compared using the Student’s t-test or Mann-Whitney U test, as appropriate. Time-to-event analysis was performed using the Kaplan-Meier survival method. To test whether SAD was an independent predictor of mortality, we employed a cox proportional-hazard model that included age, sex, and the echocardiographic parameters that significantly predicted mortality on univariable analysis. The LA volume as a continuous variable violated the proportional hazards assumption so it was not explored. All analyses were conducted using SPSS V.23.0 (IBM) and R studio V.1.4.1717 (R Foundation for Statistical Computing, Vienna, Austria).
Patient and public involvement
No participants were involved in the design, conduct, reporting, or dissemination plans of the research question or outcome measures.
Results
Baseline patients’ characteristics
Of the total cohort, 1419 patients (70.6%) had SADMR while the remaining 592 patients (29.4%) did not have concomitant SAD (figure 1). Patients’ clinical characteristics are summarised in table 1. Patients with SADMR were older (70.4 vs 68.2 years, p<0.01), had lower BMI (27.7 vs 29.3, p=0.01), and were less likely females (38% vs 48%, p<0.001). Both groups had similar comorbidities including atrial fibrillation (63% vs 66%, p=0.24). However, diabetes was more frequent in the SADMR group (40% vs 35%, p=0.04). There were no differences in the NYHA classes between both groups.
Baseline patients’ clinical characteristics
On TTE, both groups had similar EF (33.1%±9.1 vs 33.5%±9.3, p=0.34), though LV volumes were larger in the SADMR group (191.5 vs 160.4 mL p<0.001 for end-diastolic volumes and 130.4 vs 108.2 mL for end-systolic volumes, p<0.001). In terms of MR severity, both groups had similar EROA (41.9±24.7 mm2 vs 41.2±29.4 mm2, p=0.63). Also, the peak and mean MV gradients and maximum velocity of the MR jet (Vmax) were comparable (table 2). However, patients with SADMR had higher estimated SPAP (52 vs 49 mm Hg, p=0.001) and more frequent moderate/severe RV dilation and moderate or more TR (40% vs 29% p<0.001% and 63% vs 51% p<0.001, respectively).
Baseline echocardiographic parameters
In terms of diastology (table 2), the measured parameters were comparable, except for the peak A wave which was lower in the SADMR group (0.61 vs 0.72 cm/s p<0.001). Also, strain analysis (table 3) showed significantly lower LA strain in the SADMR group (9.71% vs 15.51%, p<0.001), with similar LVGLS (-6.26 vs −6.86 p=0.14). Geometrically, SADMR had larger mitral valve annulus (2.18 vs 1.84 cm p<0.001), shallower anterior and posterior leaflet angles (28.51° vs 41.19° and 30.64° vs 41.54°, respectively, both p<0.001), smaller anterior and posterior leaflets to annulus ratio (0.58 vs 0.67 and 0.58 vs 0.66, respectively, p<0.001), and lower tenting height (1.14 vs 1.55 cm, p<0.001). Similar results were also found after adjusting for LVEDV and LVESV (online supplemental table 2). On subgroup analysis, patients with or without atrial fibrillation, and with ischaemic versus non-ischaemic cardiomyopathy, had similar mitral valve measurements and LA and LV strain (online supplemental tables 3 and 4). In contrast, patients in the SADMR group with an EF ≥40% had lower tenting height, anterior and posterior angles (online supplemental table 5).
Strain analysis and mitral valve anatomic features
Interventions and outcomes
The median follow-up was 13 months (IQR 2.4–39 months). SAD patients underwent less mitral interventions (20% vs 23% p=0.04) but more LVAD and/or heart transplantation (6% vs 3% p=0.003). Other interventions were similar between both groups (table 4).
