Article Text

Abstract
Background Several studies have demonstrated that complete revascularisation improves clinical outcomes in patients with ST-segment elevation myocardial infarction (STEMI) and multivessel coronary disease. However, the optimal timing of non-culprit lesion revascularisation remains controversial.
Objective The aim of this systematic review and meta-analysis was to assess the effect of timing of complete revascularisation on cardiovascular outcomes in patients with STEMI and multivessel coronary artery disease.
Methods Searches of PubMed, the Cochrane Library, ClinicalTrials.gov and the reference lists of relevant papers were conducted covering the period from 2004 to 2019. A pairwise analysis was performed to compare the difference in clinical outcome between early complete revascularisation (index procedure or index hospitalisation) and delayed complete revascularisation (after discharge) in patients with STEMI.
The primary endpoint was the incidence of major adverse cardiac events (MACE), which was defined as the composite of all-cause mortality, recurrent myocardial infarction, unplanned repeated revascularisation and cardiovascular death.
Results Twelve studies including a total of 7596 patients were identified. The MACE rate was 10.37% in early complete revascularisation compared with 18.17% in culprit only (p=0.01). When complete revascularisation was delayed, the MACE rate was 11.81% after complete revascularisation compared with 17.21% in culprit-only percutaneous coronary intervention (PCI) (p=0.01). A meta-regression analysis demonstrated no relationship between timing of complete revascularisation and reduction in MACE relative to culprit-only PCI (p=0.862).
Conclusion In patients with STEMI treated by primary PCI and multivessel disease, there is a benefit of complete revascularisation over culprit-only PCI whether non-culprit revascularisation is performed early in hospital or delayed as an elective procedure. We have not demonstrated a relationship between timing of complete revascularisation and MACE.
PROSPERO registration number CRD42021226789.
- Cardiac Catheterization
- Myocardial Infarction
- Percutaneous Coronary Intervention
Data availability statement
All data relevant to the study are included in the article or uploaded as supplemental information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
The optimal timing of non-culprit lesion revascularisation is still controversial among patients presented with ST-segment elevation myocardial infarction (STEMI) and residual lesions after culprit revascularisation, so our systematic review and meta-analysis was designed to assess the effect of timing of complete revascularisation on major cardiovascular events.
WHAT THIS STUDY ADDS
The main finding was that early complete revascularisation (index procedure or index hospitalisation) has no significant difference regarding clinical outcomes, but may be favoured in comparison with delayed complete revascularisation (after discharge) and regardless of time, the clinical outcome is better than culprit lesion-only percutaneous coronary intervention (PCI) in patients with STEMI.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE AND/OR POLICY
We can assume that our paper will have a great impact on the clinical practice and will contribute significantly to the advancement of research in the field.
Introduction
Primary percutaneous coronary intervention (PPCI) is the gold standard treatment for ST-segment elevation myocardial infarction (STEMI). Multivessel disease is present in ~50% of patients presenting with STEMI and associated with less ST-segment resolution after PPCI and higher 1-year mortality, with a direct proportionality to coronary artery disease extent in non-culprit vessels.1 The presence of multivessel disease is associated with worse outcomes relative to single-vessel disease and features of plaque vulnerability are often present. Additionally, atherosclerotic non-culprit plaques may harbour features of vulnerability associated with recurrent atherothrombosis.2
Several randomised trials have demonstrated superior clinical outcomes including cardiovascular death and myocardial infarction with complete revascularisation rather than culprit vessel-only strategy.3 However, the optimal timing of complete revascularisation between index PCI, staged PCI before hospital discharge (early) and staged PCI after discharge (delayed) remains controversial.4
The objective of this systematic review is to identify studies involving complete revascularisation in the setting of STEMI and to compare clinical outcomes associated with different intervals from presentation to complete revascularisation.
Methods
The present systematic review and meta-analysis was performed in accordance with the Cochrane Handbook for Systematic Reviews and Interventions.
Analysis is reported following the Preferred Reporting Items for Systematic Reviews and Meta-analyses statement in healthcare interventions.5
Search strategy
Searches of PubMed, Google Scholar, Cochrane library, EMBASE and ClinicalTrials.gov, and the reference lists of relevant papers were performed between the years 2004 and 2019.
The following keywords and MeSH terms were used in the searches: “ST-segment elevation myocardial infarction” or “STEMI”, “Complete” or “Non-culprit artery” or “Multivessel”, “Culprit artery” or “Target vessel” or “Infarct related artery” or “IRA” and “Revascularization” or “Percutaneous coronary intervention” or “PCI”.
