Article Text

Abstract
Objective To prospectively assess the value of coronary CT angiography (CTA) in asymptomatic patients with high ‘a priori’ risk of coronary artery disease (CAD).
Methods 711 consecutive asymptomatic patients (61.8 years; 40.1% female) with high ‘a priori’ risk of CAD were prospectively examined with a coronary calcium score (CCS) and CTA. Coronary arteries were evaluated for atherosclerotic plaque (non-calcified and calcified) and stenosis (mild <50%, intermediate 50–70% or high-grade >70%). Coronary Segment Involvement Score (SIS, total number of segments with plaque) and nc (non-calcified) SIS were calculated. Primary end points were major adverse cardiac events (ST-elevation MI, non-ST-elevation MI and cardiac death); secondary end points were coronary revascularisation and >50% stenosis by invasive angiography.
Results Of 711 patients, 28.3% were negative for CAD and 71.7% positive (CAD+) by CTA (15.6% had plaques without stenosis, 23.9% mild, 10.7% intermediate and 21.5% high-grade stenosis). CCS zero prevalence was 306 (43%), out of those 100 (32.7%) had non-calcified plaque only. Mean follow-up period was 2.65 years. MACE rate was 0% in CAD negative and higher (1.2%) in CAD positive by CTA. Coronary revascularisation rate was 5.5%. Patients with SIS ≥5 had an HR of 6.5 (95% CI 1.6 to 25.8, p<0.013) for MACE, patients with ncSIS ≥1 had an HR of 2.4 (95% CI 1.2 to 4.6, p<0.01) for secondary end point. The sensitivity of CTA for stenosis >50% compared with invasive angiography was 92.9% (95% CI 83.0% to 98.1%). Negative predictive value of CTA was 99.4% (95% CI 98.3% to 99.8%) for combined end points.
Conclusions CAD prevalence by CTA in asymptomatic high-risk patients is high. CCS zero does not exclude CAD. CTA is highly accurate to exclude CAD. Total coronary plaque burden and nc plaques, even if only one segment is involved, are associated with an increased risk of adverse outcome.
- CORONARY ARTERY DISEASE
- IMAGING AND DIAGNOSTICS
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Key messages
What is already known about this subject?
-
Asymptomatic patients without chest pain symptoms but a high coronary risk profile carry a higher risk of myocardial infarct. Currently, CT Calcium Scoring (CCS) is recommended for risk stratification in this cohort.
What does this study add?
-
Coronary CT-Angiography adds values over CCS in terms of providing quantification of total and non-calcifying coronary plaque burden (SIS and ncSIS score) and stenosis graduation (mild, intermediate and severe). Our study shows that beyond coronary calcium, non-calcifying plaque burden as well predicts outcome.
How might this impact on clinical practice?
-
Coronary CT-Angiography should be considered in asymptomatic patients with high life-time risk of CAD as more accurate screening tool for CAD due to its ability to detect non-calcifying plaques and to quantify plaque burden (SIS and ncSIS score), as well as coronary stenosis severity graduation.
Introduction
Myocardial infarction (MI) in previously asymptomatic patients with subclinical coronary artery disease (CAD), who remain undetected with conventional screening methods, is linked with high morbidity, mortality and socioeconomic burden.
Further, asymptomatic ‘silent’ myocardial ischaemia increases the likelihood of future coronary events, particularly in healthy males.1–3
Coronary calcium scoring (CCS) using CT is recommended in asymptomatic patients with low or intermediate risk of CAD for detection of calcifying plaque.4 ,5 Screening of asymptomatic patients with intermediate-to-high risk of CAD by coronary CT angiography (CTA) is currently under debate and was graded as an uncertain but potentially useful clinical application according to 2010 ACCF/SCCT/ACR guidelines.5
CTA has the unique advantage over CCS of detecting non-calcifying plaques in addition to calcifying lesions,6 thus allowing for direct visualisation of early atherosclerosis stages such as lipid and fibrous atheroma, which are risk factors for future coronary events.7 Long-term studies report of an increased risk of adverse outcome associated with vulnerable fibroatheroma, whereas calcifying lesions tend to remain rather stable.8
Studies investigating the accuracy, outcome and, thus, the diagnostic benefit of coronary CTA (CCTA) in asymptomatic patients are scarce.9–12
Higher radiation exposure of 12 mSv using 64-slice CTA13 was an issue of concern for using CTA as a widespread screening tool in asymptomatic patients. A variety of recently introduced new CT-technologies such as high-pitch CTA, prospective ECG-triggering and iterative reconstruction reduce the radiation dose to 1 mSv or even less, thus equalising the radiation exposure of CCS and CTA.14 ,15
Therefore, the purpose of this study was to assess the value of CCTA in an asymptomatic patient cohort with high ‘a priori’ risk of CAD based on risk profile and conventional tests and to identify risk factors for adverse outcome (major adverse cardiac events (MACE) and coronary revascularisation).
Methods
Study design
Seven hundred and eleven asymptomatic, consecutive patients referred to CCTA between 2005 and 2012 were included into this prospective. IRB approved study.
