Article Text

Statistics from Altmetric.com
In 1980, a significant segment of the US population was already overweight or obese, but obesity standards did not exist. Therefore, the National Institutes of Health (NIH) held the Workshop on Body Weight, Health and Longevity to correct the deficiency so that data could be improved. The workshop concluded:In the United States, the weight associated with the greatest longevity tends to be below the average weight of the population under consideration, if such weights are not associated with a history of significant medical impairment. Overweight persons tend to die sooner than average-weight persons, especially those who are overweight at younger ages. The effect of being overweight on mortality is delayed and may not be seen in short-term studies. Cigarette smoking is a potential confounder of the relationship between obesity and mortality. Studies on body weight, morbidity, and mortality must be interpreted with careful attention to the definitions of obesity or relative weight used, preexisting morbid conditions, the length of follow-up, and confounders in the analysis. The terminology of body weight standards should be defined more precisely and cited appropriately. An appropriate database relating body weight by sex, age, and possibly frame size to morbidity and mortality should be developed to permit the preparation of reference tables for defining the desirable range of body weight based on morbidity and mortality statistics.1
Based on body mass index (BMI), 1.5 billion people are overweight (BMI≥25.0 kg/m2) and 500 million of them are classified as obese (BMI≥30 kg/m2).2–3 Since 1980 there have been many studies on the causes and management of obesity including behavioural studies, physical activity studies, nutritional studies ranging from high-protein low-carbohydrate low-fat, high-carbohydrate low-calorie diets and drugs for the treatment of obesity, yet despite all these efforts the US population continues to increase its weight and similar situations exist in other countries, both developed and developing. In developing countries, obesity coexists with undernourished and malnourished individuals. So far, no country has been able to either prevent overweight and obesity or maintain weight loss of its population.
International organisations and many scientists continue to consider obesity the result of an imbalance between energy intake and expenditure. Citing the law of thermodynamics, scientists and industries articulated the concept of ‘a calorie is a calorie’, which led to the development of a huge weight loss industry, various diets substituting ‘calories for other calories’ and books promoting ‘eat less and exercise more’. These approaches continue to be espoused today, despite the scientific evidence that ‘a calorie is not a calorie’, and that the sources of calories are important in influencing human metabolism and appetite control.4–6 For example, calories from vegetable oils high in linoleic acid (LA), an ω-6 fatty acid, are proinflammatory and thrombogenic, whereas calories from eating fish high in ω-3 fatty acids are anti-inflammatory and antithrombotic. High ω-6 fatty acid intake increases white adipose tissue that is stored and prevents its browning.7 ,8 Furthermore, calories from ω-6 fatty acid intake from vegetable oils high in LA (corn oil, sunflower, safflower, cottonseed, soya bean oil) have different effects on fat tissue development and type than calories from ω-3 fatty acid intake high in α-linolenic acid (ALA) (such as flaxseed oil, canola oil, perilla oil, chia oil). In addition, high ω-6 fatty acid intake leads to an inflammatory state, which is at the basis of obesity and other chronic diseases, whereas calories from ω-3 fatty acids have the opposite effect9 ,10 (box 1 and table 1). ω-6 and ω-3 fatty acids are essential for health and must be obtained from the diet by all mammals including human beings.
