Article Text

Abstract
Objectives To describe the occurrence of significant pericardial effusion, and to investigate characteristics associated with pericardial effusion within three months following heart valve surgery.
Methods A retrospective, observational cohort study including adult patients undergoing heart valve surgery at Odense University Hospital from August 2013 to November 2017. Data were gathered from The Western Denmark Heart Registry and electronic patient records.
Cox proportional hazard models were used to investigate the associations between characteristics associated with significant pericardial effusion during index admission and within 3 months. Results are presented as HR with 95% CI.
Results In total, 1460 patients were included (70% men, median age 71 years (IQR 63–76)) and of those, n=230 patients (16%) developed significant pericardial effusion.
EuroScore II was significantly associated with an increased risk of pericardial effusion during index admission and associated with a lower risk following discharge (index admission HR 1.05, 95% CI 1.02 to 1.08, after discharge HR 0.80, 95% CI 0.69 to 0.92). Increasing age (HR 0.97, 95% CI 0.95 to 0.98 per year) and concomitant coronary artery bypass grafting versus isolated valve surgery (HR 0.58, 95% CI 0.35 to 0.97) were significantly associated with a reduced risk of pericardial effusions in both periods. Being a man (HR 2.30, 95% CI 1.32 to 4.01) and aortic valve disease versus mitral valve disease (HR 2.16, 95% CI 1.20 to 3.90) were significantly associated with an increased risk after discharge.
Conclusion Significant pericardial effusions requiring drainage were present in 16% of cases following heart valve surgery, and different clinical characteristics were associated with the development of effusion.
- pericardial effusion
- heart valve diseases
- cardiac surgical procedures
Data availability statement
No data are available. No data are available due to Danish Law.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Pericardial effusion is a well-known complication following cardiac surgery which may cause prolonged hospitalisations, rehospitalisations, and in the most severe cases, life-threatening cardiac tamponade.
What does this study add?
The study demonstrates how different factors detect patients at risk of pericardial effusion, including young male patients with aortic valve surgery.
How might this impact on clinical practice?
Identifying patients at risk of developing pericardial effusion may help improve postoperative management following heart valve surgery.
Introduction
Pericardial effusion is a well-known complication following cardiac surgery which may cause prolonged hospitalisations, rehospitalisations, and in the most severe cases, life-threatening cardiac tamponade.1–3 Commonly, pericardial effusion develops within the first postoperative weeks and is usually diagnosed with echocardiography.3 4 Incidences of pericardial effusions in available literature vary greatly from 1% to 64%, depending on definitions, study design, observation time and surgical population studied.1 4–9 Opposed to other common complications following cardiac surgery such as atrial fibrillation, heart failure and infections, causes and characteristics of pericardial effusions have not been as thoroughly investigated.4
Most patients, with small pericardial effusion, remain asymptomatic and effusion requires no specific intervention.4 When associated with symptoms or haemodynamic compromise, the effusion requires drainage either ultrasound-guided percutaneous or surgical depending on location or time from surgery.3 There are no proven effective medical treatments of pericardial effusions without inflammation, but, when the pericardial effusion is associated with pericarditis, management should follow that of pericarditis.3 Currently, there is a growing body of evidence of a beneficial effect of Colchicine in preventing recurrent pericardial effusion in pericarditis and postpericardiotomy syndrome,10–14 whereas Colchicine is not recommended in the absence of inflammation.3 Similarly, non-steroidal anti-inflammatory drugs are not indicated as a treatment and may be associated with an increased risk of side effects.3 Thus, there is presently no medical treatment of pericardial effusions following surgery.13
In general, there is a scarcity of studies investigating factors associated with the development of pericardial effusion following heart valve surgery. A recent study of patients undergoing cardiac surgery has demonstrated how younger patients with lower surgical risk score (EuroScore), better cardiac function (measured by left ventricular ejection fraction,LVEF), less coronary artery disease and higher preoperative haemoglobin values undergoing heart valve surgery are at higher risk of developing late (>7 days) pericardial effusion.4 In addition, preoperative or postoperative anticoagulation, surgery other than coronary artery bypass grafting (CABG), implantation of a mechanical valve prosthesis, and blood transfusions have been demonstrated to be associated with increased risk of cardiac tamponade.2 9 Nevertheless, to prevent patients from developing significant pericardial effusions and to be aware of patients at increased risk, more knowledge about factors associated with pericardial effusions is needed.