Inclusion criteria were: asymptomatic patients with low, intermediate or high Framingham risk profile based on conventional risk factors. Blood tests were performed within a maximum of 14 days prior to CT and definitions were made according to the most recent ESC guidelines: arterial hypertension (systolic blood pressure (SBP) >140 bpm or diastolic BP >90 bpm), dyslipidaemia (total cholesterol >200 mg/dL or high-density lipoprotein <40 mg/dL), family history (MI or sudden cardiac death in an immediate male relative <55 years or female<65 years), smoker (current smoker or those who quit in the past 6 months) and diabetes.16 ,17
A preceding non-invasive ECG-treadmill stress test was scheduled. The patients were included if the test was inconclusive (eg, low physical performance), not feasible due to comorbidity or incompliance, not specific pathological (eg, premature ventricular contraction, arterial blood pressure increase, arrhythmia, etc) or borderline or mild positive for myocardial ischaemia (ST-segment depression of 1–2 mV).18
Patients were finally included if they had a high ‘a priori’ risk of CAD defined as: either a (1) high-‘lifetime’ cardiovascular risk estimated by Berry et al19 including patients with diabetes or (2) low lifetime risk19 but a borderline or non-specific mild pathological ECG-treadmill stress test result (see criteria above)
After a minimum of 1 year up to 8 years, follow-up was performed via phone call and examining the cardiologist’s or hospitalisation chart results of the patient. Our centre is the only invasive coronary angiography (CAG) and cardiac surgery unit in a large geographic area (200 km). Outcome data, including MACE, death (cardiac vs non-cardiac), invasive angiography (IA) results (stenosis >50%) and coronary revascularisation procedures (either via percutaneous coronary intervention (PCI) or coronary artery bypass grafting (CABG)) were collected.
Exclusion criteria were: renal dysfunction (serum GFR <60 mL/min/1.73 m2), hyperthyroidism, iodine allergy, pregnancy, known CAD, previous PCI or CABG or previous myocardial infarction/acute coronary syndrome.
Multislice CT
From December 2005 until December 2009, a 64-slice CT (Somatom Sensation 64, Siemens, detector collimation 64×0.75 mm, rotation time 0.33 s) was utilised. From December 2009, CTA exams were performed using a 128-slice dual source CT (DSCT) (Somatom Definition Flash, Siemens).
First, a non-contrast-enhanced CCS standardised CT scan (detector collimation 64×1.5 mm, 120 kV, ECG-gating, slice thickness 3 mm and heart view medium smooth kernel B 35 f) was performed and the Agatston Score was calculated.20
Second, CCTA was performed. Scan parameters for 128-DSCT (Somatom Definition Flash, Siemens) and 64-slice CT (Somatom Sensation 64, Siemens) were: detector collimation 2×64×0.6 mm with a z-flying spot and 64×0.6 mm, rotation time 0.28 and 0.33 s, respectively. Patients were scanned in supine position in mid-inspiration breath-hold while an ECG was recorded.
Based on the patient’s individual heart rate (HR) and body mass index (BMI), different scan protocols were used. For 128-DSCT, prospective ECG-triggering was applied for regular HR <65 bpm (either high-pitch FLASH-mode (pitch 3.4) if HR was <57 bpm and BMI <24 or sequential mode in the remaining) and retrospective ECG-gating was used for patients with HR >65 bpm or irregular HR. For 64-slice CT, retrospective ECG-gating was applied.
Tube voltage was 100 kV in patients with BMI <26 kg/m³ and 120 kV in BMI >26 kg/m2.
An iodine contrast agent (CA) with 370 mg/mL iodine concentration (Iopromide, Ultravist 370, Bayer Schering Pharma, Berlin, Germany) was triggered into arterial phase, applying bolus tracking technique, while initiating the CT scan at a threshold of 100 Hounsfield units (HU). The CA volume ranged between 65 and 120 cc depending on the individual patient’s body weight, iodine delivery rate and scan time using a standardised scheme. The CA was injected intravenously at a flow of 4–6 mL/s followed by a 40 cc saline solution bolus using an automated injector.
Axial images were reconstructed with 0.75 mm slice width (increment 0.4), a medium-smooth reconstruction (B 26 f) and evaluated using multiplanar reformation for presence of stenosis less than 50%, 50–70% stenosis or greater than 70%. The presence and quality of coronary plaques (non-calcified, mixed or calcified) were assessed for each coronary segment by one experienced observer (10 years of training, equivalent to ACCF/AHA level 3 accreditation) on a per segment basis (AHA modified 16-segment classification).21
Coronary atherosclerosis: per-segment-based plaque involvement
The segment involvement score (SIS) was used as a quantifying measure of coronary plaque. Each segment was scored individually as 0 or 1, based on the presence of plaques, irrespective of the degree of stenosis. The sum of all involved segments (ranging from 0 to 15) was calculated for each patient.22
Similarly, a non-calcified segment involvement score (ncSIS) was calculated. Only non-calcified hypodense plaques23 without any calcification (HU <130) were included, and all involved segments summed.
Outcome analysis
Primary end point was any MACE including ST-elevation MI (STEMI), non-ST-elevation MI (NSTEMI) acute coronary syndrome or cardiac death. Non-cardiac deaths were not defined as MACE.
Secondary end points were defined as (1) coronary revascularisation rate (PCI or CABG) and (2) coronary stenosis >50% by IA.
Statistical analysis
Statistical analysis was performed using SPSS software (V.17.0, SPSS Inc, Chicago, USA) and MedCalc (V.12.5, MedCalc Software bvba, Belgium). Quantitative variables are expressed as means±SD and categorical variables are presented as absolute values and percentages. A p value of less than 0.05 was considered statistically significant. Group comparisons were performed using χ2 test or Fisher's exact test for categorical variables.
Kaplan–Meier log-ranked survival probability analysis was applied for the different CTA groups (stenosis severity) for primary and secondary end points. Receiver operating curve (ROC) analysis (C-index) was performed for CCS and CTA compared with stenosis >50% in IA. ROC pairwise comparison using DeLong's method was applied to test for differences among the predictive value of CCS and CTA stenosis >50%.
The risk for adverse outcome was calculated for SIS and ncSIS scores using Cox proportional hazard risk model (DeLong’s approach), and thresholds were tested stepwise with increments of 1 until a statistically significant level was reached.
