Article Text

Abstract
Objective Ideal cardiovascular health (CVH) was developed to promote CVH as a key component of primordial prevention. Mobile short message service (SMS) is useful for improving health behaviours. We aim to test the effectiveness of SMS intervention in women to improve CVH.
Methods In a single-blinded, randomised, controlled study, 620 women, aged 35–70 years, without cardiovascular disease, were enrolled in SMS intervention versus no SMS. CVH metrics by self-report, and biochemical laboratory, anthropometric and blood pressure measurements were collected during home visits at baseline and 9 months. Women were categorised as having poor (0–2), intermediate (3–4) or ideal (5–7) CVH according to the number of ideal CVH metrics. Participants were randomised 1:1 to SMS intervention versus control. SMS was sent every 5–6 days for 9 months. The primary outcome was the difference in the proportion of women with ideal CVH between SMS and control groups at 9 months. Rates of intermediate CVH, poor CVH and each of the seven ideal CV health metrics at 9 months were key secondary endpoints.
Results At 9 months, there was no significant difference between groups for the primary outcome (16.3% at baseline and 13.3% at 9 months, and 10.1% and 11.1%, in SMS and control groups, respectively, adjusted RR 1.0; 95% CI 0.6 to 1.6). Similarly, there were no significant differences between groups for the key secondary endpoints. SMS had an acceptance rate of 94.9%.
Conclusions Behavioural SMS intervention did not improve rates of ideal CVH in women, despite being feasible and well received.
Trial registration number 6377.
- RISK FACTORS
- Global Health
- Outcome Assessment, Health Care
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Mobile text messaging is a strategy that has been successfully used in primary prevention to modify individual risk factors, such as smoking cessation and obesity.
In secondary prevention, results have been discordant, with some studies showing positive results and others no improvement.
Our group has previously demonstrated in a randomised group of hypertensive patients that mobile text messaging improved adherence in the intervention group.
Few studies have aimed at modifying health behaviours with text messaging, and none have aimed to change ideal cardiovascular health prevalence.
WHAT THIS STUDY ADDS
A 9-month randomised mobile text message intervention directed to improve several cardiovascular risk factors and behaviours at the same time in women did not modify the prevalence of ideal cardiovascular health (CVH) in a group of Latino women.
Short message service, as the unique intervention strategy to modify ideal CVH, was unsuccessful in this population.
Mobile text messaging was well received by women and proved to be a feasible tool for communicating with the community.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Mobile text messaging, as a unique strategy, to improve multiple cardiovascular risk factors and behaviours, could be insufficient to achieve these changes.
This study encourages seeking complementary tools along with text messages, to improve ideal cardiovascular health goals.
Introduction
Cardiovascular disease (CVD) remains the leading cause of death worldwide, with increasing rates of CV risk factors (RFs) contributing to this phenomenon.1 In Chile, the prevalence rates of obesity, overweight and diabetes are among the highest worldwide, especially among women, despite the implementation of public health policies designed to address this problem.2 3 It is particularly alarming that not only rates of metabolic RFs are worse in Chilean women than in men, but also women’s mortality from myocardial infarction continues to be twice that of men, and CVD awareness is very low among women.4–6 Also, women have been understudied, underdiagnosed and undertreated in CVD worldwide.7
In 2010, the American Heart Association (AHA), to reconfigure CVD preventive strategy, proposed the concept of ideal CV health (CVH) to encourage the population to achieve seven ideal behaviours and factors: not smoking, a healthy diet, moderate or intense physical activity, normal weight, blood pressure (BP) <120/<80 mm Hg, fasting blood glucose <100 mg/dL and total cholesterol <200 mg/dL8. Data from the National Health and Nutrition Examination Survey in the USA have demonstrated a direct relationship between the number of ideal CVH metrics and mortality, with Yang et al9 reporting that individuals with six out of seven CVH metrics had significantly lower risks of all-cause, CVD-related and ischaemic heart disease-associated mortality compared with those with ≤1 ideal CVH metric. Numerous studies have since reported the low prevalence of ideal CVH in different populations, emphasising the need to increase awareness about ideal CVH to reduce CVD risk.10 11 To that end, health promotion/awareness at the population level and CVD prevention at the individual level are critically important.