Thus, the objectives of this study were to describe the occurrence of significant pericardial effusion defined as effusion requiring intervention and to investigate characteristics associated with pericardial effusion within 3 months following heart valve surgery.
Materials and methods
Study design
The study was designed as a retrospective observational cohort study.
Participants and setting and recruitment
All consecutive patients undergoing open heart valve surgery (replacement or repair) at a tertiary Danish teaching facility, Odense University Hospital, Denmark, from August 2013 to November 2017 were included in the cohort study. Adult patients (≥18 years) with aortic valve diseases, mitral valve diseases or tricuspid valve diseases were included based on their surgical procedure codes, Nordic/NOMESCO Classification of Surgical Procedures,15 online supplemental table S1. Patients were grouped according to their primary valve disorder. Only patients with permanent residence in the Region of Southern Denmark were included.
Supplemental material
Data collection
Demographic and clinical data
Demographic and clinical data from the index admission were obtained from electronic medical records and the Western Denmark Heart Registry (WDHR).16 Data on sex, age, smoking status (current or former smoker), alcohol consumption (above the national limit of ≥7 unit/week/women and ≥14 units/week/men), body mass index, length of hospital stay and medical treatment were obtained from the electronic medical record. From the WDHR, information on the type of surgery, comorbidity, EuroScore II and blood transfusions were obtained.
Data on relevant medical treatment, including anticoagulants, platelet aggregation inhibitors, direct oral anticoagulants and use of ibuprofen, were obtained from the medical records. Medications (prescription based) received during the 3 months follow-up were registered. Among patients developing pericardial effusion requiring drainage, medications prescribed before the drainage were registered and included, to ensure that only medication intake prior to drainage was included in the analyses.
Outcomes
The primary study outcome was significant pericardial effusion defined as a pericardial effusion requiring drainage/pericardiocentesis (either percutaneous ultrasound-guided or surgical). Method/technique of drainage was decided by the treating cardiac surgeon and cardiologist, and if possible, percutaneous drainage was preferred. All significant pericardial effusions during both index admission and within the first 3 months after surgery were included. Data on significant pericardial effusions, including the type of drainage, date of drainage and whether it was performed before or after discharge were obtained from the patient electronic medical records. All pericardial effusions were registered, but only the first drainage was included in the overall analyses. Although patients could be transferred to or readmitted at local hospitals, the pericardial drainage was only performed at the tertiary centre, Odense University Hospital.
Statistics
Baseline characteristics were presented as number and percentage for categorical data and median and 25th to 75th percentiles (IQR) for continuous data since the normality assumption was not met (tested with the Shapiro-Wilks test and visualised with QQ plot). To compare baseline characteristics, the χ2-test was used for categorical variables, and the Mann-Whitney U test was used to compare continuous data.
The proportion of patients with significant pericardial effusion, type of procedure and median time (days) from surgery to the procedure was calculated.
To investigate characteristics associated with significant pericardial effusion, first, univariable Cox proportional hazard models were performed in two different models. Model 1 investigated characteristics associated with the risk of developing significant pericardial effusion during the index admission and model 2 investigated characteristics associated with significant pericardial effusion drainage after discharge and up to 3 months post surgery. The underlying time scale was time to the first event measured in days. Second, multivariable Cox proportional hazard models were performed with outcomes similar to the above models. Variables included in the models included covariates with a p value <0.20 in the unadjusted analyses and characteristics assumed to be related to the significant pericardial effusion (age, EuroScore II, cardiac function, coronary artery disease and anticoagulants2 4 9). The underlying time scale in model 2 was time from discharge to the first event thereafter, measured in days. Analyses of potential interactions among variables were performed. In cases with collinearity, the variable that had the best performance in the model (tested with the likelihood ratio) was included, and in general, variables with only a few events were excluded. The proportional hazard was assessed graphically using hazard plots, and the assumptions were met. Results were presented as HRs with its 95% CIs.
A p value of <0.05 was considered to be statistically significant. STATA IC V.16 (StataCorp) was used for the analyses.
Results
During the study period, 1460 patients underwent heart valve surgery and were included in the current study. Of those, 70% were men, the median age was 71 years (IQR 63–76), 62% were diagnosed with aortic valve stenosis, and median length of stay was 9 days (IQR 7–13). Demographic and clinical characteristics among the total population are summarised in table 1. In total, 66 patients (4.5%) died during the first 3 months after surgery, the majority, 55 patients, during the index admission. In the period after surgery, 79% of the patients were treated with acetylsalicylic acid and 41% with warfarin (table 2).