Results
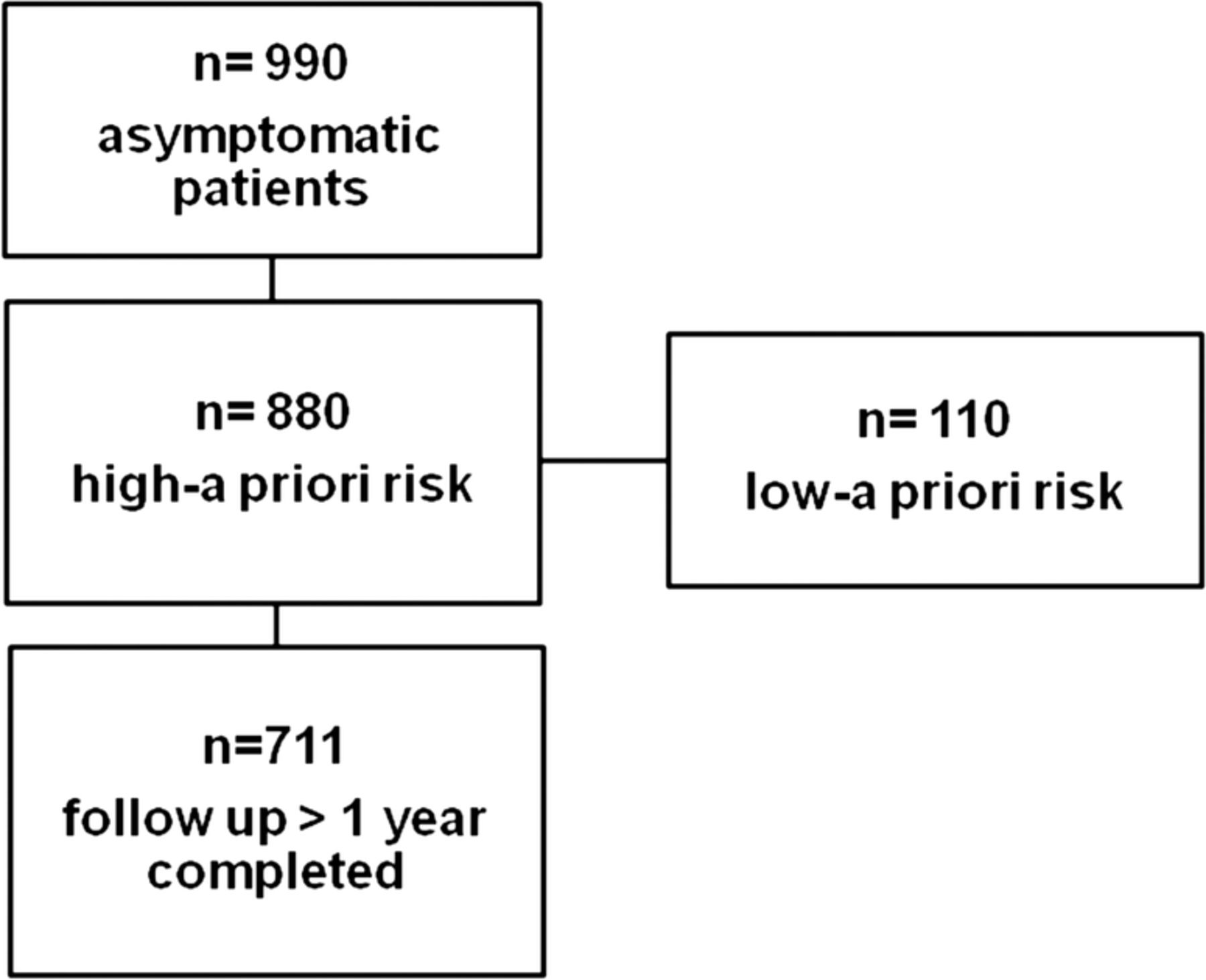
Of 880 asymptomatic patients referred to coronary CT who met the inclusion criteria, 711 (80.8%) could be followed up (F/U) and were finally enrolled (figure 1). F/U period was mean 2.65 years±1.5 (maximum 8 years). Table 1 shows our study cohort characteristics.
Study population (n=711)
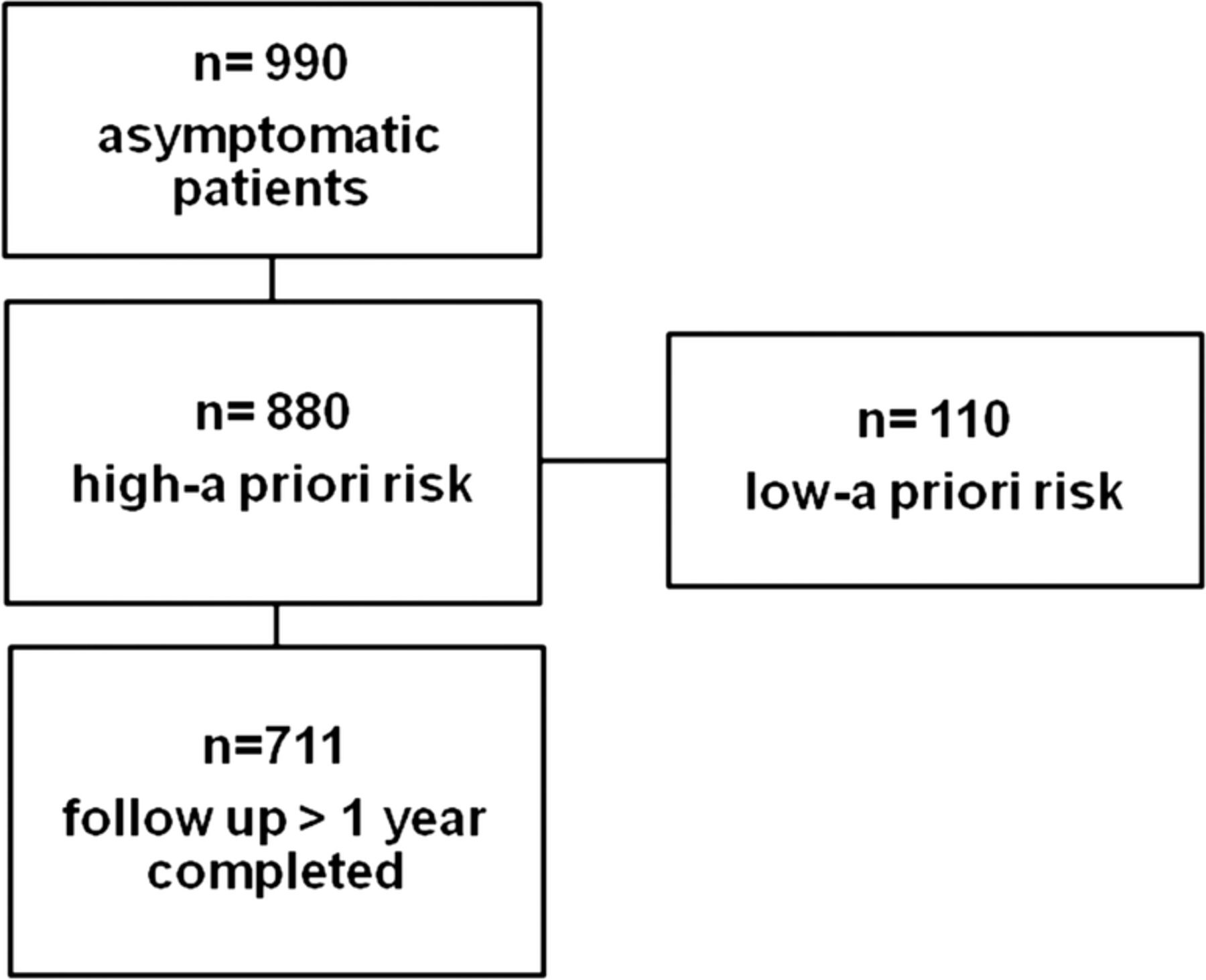