This meta-analysis was registered at the PROSPERO international prospective register of systematic reviews (Multi-Vessel or Culprit-Only Revascularization in Patients with Multi-Vessel Coronary Artery Disease Undergoing Percutaneous Coronary Intervention; CRD42021226789).
Study selection and eligibility criteria
Two reviewers independently screened the studies including the following:
Patients presented with STEMI and multivessel disease.
Studies comparing complete revascularisation versus culprit lesion-only PCI.
Studies demonstrating specific time/range for complete revascularisation procedure (index procedure or index hospitalisation, or delayed after discharge).
Studies reporting the outcomes of major adverse cardiac events (MACE), all-cause mortality, recurrent myocardial infarction, repeat revascularisation and cardiovascular death.
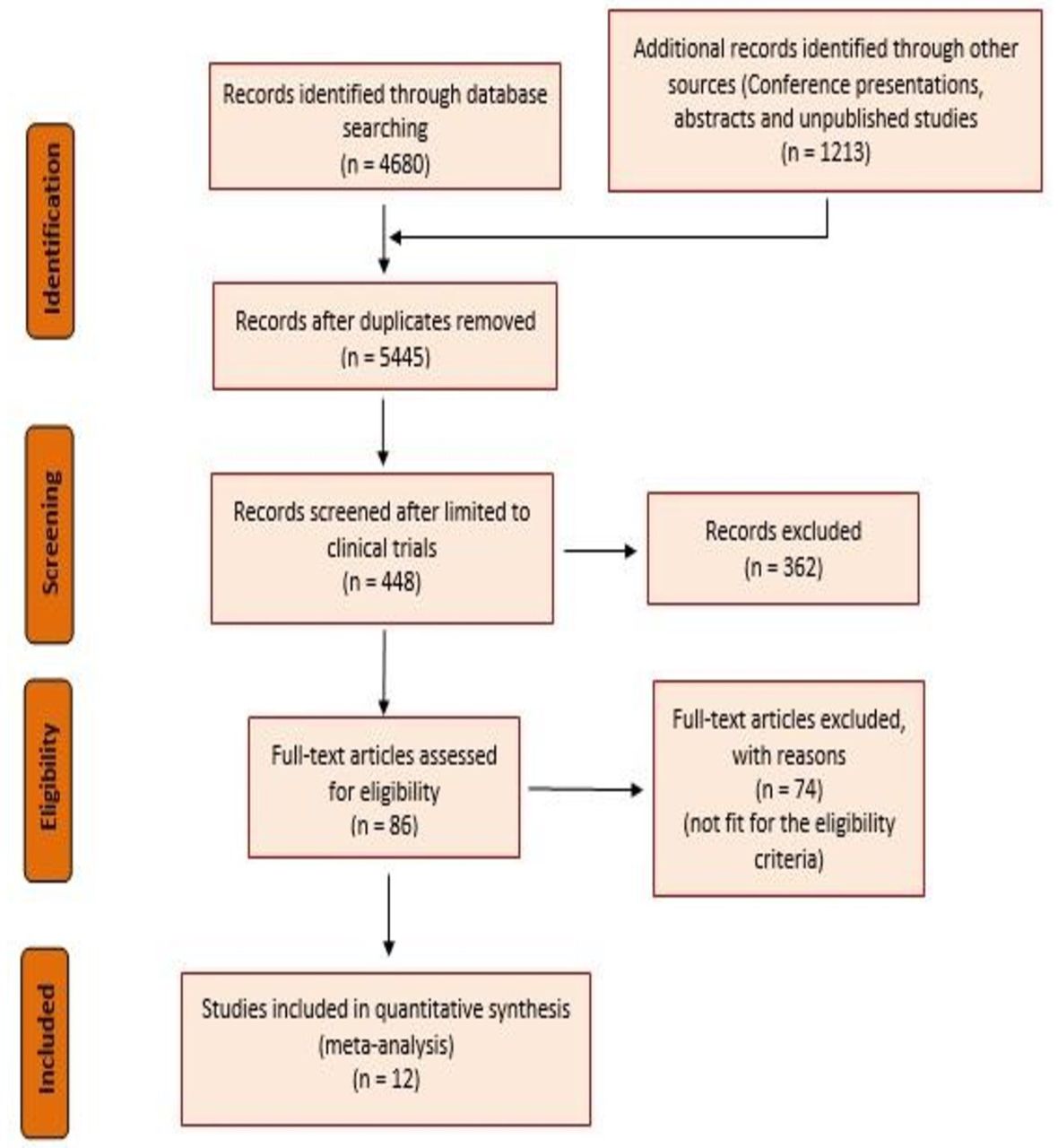
Studies enrolling patients with a diagnosis other than STEMI or comparing revascularisation strategies other than PCI or trials that solely reported non-clinical outcomes were excluded. Non-randomised controlled trials (RCTs), case reports, editorials, comments, letters, academic conferences and review articles were also excluded from the analysis. A flow chart detailing the literature search and screening process is provided in figure 1.

