Article Text

Abstract
Objective To explore the importance of early life factors shared by siblings, such as parental socioeconomic position, parental practices, housing and neighbourhood, for the association between cardiovascular disease (CVD) risk factors and mortality from CVD, ischaemic heart disease (IHD) and cerebrovascular disease.
Methods Norwegian health surveys (1974–2003) were linked with data from the Norwegian Family Based Life Course Study and the Cause of Death Registry. Participants with at least one full sibling among survey participants (n=2 71 643) were included. Data on CVD risk factors, body mass index (BMI), height, systolic blood pressure (SBP) and total cholesterol (TC) were stratified into ‘low’, ‘medium’ and ‘high’ risk, and smoking to ‘daily smoking’ and ‘not daily smoking’.
Results Mean age of participants was 41 years, mean follow-up time was 19 years and during follow-up 2512 died from CVD. For each category of increased risk factor level, the per step HR of CVD mortality was increased by 1.91 (95% CI 1.78 to 2.05) for SBP, 1.67 (1.58 to 1.76) for TC, 1.44 (1.36 to 1.53) for BMI, 1.26 (1.18 to 1.35) for height and 2.89 (2.66 to 3.14) for smoking. In analyses where each sibship (groups of full siblings) had a group-specific baseline hazard, these associations were attenuated to 1.74, 1.51, 1.29, 1.18 and 2.63, respectively. The associations between risk factors and IHD mortality followed the same pattern.
Conclusion Early life family factors explained a small part of the association between risk factors and mortality from CVD and IHD in a relatively young sample.
- risk factors
- epidemiology
- public health
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Early life circumstances have been shown to be important for later cardiovascular risk and mortality, and to partly explain socioeconomic differences in cardiovascular disease (CVD).
What does this study add?
This study explores the influence of early life family factors on the association between cardiovascular risk factors and cardiovascular mortality. This indicates to which degree cardiovascular risk factors are established in early life or modifiable in adulthood.
How might this impact on clinical practice?
The association between cardiovascular risk factors and cardiovascular mortality was not extensively influenced by early life family factors. Thus, targeting conventional risk factors in adulthood should continue to play a major role in the prevention of CVD, even though early life interventions also are of importance. The actual risk estimates used to target high-risk individuals in adulthood can continue to be used in practice.
Introduction
Conventional risk factors for cardiovascular disease (CVD), such as smoking, hypertension, high cholesterol levels and physical inactivity, have been associated with later risk of CVD1 and shown to explain most of the CVD cases in many populations.2 Knowledge on these risk factors forms the basis for primary and secondary prevention in population-wide efforts and clinical settings.1 Early life factors3 4 have been proposed as important contributors to adult CVD risk and mortality, as well as to CVD risk factors.5 6 Factors in early life could be shared by siblings, such as parental socioeconomic position (SEP), parental practices, housing and neighbourhood and include a 50% shared germ line for full siblings. Non-shared factors include systematic elements such as birth year and birth order, and non-systematic chance events such as sibling–sibling interactions, differential parental treatment and peer groups.
The socioeconomic gradient in CVD has been partly explained by early life factors in some,7 8 but not all9 10 studies. In one study, the association between education and body mass index (BMI) was attenuated when adjusting for early life family factors.11 A recent Norwegian study reported a confounding effect of early life factors on the association between CVD risk factors and education.12 Early life family factors have, however, not been shown to explain the association between CVD,13 14 or its risk factors like hypertension,13 15 and low birth weight.