Patient recruitment. Out of all 990 asymptomatic patients referred to coronary CT angiography, those with high ‘a priori’ risk were identified. Out of those, 711 could be followed up for a minimum of 1 year (up to 8 years).
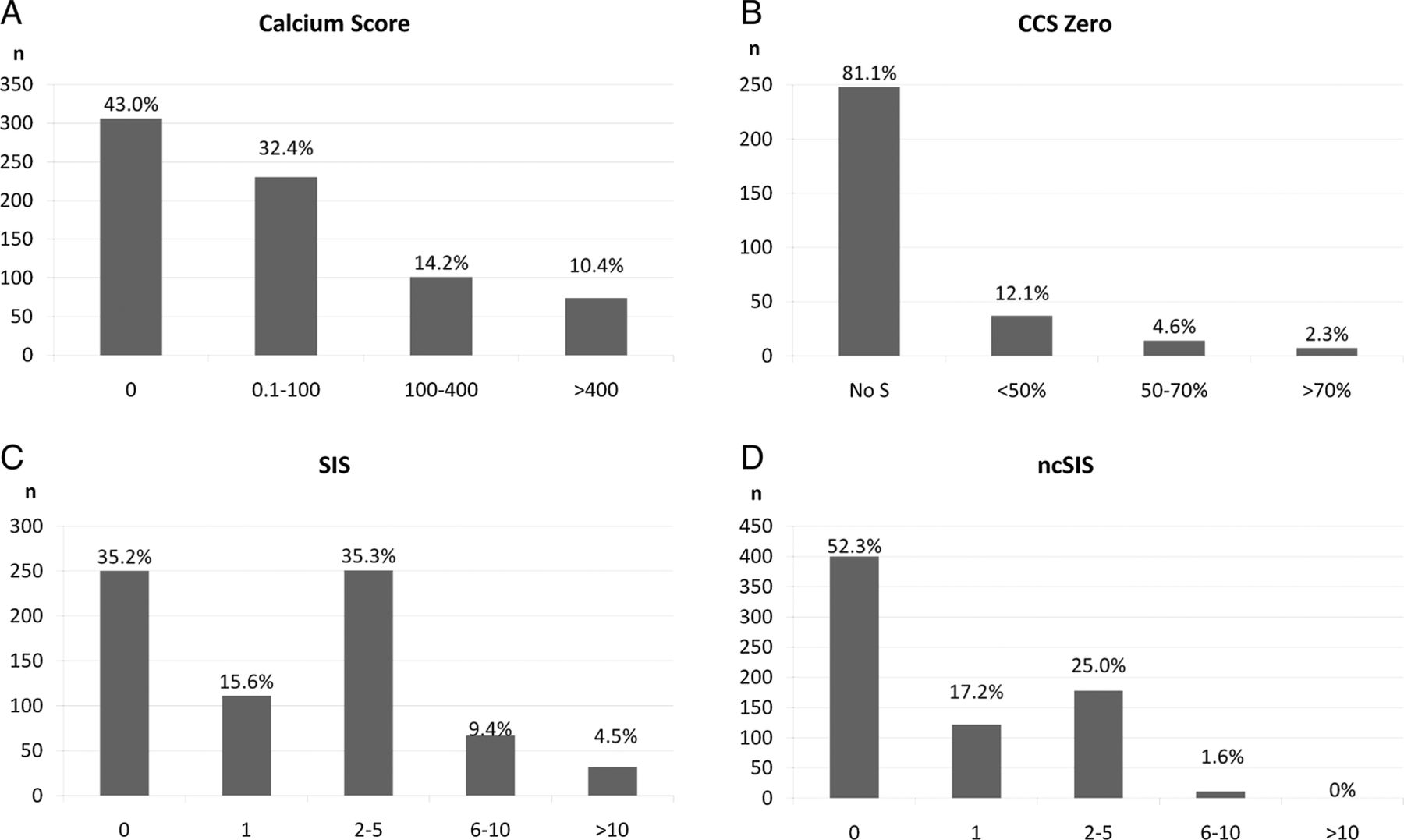
Figure 2 A illustrates CCS severity distribution. CCS zero prevalence was 306 (43%). Out of those, non-calcified plaques were found in 98 (32%; total prevalence of non-calcifying plaques and CCS zero, 7.6%).