Effects of ingestion of eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) from fish or fish oil9
Decreased production of prostaglandin E2 (PGE2) metabolites
A decrease in thromboxane A2, a potent platelet aggregator and vasoconstrictor
A decrease in leukotriene B4 formation, an inducer of inflammation, and a powerful inducer of leucocyte chemotaxis and adherence
An increase in thromboxane A3, a week platelet aggregator and weak vasoconstrictor
An increase in prostacyclin PGI3, leading to an overall increase in total prostacyclin by increasing PGI3 without a decrease in PGI2; PGI2 and PGI3 are active vasodilators and inhibitors of platelet aggregator
An increase in leukotriene B5, a weak inducer of inflammation and a weak chemotactic agent
Opposing effects of ω-6 and ω-3 fatty acids on obesity
We now know that major changes have taken place in the food supply over the last 100 years, when food technology and modern agriculture led to enormous production of vegetable oils high in ω-6 fatty acids, and changed animal feeds from grass to grains, thus increasing the amount of ω-6 fatty acids at the level of LA (from oils) and arachidonic acid (AA) (from meat, eggs, dairy). This led to very high amounts of ω-6 fatty acids in the food supply for the first time in the history of human beings.11–13 Traditionally, animals grazed. Grass contains ALA (ω-3), whereas grains, corn and soya (which are now fed to animals) are high in LA (ω-6). This imbalance in the amount of ω-6 and ω-3 fatty acids is a new phenomenon that was never a part of human evolution11 (figure 1, table 2). Human beings evolved on a diet that had equal amounts of ω-6 and ω-3 fatty acids. This balanced ratio of ω-6 to ω-3 is critical to human development during pregnancy and lactation, in the prevention of chronic diseases and in their management.9 ,14 ,15 The typical Western diet now provides an ω-6 to ω-3 ratio of around 16:1. High dietary intake of ω-6 fatty acids as occurs today leads to increases in white adipose tissue and chronic inflammation, which are the ‘hallmarks of obesity’.7 ,8 ω-6 and ω-3 fatty acids specifically metabolise to prostaglandins, thromboxane and leukotrienes. Prostaglandin E2 from AA leads to differentiation and proliferation of adipose tissue and prostaglandin F2α also from AA prevents the browning of white adipose tissue, which is the good fat tissue as it increases thermogenesis, burning fat through the release of heat.7 ,8 ,16
ω6 to ω3 ratios in various populations
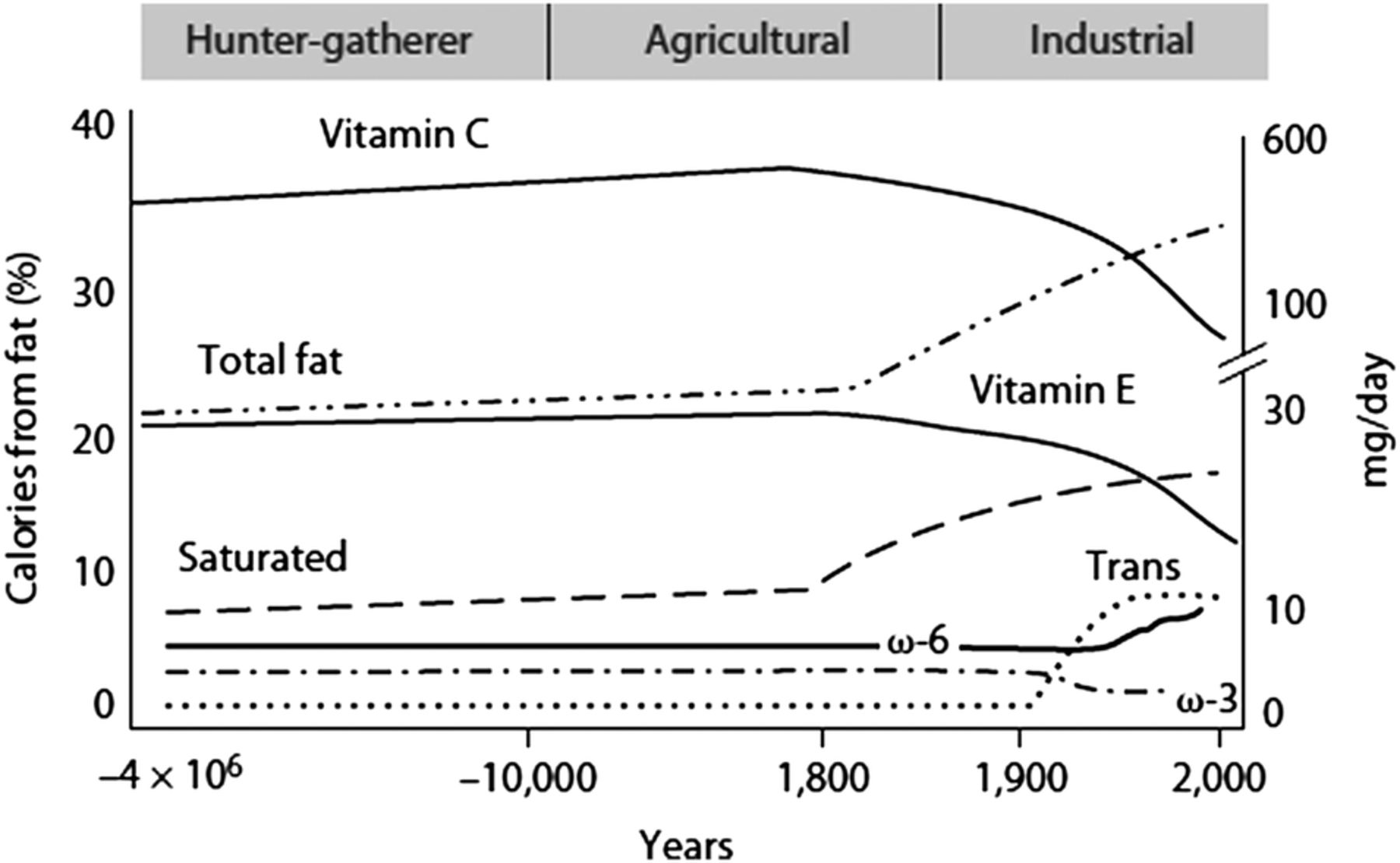
Hypothetical scheme of fat, fatty acid (ω6, ω3, trans and total) intake (as per cent of calories from fat) and intake of vitamins E and C (mg/day). Data were extrapolated from cross-sectional analyses of contemporary hunter-gatherer populations and from longitudinal observations and their putative changes during the preceding 100 years.