Search strategy and study selection.
Data extraction and quality assessment
We developed a data extraction sheet that was subsequently used by two of our authors who independently extracted the following data from the studies included: study name, year, design, number of populations, demographic data (age and gender), risk factors (hypertension, diabetes mellitus, dyslipidaemia, smoking), procedure data (number of affected vessels, culprit vessel, number of vessels revascularised, stent type), time of complete revascularisation, follow-up duration and indicators and clinical outcomes.
In the selected studies, the patients were allocated randomly to a group for complete revascularisation of culprit and non-culprit lesions in the same index procedure or in a second procedure just pre-discharge and another group for culprit lesion-only PCI during the index procedure followed by complete revascularisation of the non-culprit lesions after patients’ discharge. The decision for patients’ allocation was granted either by the study protocol or according to the clinical decision of the treating physician.
We considered 7 days as cut-off point for early complete revascularisation as in the included studies, the index hospitalisation which includes the PPCI only or PPCI and pre-discharge complete revascularisation was up to 7 days’ length of stay.
Then we divided the patients into two groups:
Group 1: early complete revascularisation (index procedure or index hospitalisation) <7 days.
Group 2: delayed complete revascularisation (after discharge) ≥7 days.
Only RCTs were included in our meta-analysis. The risk of bias for included RCTs was assessed independently by two reviewers using the Cochrane Collaboration’s tool for assessing risk of bias in randomised trials6 (online supplemental figure I and online supplemental figure II).
Supplemental material
Outcomes and data analysis
Information regarding MACE, all-cause mortality, non-fatal myocardial infarction, unplanned/repeat revascularisation and cardiac death was collected. All endpoints were defined according to the definitions used in each trial.
All outcome comparisons were calculated with RevMan V.5.4 (Cochrane Collaboration, Oxford, UK). The summary relative risks (RRs) and ORs with 95% CIs were estimated using Mantel-Haenszel random-effects method. We calculated the I2 statistic to evaluate the percentage of heterogeneity among the trials.
A full meta-analysis random-effects approach to the regression had been used, to explore potential relationship in all included studies between the rate of MACE and the time to complete revascularisation.
Results
Our initial search identified 5893 studies, of which 5445 were identified as duplicates and were removed. Four hundred forty-eight studies were screened and 362 were excluded. Eighty-six studies were included for eligibility, of which 74 were excluded. Only 12 studies were included in the final analysis (figure 1).
Eleven studies were included in the final analysis with a total of 7596 patients. Participants’ mean age was 61.86 years, 74.29% were male. Summary and population characteristics of the selected RCTs are shown in online supplemental table II.
One study by Mehta et al7 reported both early and delayed strategy for complete revascularisation, so it is included in both two groups and comparison analysis.
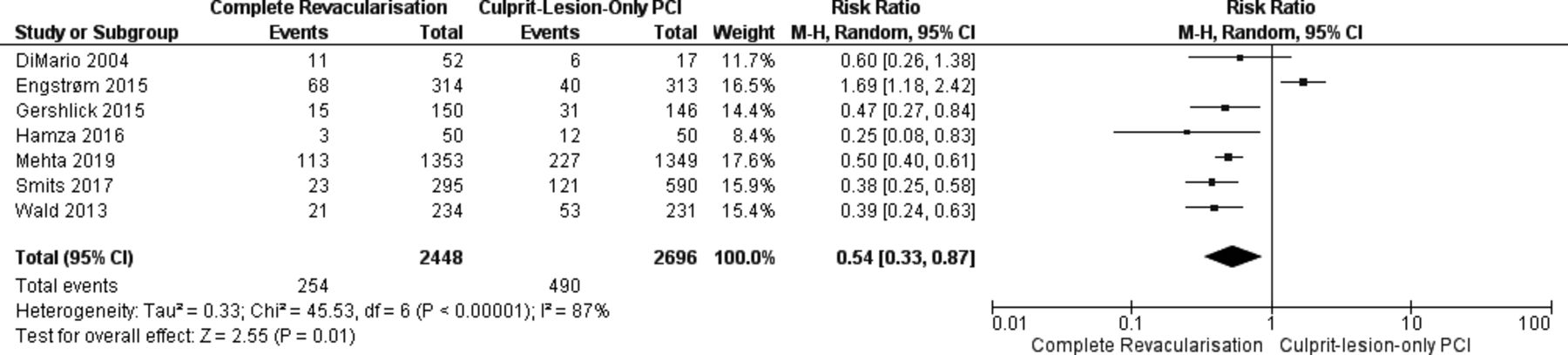
Seven studies with 5144 patients compared the outcome between early complete revascularisation and culprit lesion-only PCI. The mean time was 1.78 days (figure 2).