CT angiography results (vertical axis, N=count of patients): (A) total Coronary Calcium Score (CCS) (y-axis, Agatston Score), (B) coronary stenosis severity degree (%; y-axis) in CCS zero patients (S=stenosis). (C) coronary artery plaque segment involvement score (SIS) (y-axis) and (D) non-calcified plaque SIS (ncSIS) (y-axis) shows a declining % of patients with increasing scores.
While the majority of CCS zero patients (figure 2B) had no coronary stenosis (81%), 37 (12.1%) had <50%, 14 (4.6%) had intermediate, and 7 (2.3%) had high grade stenosis by CTA.
Overall, 29 (19%) of 153 high-grade stenoses were caused by non-calcified plaques. Non-calcified plaques caused high-grade coronary stenosis in 15/46 (32.6%) patients with low CCS of ≤100 Agatston Units.
The distribution of total and non-calcifying plaque SIS severity stratified in groups is demonstrated in figure 2B, C. Atherosclerotic plaques were calcified (61.7%), mixed (20.4%) or non-calcified (17.9%).
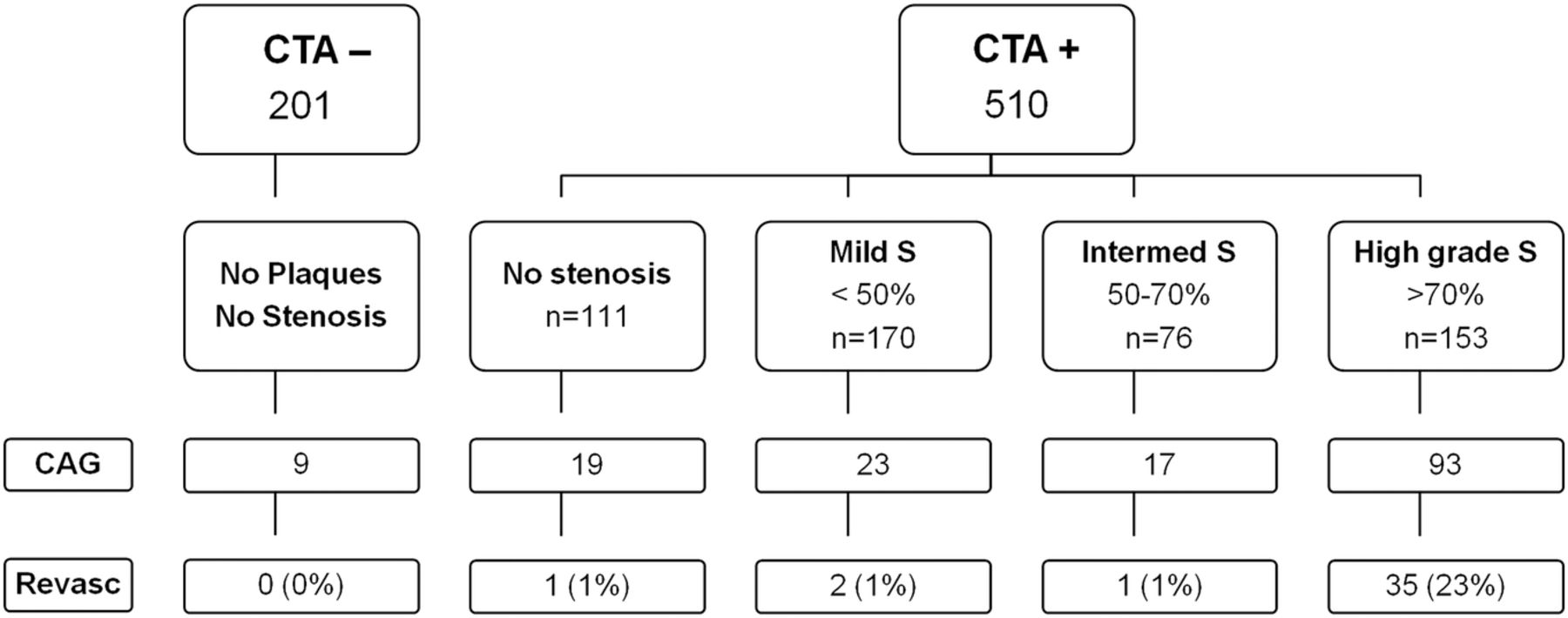
Figure 3 shows CTA findings and the corresponding assignment of patients into stenosis severity groups: 71.7% had signs of CAD+ and 28.3% were CAD− (15.6% plaques without stenosis, 23.9% mild, 10.7% intermediate and 21.5% high-grade stenosis).