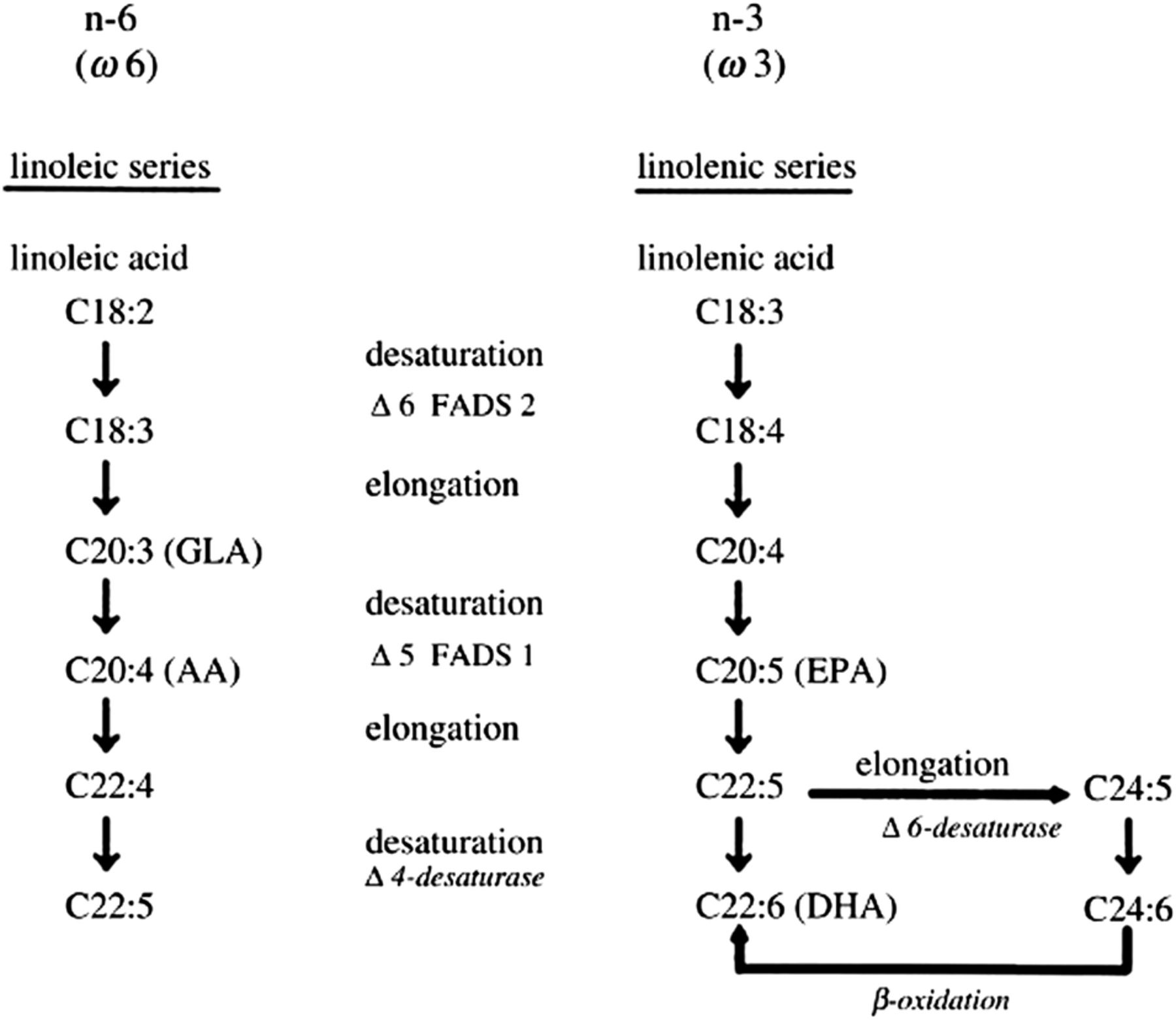
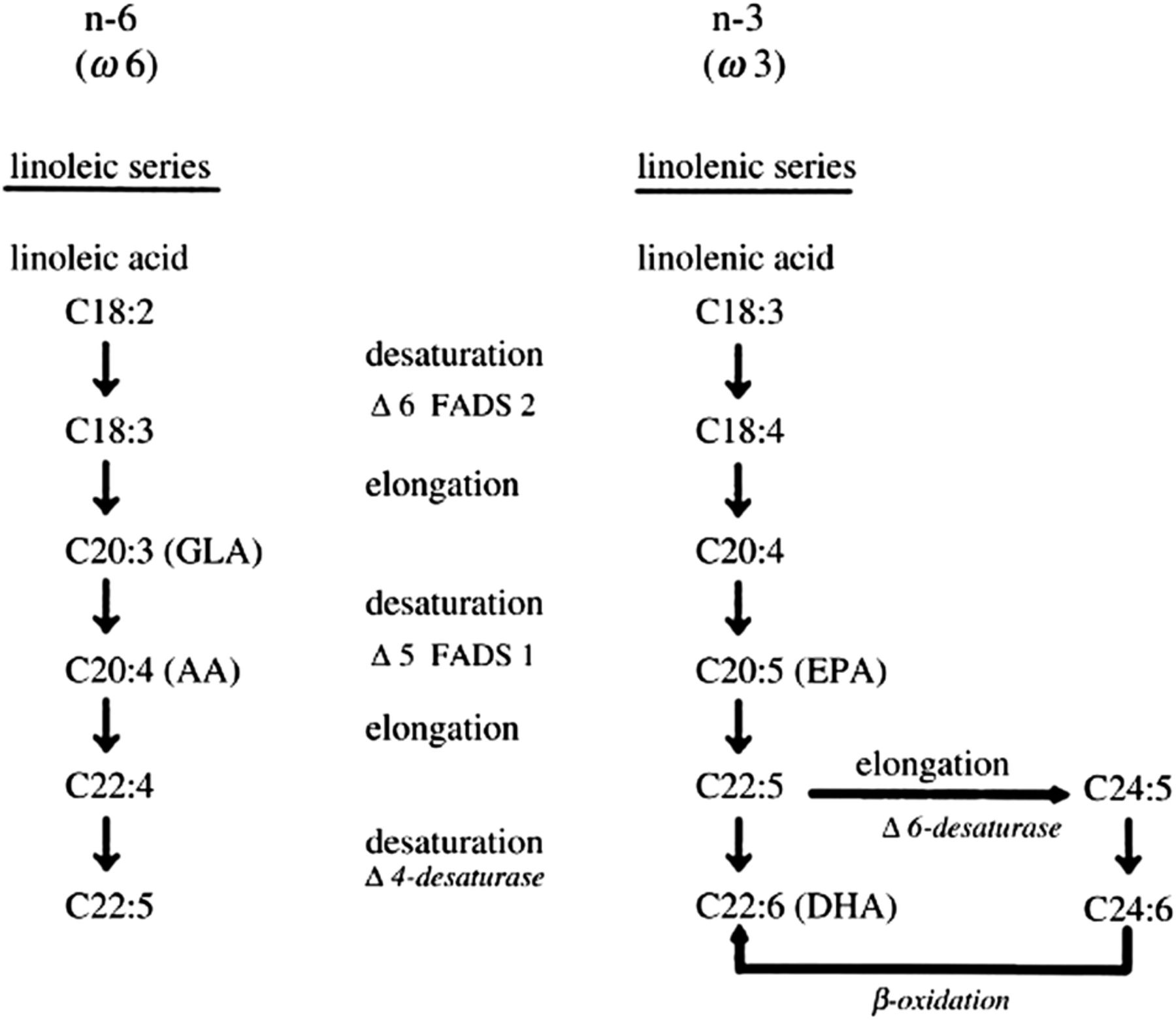
Desaturation and elongation of ω-3 and ω-6 fatty acids. The enzymes Δ6 desaturase and Δ5 desaturase are encoded by FADS2 and FADS1, respectively. AA, arachidonic acid; DHA, docosahexaenoic acid; EPA, eicosapentaenoic acid; FAD, fatty acid desaturase; GLA, γ-linoleic acid.