To what extent the association between levels of CVD risk factors and CVD mortality is confounded by early life family factor remains to be explored. This has practical implications, as it indicates to which degree risk factors for CVD are established in early life or modifiable in adulthood. Large data sets, such as register data and data from large health surveys, give the opportunity to explore the importance of factors shared by siblings, by comparing results from analyses of associations between all individuals in a cohort to results from sibship analyses, which omit factors that are constant within sibships (groups of siblings) in the same sample. Thus, the aim of this study was to explore the importance of early life factors shared by full siblings (sharing mother and father) for the association between each of the cardiovascular risk factors systolic blood pressure (SBP), total cholesterol (TC), BMI, height and smoking, and later mortality from ischaemic heart disease (IHD), cerebrovascular disease and all CVD combined. The study was carried out in a sample of relatively young adult women and men, using data from the Norwegian Family Based Life Course (NFLC) study.16
Methods
Study population
Data from national and regional health surveys in Norway were linked with data from the Norwegian Population Registry, data from the NFLC study16 and the Cause of Death Registry, using personal identification numbers. In the Counties Study (1974–88), all men and women aged 35–49 years living in three different counties in Norway were invited to cardiovascular screening.17 In the Age 40 Program, inhabitants aged 40–44 years from all counties in Norway, except from Oslo, were invited (1985–1999).18 The Cohort of Norway (CONOR) (1994–2003) is based on data from regional health surveys, with participants aged 20–103 years.19 The attendance rate of the three surveys were 86%, 70% and 58%, respectively.17–19
For the current study, all participants from the Counties Study, the Age 40 Program and CONOR born in 1940 or after were selected. If they attended more than one health survey, data from the first survey attended were used. The study population consisted of participants with at least one full sibling (sharing both mother and father) among the health survey participants. The index person's mother and father were identified by linkage in the NFLC study.16 Parental identification has proven to be reliable for persons born in 1940 and after.16 The study population consisted of 271 643 participants (figure 1).

Flow chart.
Cardiovascular risk factors
In all health survey screenings self-reported smoking status (‘daily smoker’/‘not daily smoker’) and current treatment of hypertension were recorded. Blood pressure (BP) was initially measured manually by sphygmomanometers and later by automatic oscillometric measures.20 Height and weight were measured and BMI (kilogram/square metre) was calculated. Non-fasting TC was initially measured by non-enzymatic, and later enzymatic, method. Non-enzymatic values were converted by a correction factor.21 Acceptable stability of BP measures and laboratory analyses over time in the population surveys have been reported.20 21
Cardiovascular mortality
Data on underlying causes of death from IHD (International Classification of Diseases, 9th Revision (ICD-9): 410–414, International Classification of Diseases, 10th Revision (ICD-10): I20–I25), cerebrovascular disease (ICD-9: 430–438, ICD-10: I60–I69) and all CVD combined (ICD-9: 390–459, ICD-10: I00–I99) were obtained from the Norwegian Cause of Death Registry. Participants were followed from time of survey to death or end of follow-up (31 December 2012), with a mean follow-up time of 19 years.
Statistical analyses
SBP and TC were categorised according to the Framingham model,22 with ‘low’, ‘medium’ and ‘high’ risk (SBP ‘<130’, ‘130–159’ and ‘≥160’ mm Hg; TC ‘<5.2’, ‘5.2–6.1’ and ‘≥6.2’ mmol/L). BMI was categorised according to established cut-offs, ‘normal weight <25’, ‘overweight 25–29.9’ and ‘obesity ≥30’ kg/m2. Very few participants (1.0%, n=2836) were underweight (BMI <18.5 kg/m2), so those participants were included in the normal weight category. Height was categorised into tertiles ‘<167’, ‘167–175.9’ and ≥176’ cm.
Cox proportional hazards regression model, with age as underlying time, was used to estimate HRs of mortality from CVD, IHD and cerebrovascular disease according to categories of risk factors (SBP, TC, BMI, height and smoking). Time (years of age) at risk was counted from a participant's entry in the study. Individuals who did not die during follow-up were censored at their age at the end of follow-up. In the cohort analyses, where all participants were analysed with no regard to sibships, we used Huber-White sandwich estimator to correct standard errors, which otherwise may be underestimated due to familiar clustering. The cohort analyses should produce results similar to those found in studies of unrelated individuals. For the within sibship analyses, where each sibship had a group-specific baseline hazard, we used the stratified Cox regression model of Holt and Prentice.23 The proportional hazards assumption was examined by first plotting the scaled Schoenfeld residual against age, supplemented by a global test of a zero slope in the association between age and the scaled Schoenfeld residuals. The analyses were run adjusted for sex and birth year. In regressions were SBP was the exposure, analyses were additionally adjusted for being under current treatment for hypertension. We compare the cohort and sibship analyses to assess the importance of shared environment. In sibship analyses, only those with a sibling in a discordant risk factor category contributes. To check the impact of this, we run cohort analyses including only those with a sibling discordant in risk factor category. Sensitivity analyses were also run adjusting for size of sibling group and index health survey.