Forest plot of comparison between early complete revascularisation versus culprit lesion-only PCI.11–14 PCI, percutaneous coronary intervention.
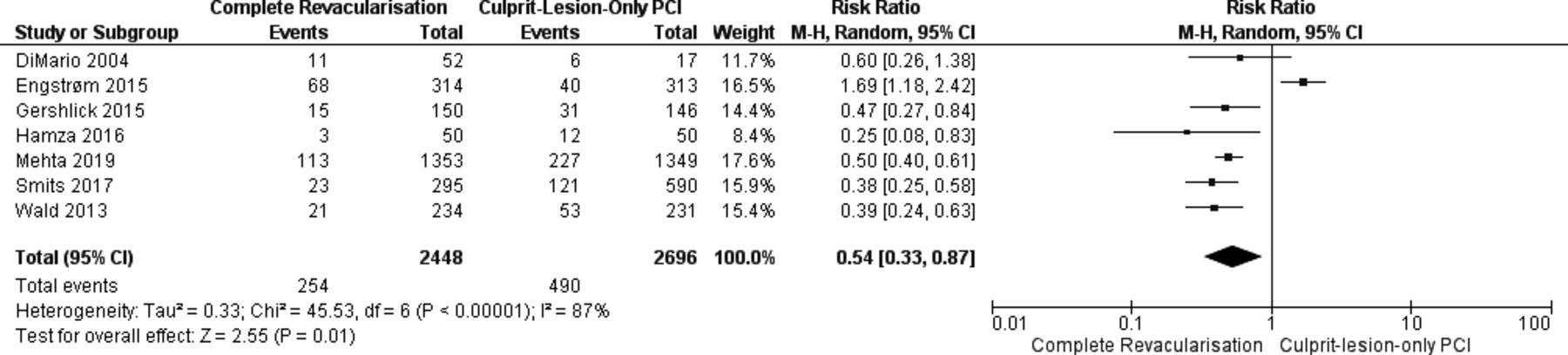
Six studies with 2452 patients compared the outcome between delayed complete revascularisation and culprit lesion-only PCI. The mean time was 18.3 days (figure 3).

Forest plot of comparison between delayed complete revascularisation and culprit lesion-only PCI.15–19 PCI, percutaneous coronary intervention.
The meta-analysis demonstrates significant reduction in the outcome in complete revascularisation versus culprit-only PCI when studies undertaking early complete revascularisation were assessed (RR 0.58 (95% CI 0.35 to 0.95)) and also when we assessed those who undertook delayed complete revascularisation (RR 0.68 (95% CI 0.50 to 0.92)). The event rate was 10.37% in early revascularisation compared with 18.17% in culprit only (p=0.01). The event rate was 11.81% in the complete revascularisation arm in studies in which it was delayed compared with 17.21% in culprit only (p=0.01).