Cardiac interventions during follow-up
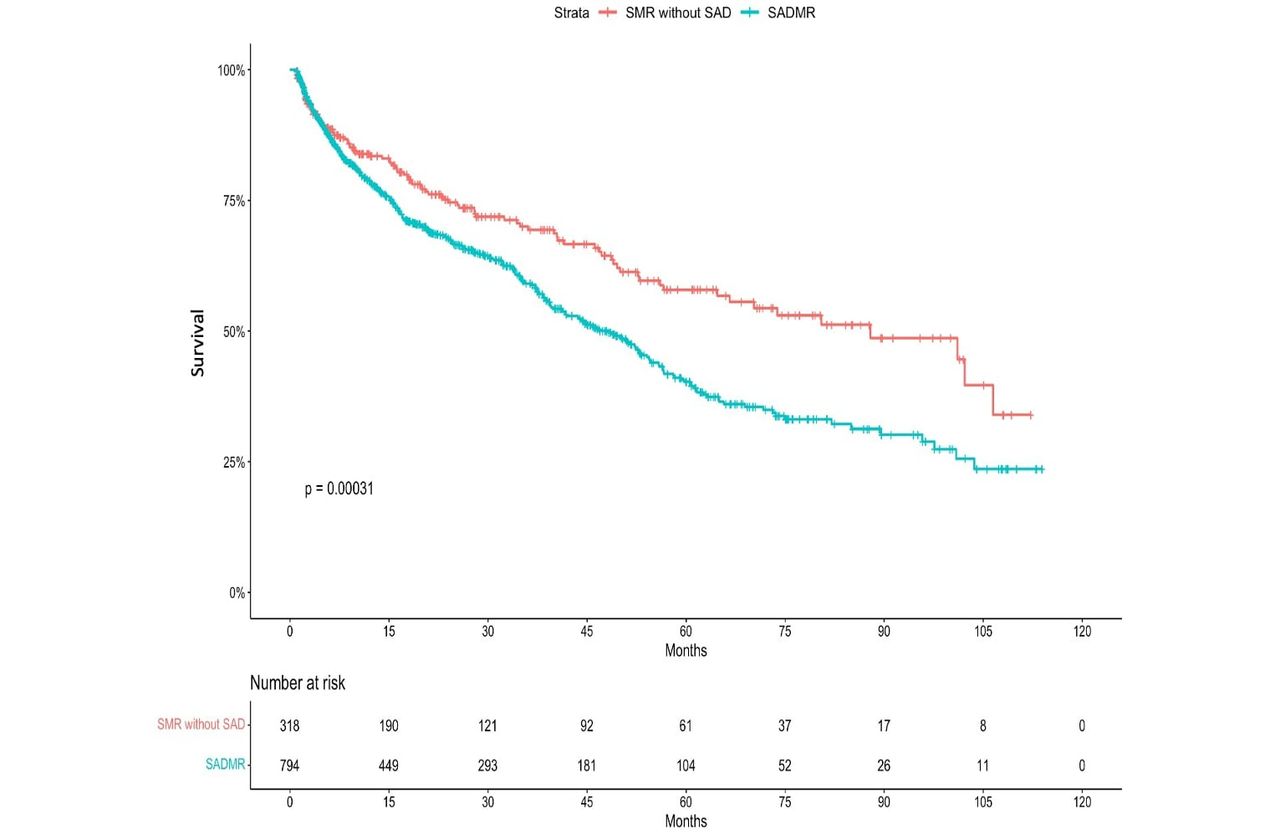
In terms of the primary outcome, there were more deaths in the SADMR group (50% vs 43%, p=0.004). On multivariable Cox regression analysis, SAD and SPAP were the only variables that were independently associated with mortality (HR 1.26 p=0.04 and HR 1.01 p<0.001, respectively) (table 5). On Kaplan-Meier survival analyses, patients with SADMR had significantly worse survival (figure 2). However, on subgroup analysis, patients with SADMR who underwent mitral interventions (surgical or TEER) had improved outcomes (age and gender adjusted log-rank p<0.001) (figure 3).
All-cause mortality: univariate and multivariable Cox regression analysis

Kaplan-Meier curves for the association of SADMR versus SMR without SAD with all-cause mortality. SAD, severe atrial dilation; SMR, secondary mitral regurgitation.

Kaplan-Meier curves for the association of mitral valve (MV) interventions with all-cause mortality in patients with SADMR. SADMR, severe atrial dilation mitral regurgitation.