The ω-6 and ω-3 fatty acids are metabolically and functionally distinct11 (box 1 and table 1). ω-3 fatty acids decrease adipose tissue development and lead to weight loss.17–19 A recent study based on the NIH Women's Health Initiative clearly showed the importance of the ω-6 to ω-3 ratio in weight gain over a period of 10 years in healthy young women.20 High concentrations of ω-6 in red blood cell membrane phospholipids were associated with increased risk of weight gain.20 Similarly, a high ω-6 to ω-3 ratio was also associated with increased risk of weight gain, whereas a high concentration of ω-3 in red blood cell membrane phospholipids was associated with decreased risk. This is a very important study because the investigators used red blood cell membrane phospholipids instead of dietary intake based on food frequency questionnaires that are not as accurate. Dietary frequency questionnaires suffer from two very important deficiencies in carrying out studies on the relationship of essential fatty acids (ω-6 and ω-3). One is the well-known inaccuracy based on the memory of what people ate, and the other is the variation in the endogenous production of ω-6 and ω-3 fatty acids. What is actually being circulated in the blood and in red blood cell membrane phospholipids consists of dietary intake and the endogenous production of ω-6 and ω-3 fatty acids. These two factors account for the discrepancy in epidemiologic, observational and clinical intervention studies along with other factors listed in box 2, which must be taken into consideration while carrying out clinical intervention studies.
Factors that affect outcomes in obesity studies5
Lack to determine the composition of the background diet in terms of ω-6 and ω-3 fatty acids and inflammatory markers, that is, the USA, UK and Northern European countries have the highest amount of linoleic acid (LA) + arachidonic acid (AA) in their diets, which competes with ω-3 polyunsaturated fatty acids (PUFAs); they also have the lowest amount of vegetable and fruit intake, which are needed for optimal absorption of ω-3 PUFA from supplements
Background inflammation
Some studies are using fish and others ω-3 supplements; studies show that a continuous daily intake of ω-3 supplements leads to higher concentrations in the blood than eating fish two times per week
Variation in the dose of ω-3 fatty acids
Variation in the number of subjects
Variation in the severity of disease
Variation in the pharmacologic treatment
Genetic variants predisposing to obesity
Dietary intake by means of questionnaires instead of actual measurements of ω-3 PUFAs in the red blood cell membrane phospholipids or plasma is a major problem that leads to conflicting results
Length of intervention
Genetic variants in the metabolism of ω-6 and ω-3 fatty acids
In the metabolism of the ω-6 and ω-3 fatty acids, there are genetic differences in the population that lead to variations in the amounts of AA (ω-6) and eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) (ω-3) formed from LA and ALA, respectively (figure 2). In European populations, about one-third of the population has genetic variants—haplotype D—that increase the production of AA, from the high LA in the diet. This genetic variation could account for an additional increase of AA of about 25% that is endogenously produced. In Africans, practically 99% of the population carries haplotype D, whereas in African-Americans the frequency is about 50% depending on the admixture of the population.21 ,22 It is obvious then that when carrying out studies, one must include dietary intake and endogenous production represented by measurements of red blood cell membrane phospholipids. A high intake of LA from vegetable oils leads to a disproportionate increase in AA in individuals with haplotype D (genetic variants in fatty acid desaturase (FADS)1 and FADS2) (figure 2), which increases the risk of obesity and its consequences, type 2 diabetes, cardiovascular disease, metabolic syndrome and cancer. Adipose tissue has a requirement for AA for adipose cell differentiation but in amounts equivalent (balanced ω-6 to ω-3 ratio) not a ratio of 16:1 as it is in the US food supply today and other developed countries).23 ω-3 fatty acids (EPA and DHA) decrease adipose tissue and produce lipid mediators—resolvins, protectins and maresins, which are neuroprotective and lead to resolution of inflammation.24 Furthermore ω-3 fatty acids lead to increased fatty acid oxidation and mitochondrial biogenesis.8
There have been many studies using rodents with various results on the effects of ω-6 and ω-3 fatty acids on the genesis and management of obesity, with conflicting results due to differences in animal models, dose of ω-3 fatty acids, observation time, etc. In animals, as in humans, it is very difficult to accurately measure dietary intake. The Fat-1 mouse model bypasses these differences because the ω-3 desaturase controls the formation of ω-3 fatty acids from ω-6, and at all times the amounts remain the same which cannot be done easily and accurately with dietary studies. Using this model, it has been shown that there is a threefold increase in ω-3 fatty acids and a threefold decrease in ω-6 fatty acids, and these changes decrease adipose tissue inflammation and increase 5′ adenosine monophosphate-activated protein kinase (AMPK) activation, which is the gatekeeper of energy.18
Fatty acids act directly on the central nervous system (CNS) and influence food intake, insulin sensitivity and leptin sensitivity. High-fat diets rich in ω-6 fatty acids, as in current Western diets, increase the risk of leptin resistance, diabetes and obesity in humans and rodents.25–27
A diet high in the ω-6 to ω-3 ratio causes an increase in the endocannabinoid signalling and related mediators, which leads to an increased inflammatory state, energy homeostasis and mood.28 In animal experiments, a high ω-6 fatty acid intake leads to decreased insulin sensitivity in muscle and promotes fat accumulation in adipose tissue. Nutritional approaches with dietary ω-3 fatty acids reverse the dysregulation of this system, improve insulin sensitivity and control body fat. A high ω-6 to ω-3 ratio in current Western diets coupled with an increased synthesis of proinflammatory cytokine interleukin 6 (IL-6) from the adipose tissue of an already overweight and obese population propagates obesity by increasing or maintaining chronic inflammation.