Mobile text messaging through short message service (SMS) is a strategy widely used in smoking cessation and obesity.12 However, evidence supporting its widespread use for health promotion is insufficient, mainly because studies have not been randomised, and the reviews are heterogeneous.13 Even fewer studies have aimed at modifying health behaviours with SMS.
The primary objective of this study was to evaluate the prevalence of ideal CVH in women in Santiago de Chile after a randomised and blind educational intervention through SMS.
Methods
Data and methodology will be made available to other investigators to replicate this study procedure on reasonable request.
Study design and participants
ESCI (Spanish name ‘Estudio de Salud Cardiovascular Ideal en Mujeres’) was a parallel-design, single-blinded, randomised controlled study of women enrolled to receive SMS for 9 months to promote the seven ideal CVH metrics and behaviours compared with a control group. We recruited eligible women from Santiago de Chile, Metropolitan Region, representing approximately 40% of the Chilean population and 52 boroughs or districts. The recruitment phase was held between 12 May 2015 and 22 August 2015.
Women were eligible if they were 35–70 years old, residents of the Metropolitan Region, had access to mobile phones to read text messages (in use and functioning) and could provide informed consent. Pregnant women and those with a history of stroke, myocardial infarction and renal failure on dialysis were excluded.
The study was done using a probabilistic, multistage and geographically stratified design to achieve a good representation of Chilean women. The details of the study sample design have been described previously.14 Briefly, the sample selection considered the districts/boroughs’ classification according to the following criteria: socioeconomic level and predominance of women within specific age ranges. Nine sampling strata were then formed after clustering three socioeconomic levels (low, medium low and medium high) and three age groups (35–44, 45–54 and 55–70) at the borough level. In each of the nine sampling strata, two boroughs were selected, establishing each one as a primary sampling unit. From each 1 of those, 12 blocks were determined using a systematic random selection method with probability proportional to the housing units. From these housing units, women were recruited from randomly selected residential dwellings.
The Centro de Estudios y Encuestas Longitudinales of the Pontificia Universidad Católica de Chile conducted the fieldwork.
Patient and public involvement
Patients and the public were not involved in the design and conduct of this research.
Randomisation and treatment assignments
Randomisation was done in a 1:1 ratio through a computerised program using a Bayesian method after collecting participants’ baseline data. Randomisation was stratified by age group, socioeconomic level and the number of ideal CVH metrics to ensure a balance in participant characteristics in both study arms. Study subjects were aware of their treatment allocation considering the study design. Clinical staff and investigators, except for the study coordinator, were blinded to treatment randomisation. The study coordinator interacted with the text messaging company, Step Therapy (Santiago, Chile), a company that develops text messaging systems focused on healthcare.
Intervention
The socialcognitive theory was used to develop a bank of text messages about education, motivational change and recommendations regarding the seven ideal CVH behaviours and factors.15 A multidisciplinary team with experience in CVD prevention (two nurses, one dietitian, one physical therapist, one psychologist and two cardiologists) selected the messages through a systematic approach. The messages were not personalised and were written using formal but colloquial language. Each message consisted of a maximum of 160 characters. Women in the intervention group received an equal number of messages related to each one of the ideal CV metrics (ie, no metric was prioritised), and the messages were sent automatically. Message delivery status (ie, delivered successfully vs not delivered) was monitored. Messages that were not delivered were resent once during the same day.
Messages were sent every 5–6 days for 9 months, starting at randomisation. All messages were sent during normal working hours from Monday to Friday. The SMS system was unidirectional, meaning participants could not reply. When two messages were undelivered, the study coordinator contacted the participant or a participant’s relative to make inquiries. Table 1 provides examples of messages used during the study (translated into English). All participants, including those in the control arm, received a letter by certified mail with their laboratory data (at baseline and 9 months) including recommendations associated with the results.
Sample text messages sent to participants in the intervention group (translated into English)
Outcomes
The primary outcome was the difference in the proportion of women with ideal CVH (defined as having 5–7 metrics) between the intervention and the control groups at 9 months.