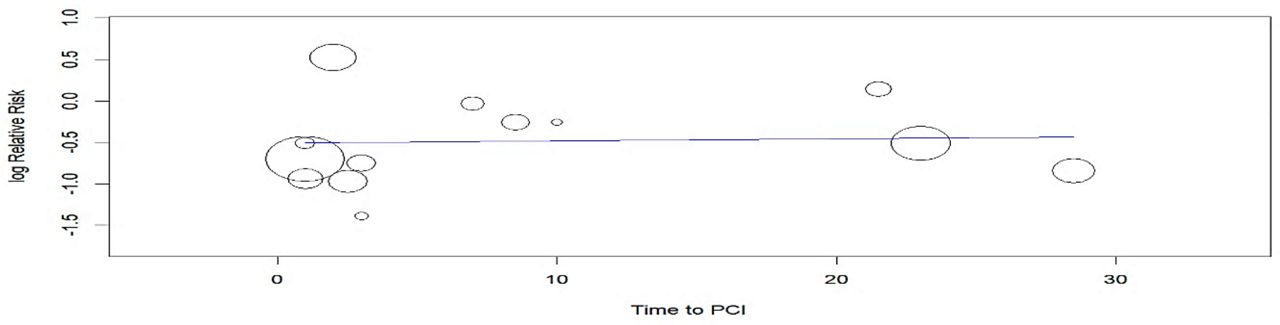
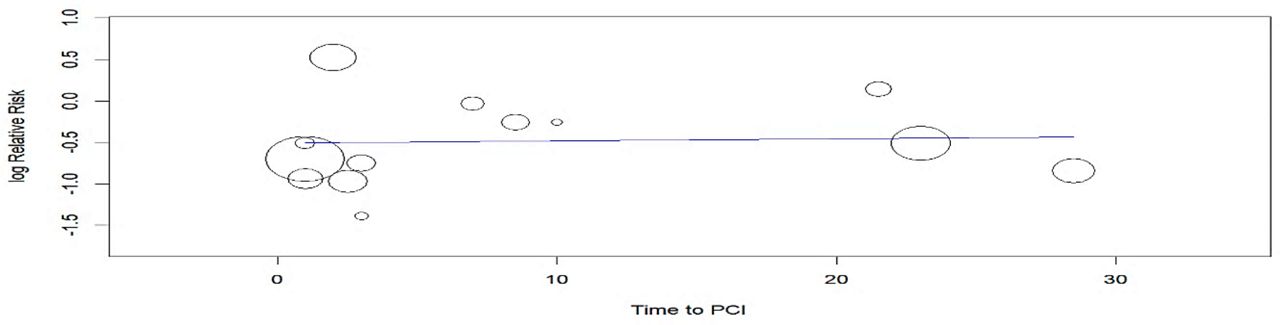
Random-effects meta-regression did not reveal any evidence for an association between the log OR for the MACE rate and the time to complete revascularisation (p=0.58). Each trial is represented by a circle and size is proportional to the sample size of each study (figure 4, table 1).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Regression plot of relation between MACE rate and time to complete revascularisation. MACE, major adverse cardiac events; PCI, percutaneous coronary intervention.
Regression analysis of relation between MACE rate and time to complete revascularisation.
Subgroup analysis
Efficacy of early complete revascularisation versus culprit-only PCI
All-cause mortality
Five studies demonstrated the comparison of all-cause mortality between early complete revascularisation versus culprit lesion-only PCI, and there was no significant effect of early complete revascularisation on all-cause mortality (RR 0.60 (95% CI 0.33 to 1.11) p=0.11) (online supplemental figure III).
Myocardial infarction
Five studies demonstrated the comparison of myocardial infarction between early complete revascularisation versus culprit lesion-only PCI, and there was significant difference in the risk of myocardial infarction (RR 0.37 (95% CI 0.26 to 0.54) p=0.00001).
Revascularisation
Five studies demonstrated the comparison of revascularisation between early complete revascularisation versus culprit lesion-only PCI, and there was significant reduction in the risk of unplanned revascularisation (RR 0.45 (95% CI 0.31 to 0.66) p<0.0001).
Cardiovascular death
Two studies demonstrated the comparison of cardiovascular death between early complete revascularisation versus culprit lesion-only PCI, and there was reduction in the risk of cardiovascular death but not statistically significant (RR 0.47 (95% CI 0.22 to 1.04) p<0.06).
The overall effect of combining all endpoints comparing early complete revascularisation versus culprit lesion-only PCI was statistically significant (RR 0.45 (95% CI 0.37 to 0.55) p<0.00001).
Efficacy of delayed complete revascularisation versus culprit-only PCI
All-cause mortality
Three studies demonstrated the comparison of all-cause mortality between delayed complete revascularisation versus culprit lesion-only PCI, and there was no significant effect of delayed complete revascularisation on all-cause mortality (RR 0.70 (95% CI 0.44 to 1.13) p=0.15) (online supplemental figure IV).
Myocardial infarction
Three studies demonstrated the comparison of myocardial infarction between delayed complete revascularisation and culprit lesion-only PCI, and there was no difference in the risk of myocardial infarction (RR 0.88 (95% CI 0.52 to 1.47) p=0.62).