Baseline characteristics
Relevant medical treatment following surgery and within the first 3 months among patients with significant pericardial effusions and without
Occurrence of significant pericardial effusion
During the follow-up period of 3 months, n=230 patients (16%) developed a significant pericardial effusion, 52% were drained as a subxiphoid (surgical) approach versus 48% as a parasternal/ultrasound-guided approach. In 125 patients (54%), the drainage was performed before discharge during the index admission, and in 105 patients (46%) after discharge (figure 1 and online supplemental table S2). The median time to treatment of significant pericardial effusion was 10 days (IQR 6–17) for the entire population. Among patients who died, eight developed significant pericardial effusions before their death (all before discharge).

Number of patients with significant pericardial effusions within 90 days after surgery.
Patients developing significant pericardial effusion were more often men (76% vs 69%, p=0.035), were more often in the younger age group from 18 to 65 years (50% vs 27%, p≤0.001), had a lower median EuroScore II (1.8 vs 2.2, p≤0.001) and fewer had coronary artery disease and were thus less likely to undergo concomitant CABG (13% vs 30%, p≤0.001) (table 1). Of the patients who developed significant pericardial effusion, 15 patients (7%) had drainage performed more than once. Colchicine was prescribed for n=5 patients (0.3%) before the pericardiocentesis and for n=32 patients (2%) after pericardiocentesis.
Factors associated with significant pericardial effusion
Factors associated with significant pericardial effusion during index admission (univariable model 1) and after discharge (univariable model 2) are presented in table 3. In the univariable models, EuroScore II was significantly associated with the risk of developing significant pericardial effusion during index admission and was associated with a reduced risk following discharge (EuroScore II, index admission HR 1.05, 95% CI 1.01 to 1.08, after discharge HR 0.63, 95% CI 0.52 to 0.75) (table 3).
