Article Text

Abstract
Objective Genetic variants that disrupt the function of the PCSK9 (proprotein convertase subtilisin kexin type 9) and APOB (apolipoprotein B)genes result in lower serum low-density lipoprotein cholesterol (LDL-C) levels and subsequently confer protection against coronary heart disease (CHD). The objective of this study was to measure the prevalence and selective advantage of such variants among healthy older individuals without a history of CHD.
Methods We performed targeted sequencing of the PCSK9 and APOB genes in 13 131 healthy individuals without CHD aged 70 years or older enrolled into the ASPirin in Reducing Events in the Elderly trial. We detected variants in the PCSK9 and APOB genes with predicted loss-of-function. We associated variant carrier status with serum LDL-C and total cholesterol (TC) levels at the time of study enrolment, adjusting for statin use.
Results We detected 22 different rare PCSK9/APOB candidate variants with putative lipid-lowering effect, carried by 104 participants (carrier rate 1 in 126). Serum LDL-C and TC concentrations for rare PCSK9/APOB variant carriers were consistently lower than non-carriers. Rare variant carrier status was associated with 19.4 mg/dL (14.6%) lower LDL-C, compared with non-carriers (p≤0.001, adjusted for statin use). Statin prescriptions were less prevalent in rare variant carriers (16%) than non-carriers (35%). The more common PCSK9 R46L variant (rs11591147-T) was associated with 15.5 mg/dL (11.8%) lower LDL-C in heterozygotes, and 25.2 mg/dL (19.2%) lower LDL-C in homozygotes (both p≤0.001).
Conclusions Lipid-lowering genetic variants are carried by healthy older individuals and contribute to CHD-free survival.
Trial registration number NCT01038583.
- lipids
- coronary artery disease
- genetics
- hyperlipidemias
Data availability statement
Data are available from the corresponding author on request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Loss-of-function genetic variants in the PCSK9 (proprotein convertase subtilisin kexin type 9) and APOB (apolipoprotein B) genes result in lower serum low-density lipoprotein cholesterol concentrations and subsequently confer protection against coronary heart disease (CHD).
What does this study add?
Our study measured the prevalence and selective advantage of lipid-lowering genetic variants in a unique population of healthy older individuals aged ≥70 years without a history of CHD events.
How might this impact on clinical practice?
An improved understanding of the role played by protective lipid-lowering variants may help inform future approaches to CHD risk-reduction and lipid management.
Introduction
Genetic variants that lower serum low-density lipoprotein cholesterol (LDL-C) levels have been demonstrated to be protective against coronary heart disease (CHD).1–9 In particular, protection can be conferred by rare loss-of-function (LoF), protein-truncating variants in canonical lipid-metabolism genes, including the apolipoprotein B (APOB)3 and the proprotein convertase subtilisin kexin type 9 (PCSK9)3 10 genes. These protective lipid-lowering genetic variants tend to be rare in the general population. In addition, LDL-C particle size and other lipoprotein-related genotypes have been associated with CHD-free longevity.11
Familial hypobetalipoproteinaemia is caused by heterozygosity for APOB variants that generally result in LDL-C concentrations that are >50% lower than normal, while PCSK9 LoF variants are associated with more modest effects of 15%–40% lower LDL-C.12 Discovery and understanding of rare protective variants in these genes, particularly PCSK9, has informed the successful development of several lipid-lowering therapies.13 However, most cholesterol-lowering variants, to date, have been identified from case-control or population-based studies.1–9 Populations of healthy older individuals without a history of CHD represent an understudied resource for the discovery and understanding of protective lipid-modifying genetic variants.
With this rationale, we sequenced 13 131 healthy older individuals aged ≥70 years without a previous history of diagnosed CHD events, enrolled in the ASPirin in Reducing Events in the Elderly (ASPREE) trial.14 Among this healthy older CHD-free population (average age 75 years), we hypothesised that the prevalence of rare cholesterol-lowering variants in canonical lipid metabolism genes (PCSK9/APOB) would be enriched, and that variant carrier status would be associated with lower serum LDL-C and total cholesterol (TC) levels—subsequently contributing to CHD-free survival.