Spline curves showing the predicted HR for cardiovascular mortality at different levels of SBP, TC and BMI were estimated from Cox proportional regression models, entering risk factors as restricted cubic splines. The intraclass correlations for continous variables, describing how strongly individuals within sibling groups resemble each other, were estimated using a random effect model, adjusted for age.
The population attributable fraction (PAF) was estimated in both cohort analyses and sibship analyses for the association between the risk factors SBP, TC, BMI, height and smoking and mortality from IHD, cerebrovascular disease and CVD, using Cox regression. Reference value was lowest risk category.
Data was analysed using Stata V.14.
The study was approved by the Norwegian Regional Committees for Medical and Health Research Ethics (REK) (2012/827).
Results
The mean age of the participants was 41 years (table 1), and 84% of the sample was between 40 and 45 years. Only 4% were below the age of 40. At the end of the follow-up, 2512 had died from CVD, including 1662 from IHD and 552 from cerebrovascular disease. Mean age at the time of censoring was 60 years. Of participants, 60% had one sibling in the sample, 26% had two, 9% had three and 4% had four or more siblings. The proportions of participants having a sibling in a discordant risk factor level were about or above 50% for all risk factors (table 2). The intraclass correlations for the cardiovascular risk factors were strongest for TC and lowest for SBP (table 3).
Characteristics of the sample, 271 643 participants from Norwegian health surveys
Proportions of individuals in a different category of cardiovascular disease risk factors than one or more sibling. Participants from Norwegian health surveys
Intraclass correlation (SE) for cardiovascular risk factors among siblings in Norwegian health surveys. From a random effect model with maximum likelihood estimation, adjusted for age
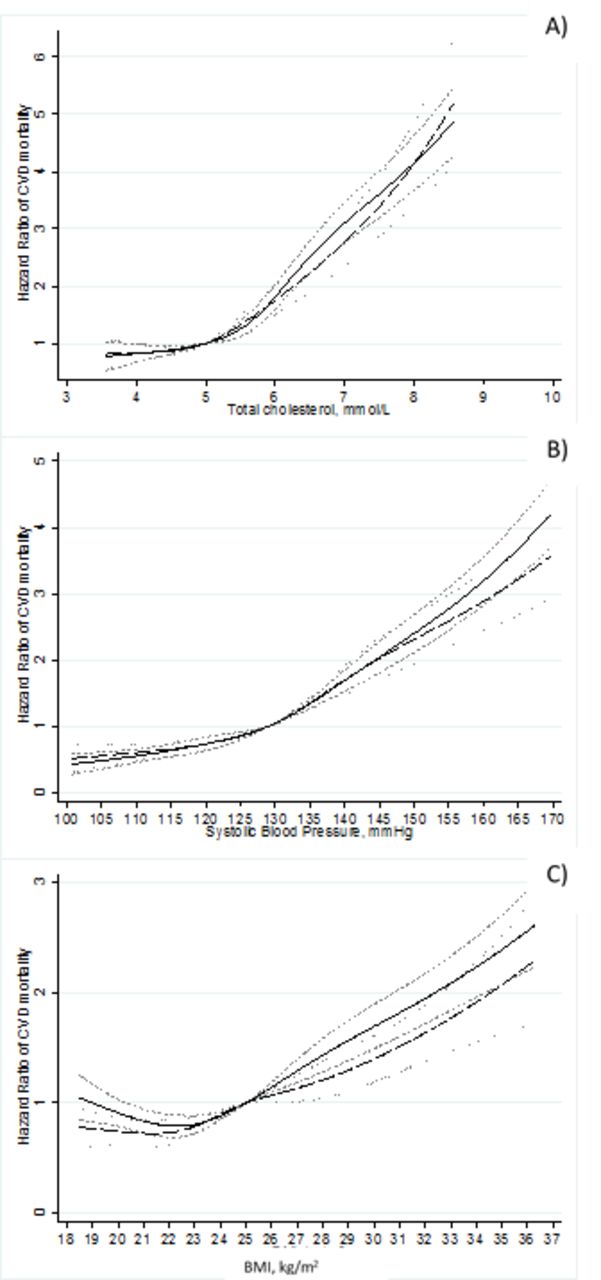
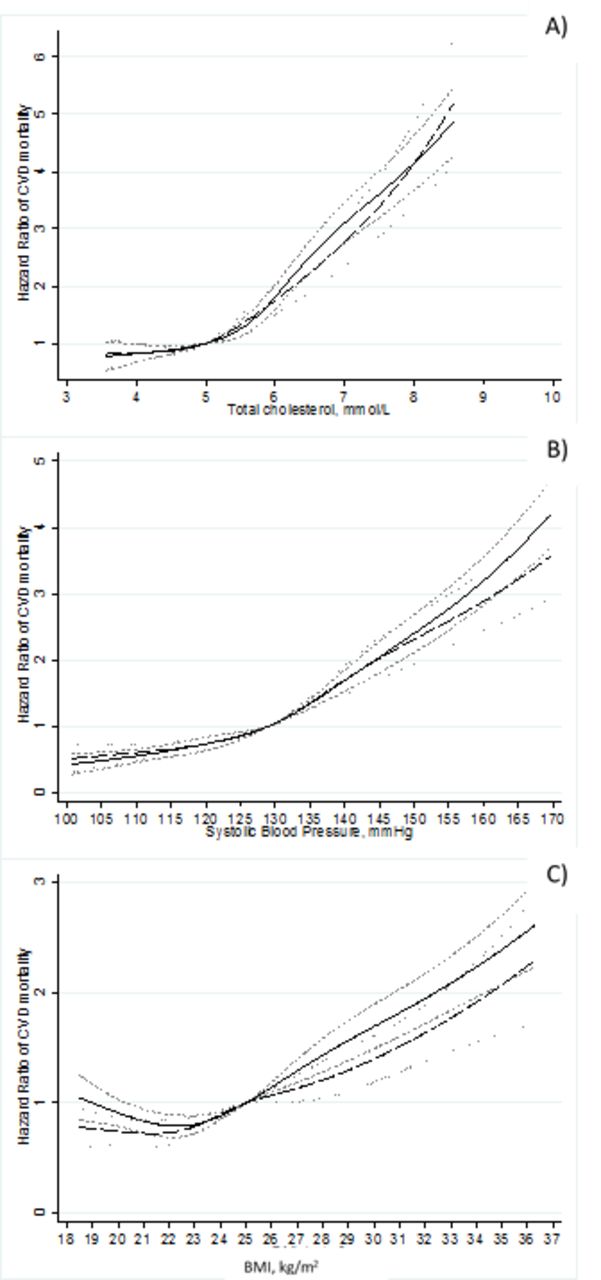
The risk of total CVD mortality, and IHD mortality, increased with higher values of SBP, TC and BMI, with smoking and with lower height (table 4). The HRs in higher risk factor levels were somewhat attenuated in within sibship analyses compared with cohort analyses. The increasing HRs of CVD mortality with increasing values of SBP, TC and BMI are shown in figure 2A–C, respectively, with the risk factors entered as restricted, cubic splines. Spline curves for IHD are shown in online supplementary figure 1.