It is therefore essential to return to a balanced dietary ω-6 to ω-3 ratio based on data from evolutionary studies,11 the Fat-1 mouse model18 and the results of the NIH Women's Health Initiative clinical study.20 By decreasing ω-6 and increasing ω-3 in the diet, the proadipogenic pathway can be inhibited. The preferred ratio of ω-6 to ω-3 for optimal health is 1:2/1, which is consistent with the evolutionary aspects of diet.29 The time has come to return the ω-3 fatty acids in the food supply and decrease the ω-6 fatty acids by changing the cooking oils (figure 3) and eating less meat and more fish. The composition of the food supply must also change to be consistent with the evolutionary aspects of diet and the genetics of the population. The scientific evidence to balance the ω-6 to ω-3 ratio is robust and necessary for normal growth and development, prevention and treatment of obesity and its comorbidities including diabetes, cardiovascular disease and cancer. This can be accomplished by studies focusing on the metabolism of nutrients, genes and their function.7 ,8 ,30–34 Genome-wide association studies (GWAS) have identified over 90 loci, and many single-nucleotide variants (SNVs) associated with BMI, with the majority of SNVs occurring in non-coding regions of the genome. Claussnitzer et al30 showed how to decipher non-coding regions and have presented a strategy to functionally analyse GWAS. Their study provided evidence that the risk allele rs 1411085 T to C SNV resulted in increased expression of IRX3 and IRX5 genes in preadipocytes, which shifted the development of these cells towards the ‘White Program’ and increased lipid storage, whereas genetic knockdown of IRX3 and IRX5 restored thermogenesis in adipocytes from persons at high risk of obesity. Thus, the risk allele functioned similarly to prostaglandin E2 and prostaglandin F2α from ω-6 fatty acids, whereas the genetic knockdown of IRX3 and IRX5 functioned similarly to ω-3 fatty acid metabolites. AA metabolites prostacyclin and prostaglandin E2 increase white adipose tissue and decrease its browning. Human studies have shown a direct relationship between plasma AA levels and infant body weight, as well as between AA levels in adipose tissue lipids and BMI in children in Cyprus and Crete.35 ,36 AA directly inhibits uncoupling protein-1 (UCP1) gene expression. Considering the high ω-6 to ω-3 fatty acid ratio of Western diets and the role of AA in adipose cell differentiation, proliferation and decreasing browning of white adipose tissue, further research should include studies on the effects of ω-3 fatty acids in blocking the effects of the risk allele (rs 1411085). Clinical intervention studies must take into consideration the background diet, the genetics of the population and be free of confounding factors listed in box 2. It is the responsibility of the governments and international organisations to establish nutrition policies based on science and not continue along the same path of focusing exclusively on calories and energy expenditure, which have failed miserably over the past 30 years.

{kind=link}
{kind=link}
{kind=link}
The fatty acid content of common fats and oils. The chart shows the percentage of saturated fatty acids, monounsaturated fatty acids, linoleic acid and α-linolenic acid in 13 commonly used fats and oils.38
References
Supplementary materials
Press release
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter Follow James J DiNicolantonio at @drjamesdinic
Contributors APS conceived and outlined the paper, JJD provided additional input and references and both authors finalised the paper.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.