Secondary outcomes were the changes in the proportion of women with intermediate CVH and poor CVH at 9 months and the changes from baseline to 9 months in rates of each of the seven ideal CV health metrics. As exploratory outcomes, we analysed the changes in each one of the individual CVH diet components at 9 months.
Data and biochemical variables collection
ESCI’s baseline and 9-month-visit data were collected during home visits (two for each milestone). At the first visit, a study nurse conducted a face-to-face interview using an electronic tablet. During the second visit, BP and anthropometric measurements and blood and urine samples were collected. The survey used during the interview was designed by a multidisciplinary team including an expert in survey methodology. It included the Global Physical Activity Questionnaire (GPAQ)16 for physical activity assessment, the Patient Health Questionnaire (PHQ 9)17 for depression, questions about CV RFs, family history of CVD and dietary habits. The study nurse used nutritional sheets and serving-size instruments to achieve more accurate responses to the diet questionnaire. Socioeconomic (ie, total family income) and sociodemographic (ie, marital status, years of education, type of health insurance and employment status) data were assessed based on the 2011 CASEN Survey.18
BP was measured with a brachial automatic validated monitor (Model HEM7200, OMROM Healthcare) after 5 min of resting in a sitting position. Three measurements were taken every 2 min, and the mean was recorded. Weight and height were measured using a digital weight (Seca model 803; Germany) and a stadiometer. Body mass index (BMI) was calculated using the standard formula.
Venous blood samples were obtained after a minimum of 8 hours of fasting and alcohol withdrawal of 24 hours. We determined total cholesterol levels, glycaemia and creatinine plasma levels. With a morning isolated urine sample, we obtained urinary creatinine and sodium to calculate estimated 24-hour salt consumption.19
Ideal CVH metrics and definitions of CV RFs
Ideal CVH was defined by the seven health metrics proposed by the AHA8: (1) no smoking or quit ≥12 months ago; (2) BMI <25 kg/m2; (3) moderate exercise ≥150 min/week or vigorous ≥75 min/week or combination, (4) healthy diet (4–5 of the following components: fruits and vegetables ≥4.5 cups/day; fish 3.5 oz servings ≥2 servings/week; sodium <1500 mg/day; sweets/sweetened beverages ≤450 kcal/week; whole grains ≥3 servings/day) (5) total cholesterol <200 mg/dL (untreated); (6) BP <120/80 mm Hg (untreated) and (7) glycaemia <100 mg/dL (untreated). We defined poor, intermediate and ideal CVH based on the presence of 0–2, 3–4 and 5–7 ideal health metrics, respectively.
In this study, smoking was defined as having smoked ≥1 cigarette in the last month. Women with a medical diagnosis of hypertension, with or without pharmacological treatment and those with a mean BP >140/90 mm Hg were defined as having hypertension. Dyslipidaemia was defined as having a medical diagnosis of hypercholesterolaemia with or without pharmacological treatment or having a total cholesterol ≥200 mg/dL. Lastly, diabetes was defined as having a medical diagnosis of diabetes with or without pharmacological treatment or having fasting glucose ≥126 mg/dL.
Definition of socioeconomic status and educational levels
The socioeconomic levels were classified into three groups: low, medium low and medium high, determined by the geographical area of the respondent’s residence and based on the total per capita income of the resident households of each borough. Education level was categorised by asking for the years of formal education and the highest qualification received and divided into three categories: low (primary school or less; 0–8 years), middle (complete or incomplete secondary education; 9–12 years) and high (complete or incomplete university or technical studies; >12 years).
Statistical analysis
A sample size of 635 women was calculated assuming a confidence level of 95% with a statistical power of 80%, to detect an absolute difference of 10% between the intervention and control groups for 9 months, based on an ideal CVH prevalence of 10% according to data from Chile and other countries.20 The estimated allowed sample loss was 15%. All interventional analyses were conducted using the intention-to-treat principle.
Results are presented as mean±SD or frequency (percentage) when suitable. Univariate comparison of prevalence of ideal CVH components at baseline and end of the study was done by Fisher’s exact tests. Continuous measurements were compared by Student’s t-tests or Wilcoxon tests for distributions departing from normal. Changes in primary and secondary outcomes comparison between groups were done by logistic regression. Paired changes in continuous variables were analysed with paired t-tests. Relative risks were causing means of binomial regression models. We considered the results as statistically significant for p<0.05.