Supplementary file 1
Cardiovascular risk factors in relation to mortality from CVD, IHD and cerebrovascular disease among adult participants in Norwegian health surveys. Adjusted for birth year and sex
{kind=link}
{kind=link}
Predicted HR for CVD mortality at different levels of (A) TC, (B) SBP and (C) BMI. Reference category SBP: 129 mm Hg, TC: 5 mmol/L and BMI: 25 kg/m2. Estimated from Cox proportional regression models, entering risk factors as restricted cubic splines. Solid line: cohort analyses. Dotted line: sibship analyses. BMI, body mass index; CVD, cardiovascular disease; SBP, systolic blood pressure; TC, total cholesterol.
The risk of cerebrovascular disease mortality increased with higher levels of SBP and TC, with smoking and with lower height (table 4). In within sibling analyses, estimates were slightly attenuated for SBP and smoking, however not for TC and height, for which the estimates were slightly increased.
PAFs of SBP, TC, BMI, height and smoking on mortality from CVD, IHD and cerebrovascular disease are shown in table 5. The PAF estimates show how much of the CVD mortality that could be accounted for by each risk factor. For example, 43% of all CVD deaths were attributable to smoking, and if everyone had been in the lowest risk category for TC, half of all IHD deaths would be avoided. The risk factors contributing the most to CVD and IHD mortality were smoking and TC and to cerebrovascular disease mortality smoking and SBP. PAF estimates in sibship analyses were somewhat lower than in cohort analyses.
Population attributable fraction (%) of smoking, medium or high-risk levels of systolic blood pressure, total cholesterol, being overweight or obese and of being in the two lowest tertiles of height on CVD, IHD and cerebrovascular disease mortality in cohort and within sibship analyses from Cox regressions
Adjusting for index health survey or size of sibling groups in sensitivity analyses did not change the results essentially (results not shown). When including only those with a sibling discordant for risk factor category in cohort analyses on CVD mortality, no substantial changes were seen for SBP, BMI and height (see online supplementary table 1). Regarding TC, per step HR was attenuated towards the HR in sibship analyses, and the per step HR for smoking became lower than in sibship analyses. For IHD mortality, no substantial changes were seen in per step HR for SBP or BMI; however, estimates were attenuated towards sibship estimates for TC and height and below sibship estimates for smoking. Regarding cerebrovascular disease mortality, cohort estimates were increased for SBP, TC, BMI and height, and attenuated for smoking only.
Supplementary file 2
Discussion
The risk of CVD mortality increased as expected with raised levels of SBP, TC and BMI, as well as with smoking and with lower levels of height.2 Within sibship analyses suggested that early life factors to some degree confound the association between CVD risk factors and death from CVD and IHD. However, importantly, most of the association between risk factors and mortality was unrelated to early life factors. The results should be interpreted in light of the fact that the sample was relatively young for CVD.
One previous study in a cohort overlapping ours have reported less variation of CVD risk factors within sibships than between individuals,12 confirming some importance of early life factors on CVD risk factors. An association between childhood SEP and adult BMI has previously been reported by some,24 but not all25 studies. SBP has been weakly associated with childhood SEP,24 25 and smoking has been mostly attributed to adult SEP.26 Childhood SEP is one of the important early life factors siblings share. Thus, a modest intraclass correlation for risk factors within sibships, suggesting fairly large variation, is in line with previous research. We found early life factors to be less important for the association between the CVD risk factors under study and cerebrovascular disease than for the association with IHD and total CVD. Risk factors not included in this study, such as previous heart disease and diabetes, could be more important for cerebrovascular disease.27 If we had such risk factors included, the importance of early life family factors for the association between cerebrovascular disease and risk factors might have been stronger.