Unadjusted characteristics associated with significant pericardial effusions within 90 days after surgery
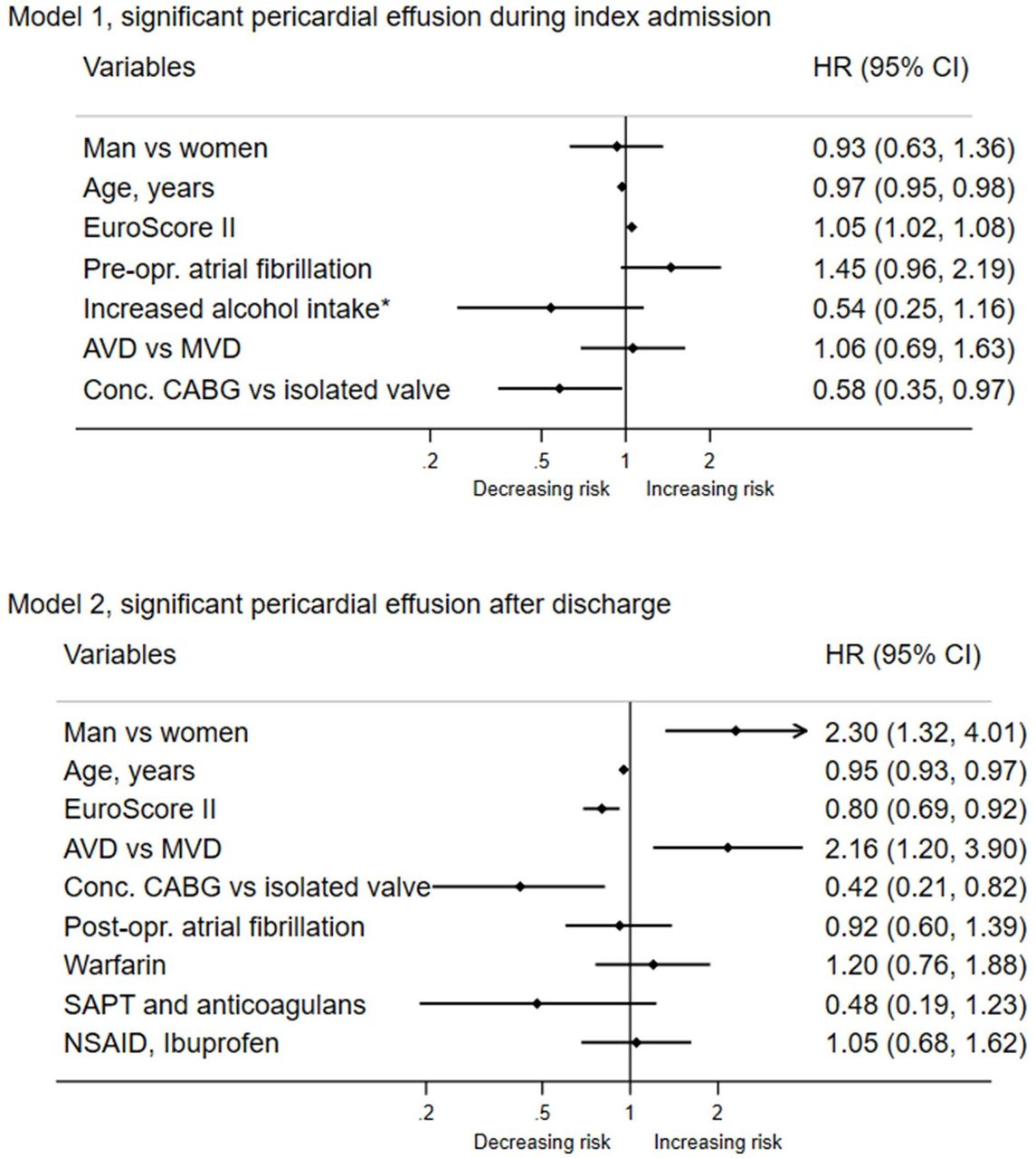
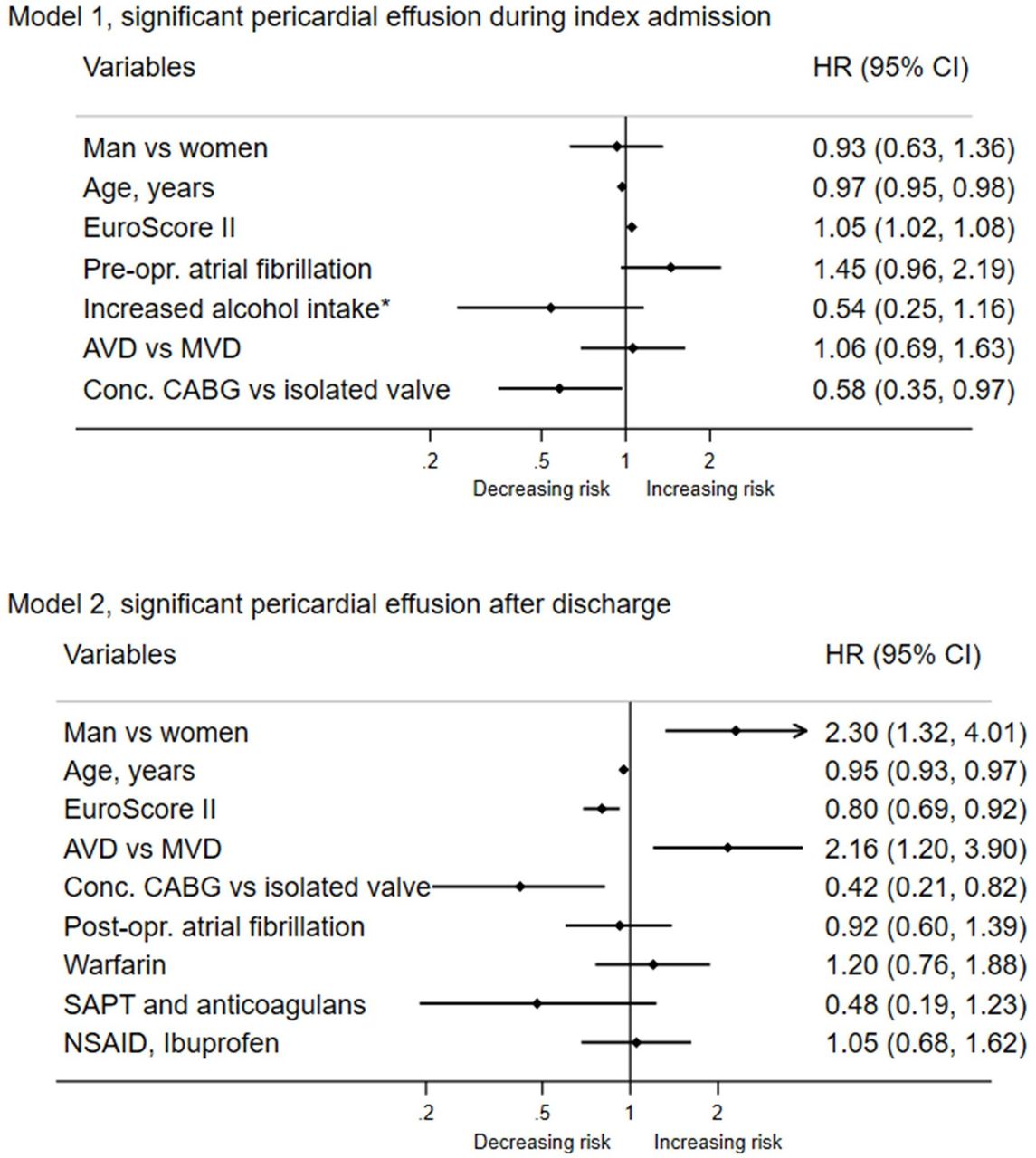
In the adjusted analyses, EuroScore II (HR 1.05, 95% CI 1.02 to 1.08) was significantly associated with increased risk of significant pericardial effusion and increasing age (HR 0.97, 95% CI 0.95 to 0.98 per year) and concomitant CABG versus isolated valve surgery (HR 0.58, 95% CI 0.35 to 0.97) were associated with a reduced risk of significant pericardial effusion during index admission (model 1) (figure 2). After discharge, being a man (HR 2.30, 95% CI 1.32 to 4.01) and aortic valve disease versus mitral valve disease (HR 2.16, 95% CI 1.20 to 3.90) were associated with an increased risk of significant pericardial effusion. Conversely, increasing age (HR 0.95, 95% CI 0.93 to 0.97), EuroScore II (HR 0.80, 95% CI 0.69 to 0.92) and concomitant CABG versus isolated valve surgery (HR 0.42, 95% CI 0.21 to 0.82) were significantly associated with a reduced risk of significant pericardial effusion after discharge (model 2) (figure 2). When testing for interactions, the interaction between being a man and mechanical valve replacement were significantly associated with outcome (p value for interaction 0.028), no other significant interaction terms were found.
{kind=link}
{kind=link}
Characteristics associated with significant pericardial effusions at different time points. The figures illustrate characteristics associated with significant pericardial effusions during the index admission (model 1) and after discharge (model 2). The models included covariates with a p value <0.25 in the unadjusted analyses and/or characteristics assumed to be related to the significant pericardial effusion. AVD, aortic valve disease; CABG, coronary artery bypass grafting; Conc., concomitant; NSAID, non-steroidal anti-inflammatory drug; MVD, mitral valve disease; SAPT, single antiplatelet therapy.