Regarding TEER results, of the 43 patients that underwent the procedure, 14% had significant residual MR, which was not associated with the SADMR or the measured geometrical parameters (online supplemental table 6).
Discussion
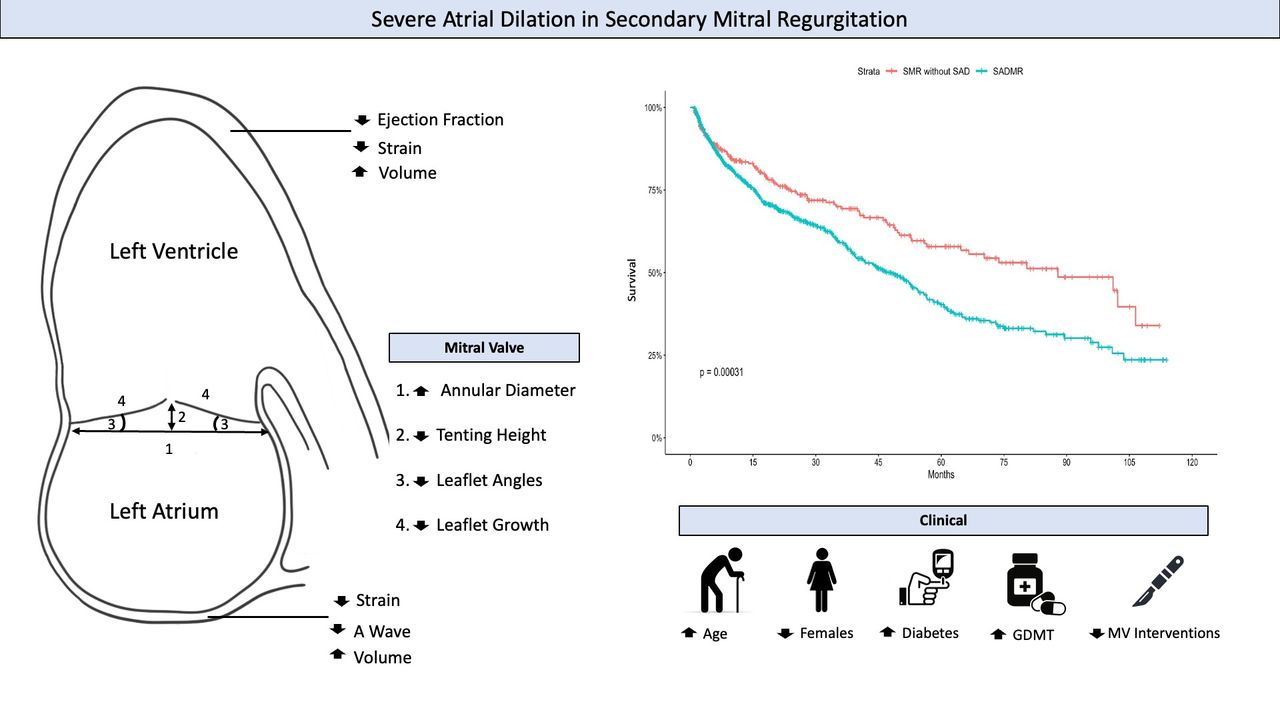
There are multiple key observations from this study. SAD is present in 70.6% of patients with severe SMR and, when present, it is associated with specific mechanistic and geometrical alterations, limited therapeutic options and worse outcomes (figure 4). Previous studies established the negative prognostic value of atrial enlargement in primary MR.6–8 Although SAD is frequently present in chronic SMR and could reflect its severity and longer duration, the ensuing mitral geometrical alterations and the clinical, therapeutic and prognostic implications have not been previously explored. Our findings of distinct functional and anatomic alterations along with divergences in the management and outcomes, for the same degree of MR and LV function, suggest that this subgroup of SMR patients may need to be considered separately. Specifically, we found SADMR, compared with SMR without SAD, has distinctive geometrical changes (larger annular size, and shallower leaflets angulations and tenting), and more pronounced LA dysfunction (lower A waves and LA strain). In addition, the management options were more limited, with less referral for mitral interventions, and the outcome was worse.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Anatomical, mechanistic and clinical insights into severe atrial dilation in SMR. GDMT, guideline directed medical therapy; MV, mitral valve; SAD, severe atrial dilation; SMR, secondary mitral regurgitation.