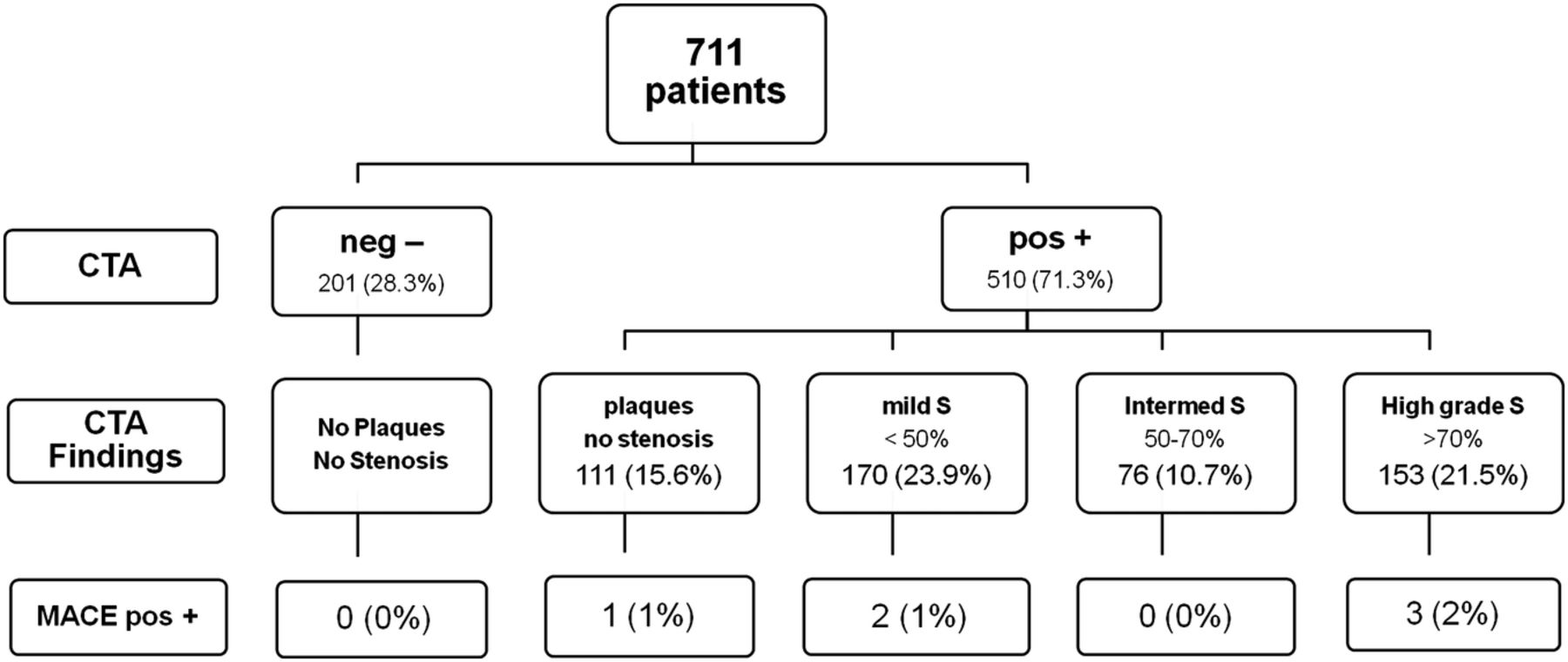
MACE rate among CAD severity groups (total 0.8%; 6/711) based on CTA findings (stenosis severity). MACE occurred only in CAD-positive patients but in none (0%) of CAD negatives by CTA CAD, coronary artery disease; CTA, CT angiography; MACE, major adverse cardiac events; S, stenosis.
Primary end point: MACE
Total MACE rate was 0.8% (6/711, 4 STEMI and 2 NSTEMI; including 2 cardiac deaths after STEMI). Figure 3 shows the MACE rates among the CTA stenosis severity groups. There was no MACE in the negative CTA (0%) group. Of six events in the CAD+ group, three patients had high-grade stenosis, two had intermediate and one had mild stenosis by CTA (four of six patients had non-calcifying plaque).
MACE rate in the CAD+ group was slightly higher (1.2%) than in the CAD− (0%) group (p=0.27; Fisher’s exact test). The Kaplan-Meier curve for MACE (figure 4) illustrates a trend towards superior survival in CAD− patients as compared with CAD+ (p=0.063).

Kaplan–Meier survival curve for major adverse cardiac events (MACE): a trend towards superior survival in patients without signs of coronary artery disease (CAD; 0%) as compared to CAD+ groups; with a close-to-borderline statistical significance level (p=0.063), and declining survival probability with increasing stenosis severity.
Non-cardiac death was observed in five patients with metastatic disease: one pulmonary embolism/carcinoma, one sarcoma, one Merkel-cell-carcinoma and two metastatic adenocarcinoma.
Secondary end points: (1) Coronary revascularisation and (2) IA >50% stenosis
Total coronary revascularisation rate was 5.5% (39/711, 29 PCI and 10 CABG surgery). Figure 5 illustrates the revascularisation rates among the different CTA stenosis severity groups, and figure 6 Kaplan–Meier survival curve.

Coronary revascularisation rate (total 5.5%; 39/711) was 0% in patients with negative CAD findings. CAD, coronary artery disease; CAG, coronary angiography; CTA+, positive for CAD (presence of non-calcified or calcified plaque); CTA–, negative for CAD; Revasc, revascularisation (percutaneous coronary intervention or coronary artery bypass grafting); S, stenosis; Data are presented as n (%).