Discussion
In this retrospective cohort study, we investigated characteristics associated with significant pericardial effusion within the first 3 months following heart valve surgery. We found that 16% of patients developed pericardial effusion requiring drainage at any time during the first 3 months after surgery. Although the majority of effusions were managed during the first 2 weeks after surgery, some patients were treated more than 2 months after surgery. Several clinical and demographic characteristics were associated with significant pericardial effusion, although characteristics varied during index admission and after discharge. This knowledge might help clinicians assess and be aware of patients with a higher risk profile.
The incidence of significant pericardial effusion (16%) found in the current study is seemingly high when compared with previous studies.1 4–9 This can be explained by several factors: several studies report incidences of significant pericardial effusions based on broad cardiac surgical populations, including patients undergoing isolated CABG. Previous studies have suggested CABG to be associated with a lower risk of postoperative pericardial effusion compared with valve procedures.2 4 8 17 Thus, a direct comparison between these studies and the present study should be done with caution. The haemostasis techniques in CABG in combination with a wide opening to the left pleura may facilitate drainage of pericardial fluid and prevent pericardial effusions.8 Thus, it is expected that our study, only including patients undergoing valve surgery, will find a higher proportion of pericardial effusions. In addition, the definition of significant pericardial effusion versus cardiac tamponade varies across studies1 4–9 18 and in the current study, all significant pericardial effusions requiring drainage were included.