Results
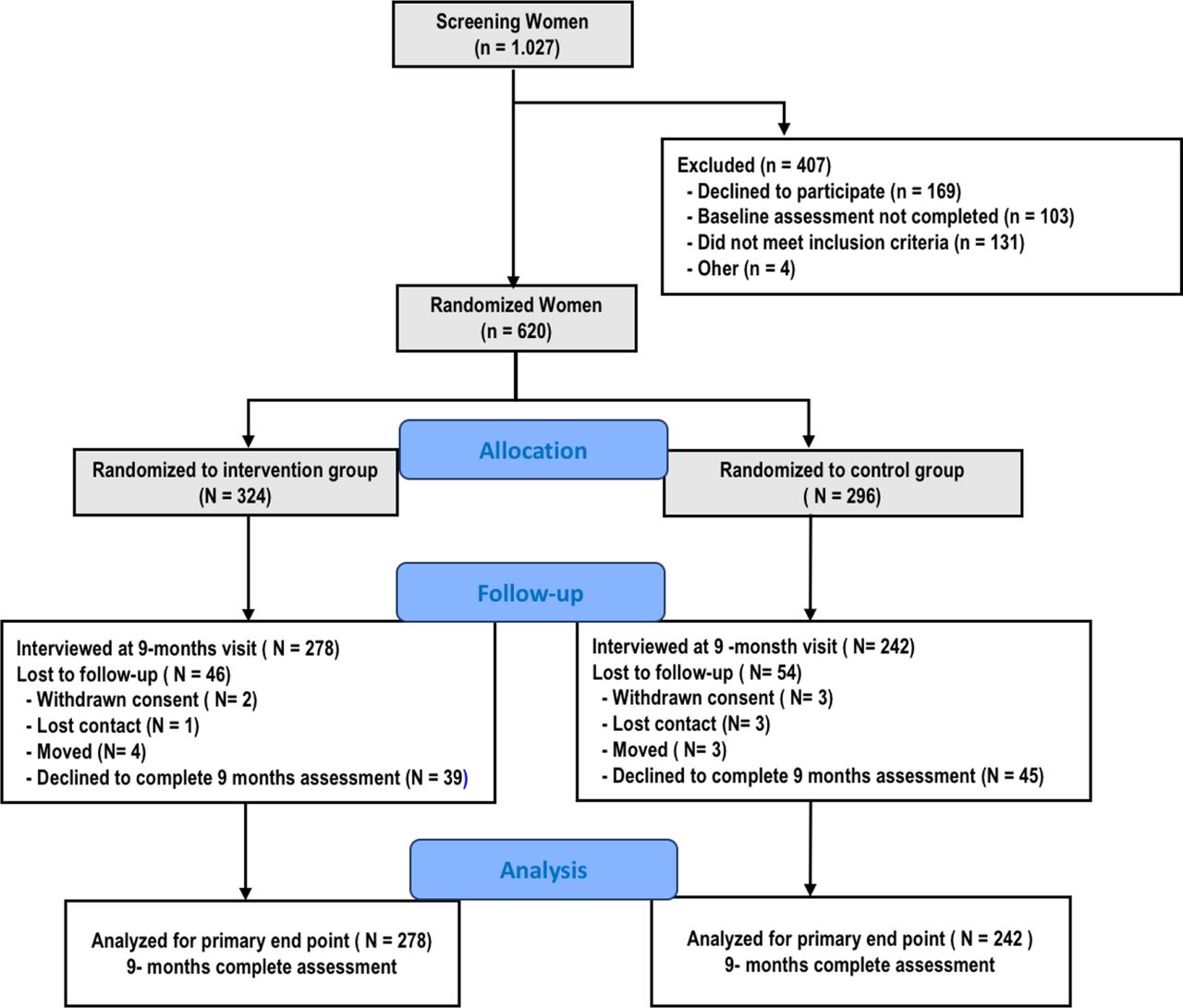
Between 4 July 2015 and 10 November 2015, 1027 women were screened for eligibility. Among these, 620 women were enrolled and randomly assigned to the intervention SMS group (n=324) or control group (n=296). The median follow-up was 9 months. At the end of the study, 46 subjects were lost to follow-up in the intervention group and 54 in the control group (figure 1). At baseline, the only significant differences between groups were the mean systolic BP and the ideal BP <120/80 mm Hg (table 2). The mean age was 52±9 years, and the median (IQR) years of education were 8 (4). Overall, there were high rates of CV RFs in the study cohort (table 2). The prevalence of ideal CVH was 14.3% for the study population, with the majority of women having an intermediate CVH (57.1%).