Revascularisation
Three studies demonstrated the comparison of revascularisation between delayed complete revascularisation and culprit lesion-only PCI, and there was no difference in the risk of unplanned revascularisation (RR 0.96 (95% CI 0.28 to 3.29) p=0.95).
Cardiovascular death
Three studies demonstrated the comparison of cardiovascular death between delayed complete revascularisation and culprit lesion-only PCI, and there was no difference in the risk of cardiovascular death (RR 0.59 (95% CI 0.30 to 1.15) p=0.12).
The overall effect of combining all endpoints comparing delayed complete revascularisation with culprit lesion-only PCI was statistically non-significant (RR 0.78 (95% CI 0.54 to 1.14) p<0.19).
Discussion
The present meta-analysis of randomised and observational studies included 7496 patients comparing the effect of early with delayed complete revascularisation in patients with STEMI. We have demonstrated a benefit in terms of reduction in rate of MACE with complete revascularisation over culprit-only revascularisation, whether the non-culprit revascularisation was performed early or late. We have not demonstrated any relationship between timing of revascularisation in those completely revascularised and differences in clinical outcomes.
It is now well established that MACE is reduced by complete revascularisation when compared with culprit-only revascularisation in patients presenting with STEMI.8 There has been no randomised comparison to guide timing of non-culprit revascularisation. This could be performed at the time of the index PPCI procedure, staged prior to discharge from hospital (both of which would be considered ‘early’ in our analysis) or as a staged elective procedure (delayed). Staged, inpatient revascularisation might increase length of stay after presentation with STEMI, such that an early elective procedure might reduce costs. In analysing those studies where complete revascularisation was performed early separately from those in which it was delayed, we have demonstrated a reduction in MACE from both approaches relative to culprit-only PCI. To investigate this further, we performed a meta-regression analysis and demonstrated no relationship between timing of complete revascularisation and altered relative risk of MACE compared with a culprit-only strategy.
In the most recent published trial, COMPLETE,7 the largest trial in the field to date, 64% of patients randomised to complete revascularisation had it performed before discharge (median 1 day) and 36% after discharge (median 23 days). A subgroup analysis from this study revealed no difference in outcomes whether total revascularisation was performed early or staged, which was consistent with our findings demonstrated in this meta-analysis.
We have demonstrated a statistically significant benefit for early complete revascularisation with PCI compared with culprit-only PCI in terms of a reduction in myocardial infarction, unplanned revascularisation and cardiovascular death. In the studies in which delayed complete revascularisation was performed, we did not demonstrate a significant reduction in myocardial infarction, cardiovascular death and unplanned revascularisation, Studies, such as DANAMI-3-PRIMULTI9 and COMPARE-ACUTE,10 show that early complete revascularisation of non-culprit vessels was associated with good prognosis when compared with infarct-only PCI.
It is possible that early complete revascularisation might have a greater benefit on the outcomes than a delayed approach. If stunned myocardium in the territory of infarction has not fully recovered, ischaemia or infarction related to a non-culprit stenosis might be more likely to lead to cardiovascular death. Delaying non-culprit revascularisation leaves an interval during which a patient might re-present, prompting unplanned revascularisation, particularly as physicians are likely to be unblinded to the findings of the index angiogram.
Limitations
The main limitation to this review is that there are no studies directly comparing early versus delayed revascularisation of non-culprit lesions in the setting of STEMI. Despite the large number of patients included in our analysis, the comparisons of early versus delayed complete revascularisation in this setting are indirect using the same comparator, which is culprit lesion-only PCI, and as such are subject to confounding. Any differences in outcomes between the two groups can only be considered hypothesis generating. An adequately powered randomised trial directly comparing both strategies would be required to address this question more definitively.
Conclusion
In patients presenting with STEMI and multivessel disease treated by PPCI, there is a benefit of complete revascularisation over culprit-only PCI, whether the non-culprit revascularisation is performed in hospital or staged as an elective procedure. We have not demonstrated a relationship between timing of complete revascularisation and MACE.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplemental information.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors KA and MI were responsible for the conception, design, analysis and interpretation of data, drafting of the manuscript and revising it critically for important intellectual content as well as the final approval of the manuscript submitted. Both HT and AA significantly contributed to the conception, design, analysis and interpretation of data, and drafting of the manuscript. AL was significantly involved in the drafting of the manuscript and revising it critically for important intellectual content as well as the final approval of the manuscript submitted.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.