As significant pericardial effusions prolong hospitalisations, increase the risk of developing tamponade and are a significant burden for the patients,1–3 gaining knowledge on how to identify patients at higher risk is important. This identification, for example, of higher risk among men with mechanical valve replacements, can increase awareness about the risk and support early echocardiography postoperatively and thus, manage pericardial effusions when developed. In the current study, a significant finding was the association between younger age and the risk of developing significant pericardial effusions in both periods. Khan and colleagues have previously demonstrated a similar finding.4 As younger patients most commonly present ‘better’; have lower surgical risk (measured with EuroScore), fewer comorbidities and are less likely to suffer from ischaemic heart disease, many of the other significant variables in the current analyses might be explained by age. Whether the inflammatory response of the valve surgery is different in younger patients than more elderly has previously been speculated but never demonstrated.4 19 Thus, whether the development of pericardial effusions following heart valve surgery is caused by the mechanical process of the surgery and/or an inflammatory process in the pericardium, is currently unknown.20 Furthermore, as the pathogenesis of the pericardial fluid differs depending on the underlying pericardial disease, this might also be related to the development of pericardial effusions following surgery.20 In general, findings of the current study suggest, that early development of significant pericardial effusions might be related to higher surgical risk, whereas the development longer after surgery (after discharge) might be related to other factors such as inflammatory response. Also, ibuprofen intake was not associated with pericardial effusion in the adjusted models which might be related to it being used as a treatment of postoperative pain, pro necessitate. Thus, whether ibuprofen influence the inflammatory response after discharge cannot be demonstrated in the current study. Future studies should incorporate markers of inflammation to better elucidate the importance of inflammation in the development of pericardial effusion.
The increased risk of pericardial effusions related to isolated valve surgery is in line with earlier studies and is commonly explained by the use of anticoagulant therapy.4 21 In the univariable analyses, we demonstrated how the use of many anticoagulants appeared to be associated with reduced risk of developing significant pericardial effusions, except for treatment with warfarin. In the adjusted analyses, these associations did not remain and as such, does not suggest that anticoagulation per se is associated with the development of significant pericardial effusion in the present study.
Strengths and limitations
Our study has the strength of being performed on a complete set of data from electronic patient records and the WDHR.16 Also, development of significant pericardial effusion was recorded from a thorough review of patient records and validated by two persons, and as this procedure is only performed in a single centre in the Region of Southern Denmark making it unlikely that procedures were missed. Moreover, the study included a consecutive cohort of all patients undergoing open heart valve surgery during the period. To ensure only medical treatment related to the outcome were included in the analyses, all medical treatment prescribed after the outcome had occurred was left out of the regression models.
The study also has limitations. The study was conducted as a single-centre study, where the outcome and results may reflect local patient selection and treatment protocols. This might restrict the generalizability of the results, and we acknowledge how a multicentre cohort study would have been a strength. Besides, the retrospective design has limitations. The retrospective design precludes any assumption of causality of identified associations. Yet, as data were based on prospectively captured register-data and real-life data from electronic patient records, we do not believe this influences the demonstrated associations.
The timing of the removal of pericardial drains might increase the risk of developing significant pericardial effusions, as described in earlier studies.4 17 22 23 In current study removal drains were standardised and performed at the intensive care unit, but whether differences in reporting influence the current result is unknown. Finally, we acknowledge how the study is a descriptive, hypothesis-generating study and more knowledge on factors associated with outcomes based on prospective designs are needed before drawing a causal conclusion.
Conclusion
In a consecutive cohort of patients undergoing heart valve surgery, significant pericardial effusions requiring invasive drainage were present in 16% of cases. Although the majority of effusions were managed during the first 2 weeks after surgery, some patients were treated more than 2 months after surgery. EuroScore II increased the risk of significant pericardial effusion during index admission and reduced the risk following discharge. Increasing age and concomitant CABG versus isolated valve surgery reduced the risk of significant pericardial effusions in both periods, whereas being a man and aortic valve disease versus mitral valve disease increased the risk after discharge.
The study highlights the need for further research investigating the potential inflammatory processes of pericardial effusions following open heart valve surgery.
Data availability statement
No data are available. No data are available due to Danish Law.
Ethics statements
Patient consent for publication
Ethics approval
The investigation conformed with the principles outlined in the Declaration of Helsinki. The study was approved by the Danish Data Protection Agency (18/19152) and Danish Patient Safety Authority.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors BB, JSD and JEM were involved in designing the study. BB, JSD, MGW, EKL, SNN and JEM participated in data collection, and BB, JSD and JEM were involved in analysing and interpretation of data in collaboration with OE. BB wrote the first draft of the manuscript. BBO is overall guarantor for the content. All authors critically revised the manuscript. All authors approved the final version of the manuscript.
Funding Helsefonden, The Odense University Hospital PhD foundation, Ove William Buhl Olesen and Edith Buhl Olesen Foundation and Kurt Bønnelycke and Grethe Bønnelycke Foundation funded this research.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.