Baseline characteristics of the study population
{kind=link}
Participant flow diagram.
Throughout the study, 11 664 messages were sent, and there was an 11% rate of failed delivery secondary to defective data reception (ie, mobile cell phone not working or with weak reception covering the area) or participant problems (ie, women who did not open messages or who had a full mailbox).
Primary outcome results
In the intervention group, the mean prevalence of ideal CVH was 16.3% at baseline and 13.3% at the end of the study; in the control group, the mean of ideal CVH was 10.1% and 11.1% at the end of the study (table 3). The difference in the proportion of participants who had an ideal CVH at 9 months was not statistically significant between groups (adjusted RR 1.0; 95% CI 0.6 to 1.6) (table 3).
Primary and secondary outcomes analysis at 9 months
Secondary outcomes
No significant differences were observed for poor or intermediate CVH prevalence between groups. Similarly, there were no significant differences for most CVH metrics, except for ideal BP (RR 1.27: 95% CI 1.0 to 1.6, p=0.03), even after adjusting for baseline differences. There was a trend for more women having total cholesterol <200 mg/dL at 9 months in the intervention group compared with the control group (RR 1,1: 95% CI 1.0 to 1.3, p=0.14). (table 3).
Perception and opinions about mobile text messaging
Of the 213 women who remembered receiving health-related SMS during the last 9 months, only 2.8% reported disliking receiving SMS (table 4). The vast majority of women were willing to continue receiving messages (95.3%), with 93.9% stating they would recommend to others to receive healthy lifestyle SMS. Weekly SMS was preferred by the majority of women.
Intervention participants’ perceptions and opinions of mobile text messaging programme
Discussion
ESCI showed that a 9-month SMS intervention did not significantly increase the prevalence of ideal CVH in urban Chilean women. SMS intervention was well received and feasible, with low rates of participant dissatisfaction and failed message delivery.
CV RFs are highly prevalent in the general population in the Southern Cone of Latin America, including Chile.21 Despite multiple public health policies to reduce the prevalence of these RFs, both at the community level and individual level, the burden of CV risk continues to increase. Therefore, it is important to seek new strategies to intervene. To our knowledge, ESCI is the first randomised clinical study conducted on women incorporating SMS to intervene in CVD-health behaviours and RFs in Latin America. The achievement of ideal CVH in women may help in decreasing CVD morbimortality in the next decades, especially in young women, in whom there has been an increment in myocardial infarction prevalence in the last 20 years.22
Studies evaluating the effects of SMS on health behaviours have yielded disparate results. Other international studies with this technology in primary prevention have successfully addressed individual RFs, such as weight loss or smoking cessation, with favourable results.23 24 These studies, rather than trying to reduce the whole burden of disease, pointing to several RFs at the same time, targeted a less ambitious endpoint. Indeed, our group had previously demonstrated that SMS increased antihypertensive drug adherence in hypertensive patients within the community.25
The TEXT ME study,26 conducted in patients with established coronary heart disease (CHD), demonstrated modest but significant improvements in low-density lipoprotein cholesterol levels at 6 months as well as improvements in systolic BP, BMI and physical activity. By contrast, the Cardiovascular Health and Text Messaging (CHAT) study27 showed no significant improvements in CV RF management with SMS . The above studies were conducted in CHD populations and treated by guideline-directed therapy. Our study was performed in a primordial prevention cohort, where changes in lifestyle behaviours are challenging. In concordance with ESCI, the TextMe 2 study performed in a moderate-high CV risk primary prevention cohort also showed no significant differences with an SMS intervention in the primary endpoint. Klimis et al28 claimed sample size and loss of follow-up as the main reasons for their results. We had a significant loss of follow-up, with a discontinuation rate of over 20%, that primarily affected our estimated sample size calculation to have differences between groups. However, we cannot assure our negative results only based on the participant’s lost to follow-up. Also, we only sent one SMS every 5–6 days which could have affected our