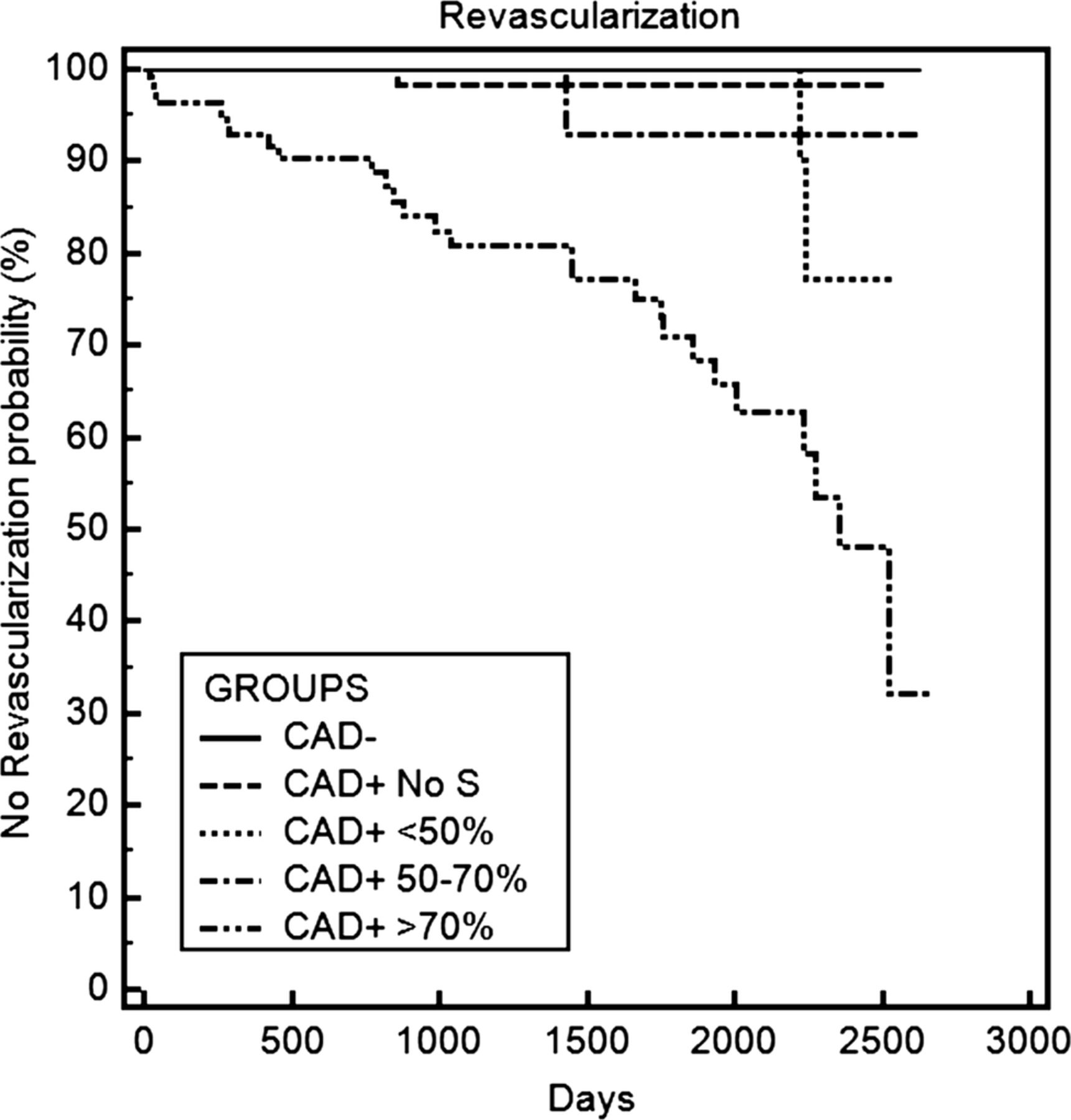
Kaplan-Meier curves: revascularisation rate (PCI or CABG) was significantly higher (p<0.0001) in the CAD+ group (without a statistical difference among stenosis severity groups). CAD+, positive for coronary artery disease; PCI, percutaneous coronary intervention; CABG, coronary artery bypass grafting.
Based on CTA findings and downstream testing, 161 patients (22.6%) were referred to IA. Of those, 93 had high-grade stenosis by CT, the remaining had intermediate or mild stenosis, or IA was performed due to NSTEMI or STEMI.
Compared to IA, the accuracy of CTA for the detection of coronary artery stenosis >50% in 165 patients was: sensitivity 92.5% (95% CI 81.8% to 97.9%). Figure 7 shows an asymptomatic patient with a 99% stenosis by CTA and IA.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Asymptomatic 67-year-old man prior to orthopaedic surgery with three cardiac risk factors and borderline ST-segment depression inferior-posterior on treadmill test, caused by 99% stenosis of the right coronary artery (white arrows, A–C) and concentric non-calcified plaque (inlay right, B) which were correctly identified by CT (A,B) and confirmed by invasive angiography (C).
For exclusion of combined primary and secondary end points, the negative predictive value (NPV) of CTA (>50% stenosis) compared to ICA >50% was 99.3% (95% CI 98.3% to 99.7%) in 711 patients.
CCS had a lower predictive value (c=0.64; 95% CI 0.558 to 0.711) as CTA >50% (c=0.71; 95% CI 0.632 to 0.777; p<0.001) to predict >50% stenosis by CAG (p=0.11).
Atherosclerosis severity scores by CTA for risk prediction
Total coronary atherosclerosis SIS was a significant predictor for MACE if five or more segments were involved (SIS≥5, hazard risk, HR 6.5; table 2) and for secondary end point if SIS≥1.
Cox proportional hazard risk model for primary end point (MACE) and secondary end point (revascularisation rate)
ncSIS≥1 was associated with a significantly increased HR of 2.4 in patients with one or more segments with non-calcified plaques for secondary end point.
Discussion
Our prospective outcome study clearly supports the use of CTA for screening of asymptomatic patients with high ‘a priori’ risk of CAD after conventional cardiological baseline assessment, due to the following findings: First, the prevalence of CAD in our high-risk study cohort was high with 71%, which is markedly higher than in asymptomatic healthy South Koreans9 ,10 with no-risk or low-risk of CAD (22% rate for coronary stenosis of any severity by CTA9 and 11.4% atherosclerosis prevalence by CTA). Beyond ethnic and genetic differences between Asian and Caucasians,24 a higher CAD rate in our study is explained by the higher ‘a priori’ likelihood of CAD in our ‘high-risk’ population, which is characterised by a higher mean age, a higher rate of male gender, higher risk profile, inclusion of patients with diabetes and abnormal previous ECG-treadmill stress test. An underestimation of occult CAD using national cholesterol education programme (NCEP) guidelines as compared to CTA was suggested by Kim et al.10
In our cohort, the majority of patients had mild or intermediate stenosis. All those patients benefit from medical treatment and restrictive coronary risk control management in order to reduce progression of total atherosclerotic plaque burden.25 However, high-grade stenoses were found in one-quarter, and those patients require further diagnostic work-up, potentially including an invasive coronary angiography.