Mechanistically, patients with SADMR had significantly lower A wave velocity on diastology and lower LA strain (though with similar LVGLS), supporting the hypothesis of significant coexisting LA myopathy superimposed on the LV cardiomyopathy. LA dysfunction in patients with heart failure is associated with a higher risk of developing atrial fibrillation.18 Interestingly, in our study, there were no significant differences in the prevalence of atrial fibrillation between both groups; However, a time-to-event analysis could be necessary to sense the difference in the onset of new atrial fibrillation. Nevertheless, type 2 diabetes was more common in SADMR and prior studies have shown an association between diabetes and atrial dysfunction.19
From a geometrical perspective, the lower tenting height, shallower leaflet angulations, larger annulus and smaller leaflets to annulus ratio in SADMR suggest a dual interaction—both ventricular and atrial.20 From one side, ventricular dysfunction/enlargement leads to apical tethering of the leaflets with increased tenting, as has been typically described in ventricular SMR.3 21 On the other side, the concomitant presence of SAD is associated with outward annular stretching and flattening of the leaflets as has been described with atrial SMR.22–24 Our findings support an additive effect whereby the leaflets are tethered by the ventricular component but to a lesser extent due to the atrial component. While annular dilation is a key component of both ASMR and VSMR,3 25 26 our study shows that SADMR is associated with an even greater annular dilation.
From a management standpoint, both groups had high utilisation rates of guideline directed medical therapy (GDMT) with overall relatively low referrals for advanced heart failure therapies, in concordance with recently reported literature.11 27 Interestingly, mitral interventions, both surgical and percutaneous, were less frequent in the SADMR group despite the association with improved outcomes. This may be due to the older population and the severity of LA enlargement. However, our findings suggest that SADMR may still benefit from mitral interventions. This is in concordance with the recent subanalysis of the COAPT trial showing markedly improved survival in patients with SMR and atrial fibrillation undergoing TEER, with similar effect of intervention as patients without atrial fibrillation.20 Similarly, in our study, significant residual MR was not different between both groups suggesting that the degree of LA enlargement should not deter from intervening.
In terms of prognosis, the SADMR group had worse survival and the concomitant presence of atrial dilation in SMR was found to be an independent predictor of mortality. While this finding is relatively novel for SMR, it is not unexpected given the preponderance of data suggesting that LA enlargement is a marker of worse outcomes across the spectrum of cardiac disorders.28
Study limitations
There are multiple limitations to our study. First, this is a retrospective single-centre observational study with all the inherent limitations including lack of causality and external validity. Second, the dynamic nature of SMR is well established29 with its severity being variable with loading conditions and medical therapy. However, the high rates of GDMT utilisation in our study suggest that this may not have been impactful on our findings. Third, SMR and heart failure are progressive diseases over time, and SADMR patients might have been exposed to a longer duration of the disease which could be impactful on outcomes. Lastly, patients lost to follow-up may affect our study results. We tried to mitigate this risk by excluding patients who came for one visit or did not have a follow-up beyond 1 month from inclusion.
Conclusion
For the same degree of MR and severity of LV dysfunction, SAD in the setting of severe SMR is associated with distinct mechanistic and geometrical alterations, fewer referrals for mitral interventions and worse outcomes.
Data availability statement
No data are available.
Ethics statements
Patient consent for publication
Ethics approval
The institutional review board of Cleveland Clinic approved this study (21-603).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors HL, AM and SCH conceived and designed the study; HL, EA, AM and SCH collected, analysed, and interpreted the data; HL, EA, AM, MM, CK and SCH drafted and critically revised the manuscript; RD; JR, DB, AMG, SB, RP, PC, BG, SK and SCH supervised the study; HL and SCH are responsible for the overall content and serve as guarantors. All authors read and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.