results. TextMe2 study sent four SMS per week. However, we based this decision on our previous study on hypertensive patients. In this regard, the ideal number of SMS per week to achieve differences in CV health parameters has not been definitively ascertained. ESCI and TextMe 2, both resulted negative. Finally, the kind of intervention in itself could have precluded better results. Intervention through text messaging pointing to modifying multiple CVRF could not be the only strategy in the community. Probably, it needs to be complemented using an integrated-multiple-tool strategy physician directed and nurse managed such as community meetings, individual phone calls, web-based health interventions (groups and individually) and the support of an interactive programme device application.29–31
ESCI was ambitious for striving to effect change in the composite of ideal CVH, which meant to achieve an ideal condition in ≥5 CV metrics simultaneously. Moreover, the ideal CV parameters demand very strict goals, such as ideal BP and weight, which are difficult to pursue in postmenopausal women. In general, achieving changes in health behaviours is complicated. Women included in our study were representative of those in a nascent developed country with high rates of working outside the home, primary caregiving of children and stress.2 3 32 These factors, among others, may have interfered with the ability of the single intervention of SMS to change health behaviours. Indeed, it has been proposed that multifaceted approaches to CVD prevention are necessary to make a difference in women’s health.33 34
SMS technology was well received by our participants, as discussed previously. Our study demonstrated that SMS intervention was feasible, easy to administer and understand, and could be delivered without in-person contact. As such, this approach could become a desirable means of education/motivation, especially during difficult times to have in-person visits such as the last pandemic period.
Our study has limitations. A larger sample size may have provided a better ability to detect differences between treatment arms. In addition, we experienced a higher loss of follow-up than anticipated, emphasising the need for better retention strategies. Also, we had a limited number of messages as discussed previously, and they were depersonalised. Finally, we did have differences in baseline ideal BP between groups. We tried to surpass this limitation by adjusting the results by binomial logarithm regression as done by other similar studies.28
In conclusion, ESCI, the first randomised SMS intervention study targeting ideal CVH in Latino women, did not demonstrate a significant impact on increasing the prevalence of ideal CVH in this community. However, SMS was feasible and well accepted by study participants. SMS could become a complementary tool to provide education and motivation about healthy behaviours, along with an integrated CVH preventive programme for women.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Santiago East Metropolitan Region Ethics Committee on 27 January 2015. Participants gave informed consent to participate in the study before taking part.
References
Footnotes
Contributors Conception and design of the research: MA, PV and CC-C. Acquisition of data: CC-C, AB, GV and RL. Analysis and interpretation of data: MA, PV, SCS, GV. Statistical analysis: CN. Obtaining financing: MA and PV. Writing of the manuscript: MA and PV. Critical revision of the manuscript for intellectual content: all authors. Authors responsible for the overall content as guarantors: MA and PV.
Funding This study was supported by an unrestricted grant from the American Heart Association and the Fundación SOCHICAR of the Chilean Society of Cardiology and an unrestricted grant from TEVA Pharmaceutical Industries to the principal investigators, MA, MD, and PV, MD.
Competing interests MA has served on an advisory board for AstraZeneca, Bayer, Novo Nordisk, Boehringer, Tecnofarma, Axon Pharma, Novartis and has received fees for speaking from AstraZeneca, Boehringer Ingelheim, Bayer, Novo Nordisk, Tecnofarma, TEVA Pharmaceuticals, Abbott, Axon Pharma, Elli Lilly. PV has served on advisory boards for Axon Pharma, Novo Nordisk, Boehringer Ingelheim, Novartis, and has received fees for speaking from: Boehringer Ingelheim, AstraZeneca Novo Nordisk, Axon Pharma, Abbott, Bayer and Tecnofarma, Organon, Teva Pharmaceuticals and fees for being the principal investigator for the following Clinical Studies: Horizon (Novartis)/ Victorion Prevent (Novartis).
Provenance and peer review Not commissioned; externally peer reviewed.