Height in adulthood is a composite measure of health and nutrition during growing years and genetic disposition. It is a trait potentially modifiable in the period where most siblings share environment, but will generally not be influenced by adult lifestyle factors. Up to late 1980s, the height of Norwegian conscripts was increasing, but has later been stable.28 The majority of our study population was born before the flattening of the height trend. It is thus plausible that adult height is related to environmental factors during childhood, like access to material resources, including adequate nutrition. Height, therefore, serves as a model exposure for shared early life environment in sibling design, as other CVD risk factors examined are modifiable also in adult life where most siblings does not share environment, and the effects of shared early life environment within sibships might be diluted by differential adult lifestyle. The attenuation of association between height, as well as BMI and CVD mortality was considerable between cohort and within sibling analyses, confirming our hypothesis that early life factors are at play.
Assumptions in sibling design
Only siblings discordant in exposure contribute to the estimation of the impact of early life family factors on the association under study. Using more risk strata would have given more siblings in different categories. We did, however, consider the use of three conventional risk categories practically and clinically relevant. Confounders could be the cause of discordance in risk factors and thus cause estimates for risk factor levels to become stronger in the sibship analyses.29 Families with discordant and concordant risk factor levels among siblings may differ. For example, in families where all siblings have a preferable risk factor profile, this may be due to both health related habits and genetic disposition. Siblings with discordant risk factor levels despite shared childhood circumstances may differ more in non-shared factors than two random persons do. It may also be that they were in different age groups. Including only those with a sibling in a discordant risk factors group in cohort analyses did not change results essentially.
Matching siblings on known mother and father probably gives siblings sharing more of early life environment, as well as of the germ line, than siblings defined as having the same mother only. We do not know, however, whether some parents separated during early life. A divorce might have influenced the extent of early life factors shared by siblings. Up to the 1960s, divorce rate was low and constant at 4 per 1000 marriages in Norway. During the 70s and beginning of the 80s, it rose to about 7 per 1000 marriages.30 We rely on shared early life factors to contribute to the estimation of early life confounding on risk factor differences in CVD mortality. If such factors are not fully captured by being siblings, the confounding effect may be larger than our estimates. Circumstances in a family may change due to factors not shared by siblings, for example, more children means less resources on each. Adjustment for size of sibling group produced little change in results.
Strengths and limitations
This population-based study had a large sample size and the ability to study the impact of early life environment on associations between cardiovascular risk factors and mortality using sibship analysis. Use of register data by large sample size eliminates problems related to loss to follow-up. The response rate of the health surveys from which data originated was reasonable. The majority of the sample was in their 40s at screening, and many subjects did not reach an age during follow-up where CVD mortality is probable. Mean age at censoring was 60 years, and mean age of death was 55 years. Thus, our results confine roughly to premature CVD death. If we had the possibility to follow the participants for a longer period, more deaths would have occurred, and the importance of early life factors for the associations between risk factors and mortality might have changed. To account for possible secular trends in risk factors, CVD deaths and attained levels of education, we adjusted the analyses for birth year. We also adjusted for sex, as stratification on sex would have left fewer sibling comparisons and considerably reduced the power of the analyses. Further, the inclusion of any variable that is associated with the outcome may cause the estimates of other variables to inflate even in the absence of confounding in a Cox regression.31 This might counteract the attenuation of confounding by early life factors.
Implications
Associations between adult risk factor profile and future mortality from CVD and IHD vary to some degree with shared early life family factors. However, the CVD risk factor profile is strongly associated with mortality regardless of early life factors. Targeting conventional risk factors in adulthood should thus continue to play a major role in the prevention of CVD, even though early life interventions also will be of importance for later cardiovascular risk.
References
Footnotes
Contributors ØN conceived the idea for the article. MKRK did the statistical analyses and the drafting of the article. All authors contributed in the final stage of the writing.
Funding The work was supported by the Norwegian Research Council (grant number 213788).
Competing interests None declared.
Patient consent New consent is not required as consent was obtained at the time the data was collected and by those who undertook the study.
Ethics approval Norwegian Regional Committees for Medical and Health Research Ethics (REK) (2012/827).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Data are owned by Norwegian Institute of Public Health (NIPH) and cannot be shared. Application has to be sent to NIPH after approval of study from Norwegian Regional Committees for Medical and Health Research Ethics.