Studies investigating CTA in asymptomatic patients are rare.9–12 Beyond the two South Korean reports, only two other pivotal studies11 ,12 in small cohorts showed, for example, an excellent outcome in 100 patients with normal CTA scans (0% event rate), but a low event rate (8%) in those with non-obstructive CAD.12
Second, our study revealed that zero CCS does not exclude CAD. CCS zero is known for a high NPV for exclusion of CAD and recommended for screening of asymptomatic patients.26 ,27 This finding is in line with Cheng et al28 in which CCS zero failed to rule out CAD and even high-grade stenosis in selected patients due to non-calcifying plaques. Similarly, well over one-third of all plaques were non-calcified in another study.10
Our study supports the use of CTA instead of CCS for screening of asymptomatic patients for CAD by CTA, particularly in those having a high ‘a priori’ risk of CAD, who have a markedly higher prevalence of CAD, in contrast to no-risk or low-risk patients (eg, CCS zero rate was 93% in asymptomatic healthy Koreans).10
The advantage of CTA over CCS was highlighted in a recent data release from the CONFIRM registry, in which symptomatic patients were enrolled, which showed the incremental value of CCTA using plaque burden and stenosis severity score over CCS for discrimination of individuals at risk of death or myocardial infarct.29 Most recently, incremental value data of CTA over CCS were also released from the CONFIRM registry for 27 125 asymptomatic individuals with diabetes,30 with results similar to those found in our population. Beyond age, gender and CCS (C-index 0.64), CCTA improved discrimination by maximal stenosis, number of obstructive vessels and the coronary segment stenosis score (C-index 0.77–78, respectively) in this study.30
Moreover, our data are in line with other studies emphasising no absolute linearity of increasing CCS and total coronary plaque burden. Particularly low CCS was significantly less reliable in predicting total plaque burden due to their association with higher overall prevalence of non-calcified plaques. This has been shown in other studies with a significant stenosis rate of nearly 10%27 and high prevalence of non-calcifying plaques (83.3%) in those with low CCS (≤100).10
Overall, the total rate of non-calcifying plaques and Calcium Score zero in our study cohort was 7.6%, similar to patients with atypical chest pain and an intermediate Framingham risk profile.6 Non-calcifying plaques may cause chest pain, for example, due to endothelial dysfunction, which occurs at early stages of atherosclerosis, due to lack of regular flow-mediated vasodilation or even vasoconstriction at a lesion with mild stenosis.31
Third, our study revealed that the total and non-calcified plaque burdens (SIS and ncSIS) predict adverse outcome in terms of MACE and revascularisation procedures such as PCI or CABG, respectively, which is in line with results from the CONFIRM trial.32 In contrast, the CONFIRM trial mainly enrolled symptomatic patients.
As a study novelty, we calculated a dedicated non-calcifying plaque score (the ‘ncSIS’), which showed an increased risk of adverse outcome for secondary end point, even if only one (or more) segment was involved.
An increasing total coronary plaque burden by CTA was associated with a significantly increased risk of MACE and revascularisation rate, going in line with results from multicentre-registry CONFIRM, in which were identified as risk factors. The total plaque burden, stenosis severity32 or number of proximal segments with mixed or calcified plaques by CTA.33
Finally, our study provides strong evidence that CTA is a highly reliable and accurate tool to exclude significant CAD and MACE events over a midterm follow-up period of mean 2.65 years (up to 8 years). No cardiac events occurred in patients with negative CTA findings.
In summary, our data support screening of asymptomatic high-risk patients with CTA. Compared to CT Calcium Score, most recently introduced low-dose CT techniques such as prospective ECG-gating allow for almost equal or just slightly higher radiation exposure of ≥1 mSv, however, while adding iodine CA.
Compared to CCS, CTA provides the advantage of detecting non-calcifying plaque (representing early stages of atherosclerosis), coronary plaque load assessment and stenosis quantification for risk stratification. Patients with stenosis >50% by CTA yielded a markedly higher risk of adverse outcome than increasing CCS values.
Whether follow-up of high-risk patients by CCTA should be performed is currently an open item for discussion. There are no scientific data on CTA for monitoring of CAD progression. Follow-up intervals of a minimum of 5–7 years may be reasonable for evaluation of CAD progression. In those with intermediate stenosis (50–70%), a myocardial perfusion stress test (eg, SPECT) should be appended in order to define the haemodynamic significance of a coronary lesion.
Study limitations
First, we acknowledge a low total MACE rate. One reason is the short-term follow-up period of 2.65 years, beyond patient population selection criteria with a low rate of diabetes (12.4%).
Second, our inclusion criteria for definition of our cohorts ‘high-risk’ of CAD involved ECG-treadmill stress testing (beyond coronary risk factors). The ECG-treadmill test has a low accuracy for detection of myocardial ischaemia.
Third, the patient’s current medication (aspirin, statins) was not recorded.
Conclusion
In summary, our study recommends the use of CCTA in asymptomatic patients with a high ‘a priori’ risk of CAD in order to detect subclinical atherosclerosis and obstructive CAD. Non-calcified plaques were found in a high amount of asymptomatic patients, even in CCS zero patients. Non-calcified plaques pose a risk for adverse outcome, even if only small numbers of coronary segments are affected.
CTA allows for coronary risk estimation based on increasing total and non-calcifying plaque burden. CTA is a safe, accurate and reliable modality for exclusion of CAD
Given low radiation exposure of CTA below <1 mSv using the newest low-dose prospective ECG-gated CT techniques such as high-pitch mode or iterative reconstruction, which is equivalent to CCS scanning, CTA should be favoured over CCS in asymptomatic patients with a high ‘a priori’ risk of CAD.
References
Footnotes
-
Contributors FP: data acquisition, manuscript drafting. GF: patient selection, manuscript drafting. WD: statistical analysis, manuscript drafting. AK: statistical analysis, manuscript drafting. WJ: manuscript drafting. WMF: manuscript drafting. GF: data acquisition, patient selection, manuscript drafting.
-
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
-
Competing interests None.
-
Ethics approval Local IRB.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No additional data are available.