Methods
Study population
Participants were enrolled in the ASPREE study, a randomised, placebo-controlled trial of daily low-dose aspirin investigating the effect of daily 100 mg aspirin on disability-free survival.15–17 The ASPREE study design,18 19 recruitment20 and baseline characteristics14 have been published previously. Participants had no previous diagnosis of atherosclerotic or atherothrombotic cardiovascular disease events, including myocardial infarction; heart failure; angina; pectoris; stroke or transient ischaemic attack or diagnosis of atrial fibrillation or high blood pressure.21 Diagnosis of dementia or other serious illness likely to cause death within 5 years were also exclusion criteria. Genetic analysis was conducted on 13 131 samples provided by Australian ASPREE participants aged 70 years or older at enrolment.22
DNA sequencing and variant analysis
A targeted sequencing panel was designed containing the PCSK9 and APOB genes.22 Following standard protocols, DNA was extracted and sequenced using the Thermo Fisher Scientific S5TM XL system to average 200× depth, with sequences aligned to the human genome reference 37. We identified candidate cholesterol-lowering variants from sequence data using two methods: (1) prediction of rare candidate LoF, protein-truncating PCSK9 and APOB variants using the Loss-of-Function Transcript Effect Estimator tool, high-confidence filter, a plugin of Ensemble Variant Effect Predictor23 and (2) assessment of candidate variants associated with hypercholesterolaemia or hypobetalipoproteinaemia identified from published functional and population studies3 10 24 (for list of variants meeting the inclusion criteria, see online supplemental materials). We also examined the effect of the more common PCSK9 R46L variant with known lipid-lowering effect (rs11591147-T).25 Rare variants were curated manually by two or more laboratory scientists following the American College of Medical Genetics/Association for Molecular Pathology Standards26 and variant classification was agnostic to lipid effects. A random selection of 10% of rare variants detected were validated using Sanger sequencing with 100% concordance. The minor allele frequency (MAF) of each variant detected in the ASPREE population was compared with the MAF reported in the genome Aggregation Database Non-Finnish European reference population (gnomAD-NFE).23
Supplemental material
Association of variant carrier status with blood lipid levels
We sought to determine whether PCSK9/APOB variant carriers in the ASPREE cohort were associated with lower serum cholesterol levels at the time of enrolment, versus age-matched and gender-matched non-carriers. To do this, we compared serum LDL-C and TC levels between detected variant carriers versus n=9540 age-matched and gender-matched non-carrier ASPREE controls who did not carry any PCSK9 or APOB variants that met our inclusion criteria. Baseline LDL-C and TC levels were measured in routine blood samples provided by ASPREE participants at enrolment, analysed at commercial pathology laboratories. We tested association of variant carrier status with serum LDL-C and TC levels using multivariable linear regression, adjusting for age, gender, diabetes, hypertension, smoking status, alcohol use and body mass index (BMI). We first tested association using raw unadjusted LDL-C and TC levels (not accounting for statin use), then separately using statin-adjusted levels, dividing LDL-C and TC levels by 0.7 and 0.8, respectively for those using statin medication to estimate untreated levels, as done previously.3 We identified statin users based on concomitant medication data collected by ASPREE (Anatomical Therapeutic Chemical (ATC) code=C10, lipid-modifying agents).
Results
Characteristics of the 13 131 sequenced participants are shown in table 1. The median age at enrolment was 75 years, with 54% of participants female; 28% obese and 4% current smokers. Participants had no previous diagnosis of cardiovascular disease or dementia.14 Most participants were of European ancestry (99% self-reported as white/Caucasian). The mean serum LDL-C and TC concentrations of the study population were 119 and 204 mg/dL, respectively at the time of enrolment.
Characteristics of sequenced participants at enrolment
Among this population, we detected a total of 104 healthy older CHD-free individuals carrying rare candidate LoF variants that met our inclusion criteria (MAF <0.01). Variants were found across multiple different domains of the APOB and PCSK9 genes (schematic representation in figure 1). Overall, the carrier rate of detected rare variants in PCSK9/APOB meeting our inclusion criteria (when considered as a group) was 1 in 126 participants or 0.8%.

Schematic representation of the apolipoprotein B (APOB) and proprotein convertase subtilisin kexin type 9 (PCSK9) genes indicating the location of identified variants. We detected 22 different rare protein truncating or missense APOB and PCSK9 variants with putative loss-of-function and lipid-lowering effect. We also investigated the more common PCSK9 R46L variant (rs11591147). Variants were found across different protein domains of the APOB and PCSK9 genes.
We detected a total of 22 different rare APOB/PCSK9 variants, ranging in frequency between MAF=0.00335 (detected in 44 ASPREE participants) and MAF=0.00008 (singletons detected in only one ASPREE participant) (table 2). MAFs of the variants detected in the ASPREE population were found to be consistently higher when compared with MAFs from the gnomAD-NFE reference population (table 2). We found six putatively novel rare APOB variants that, at the time of our analysis, were not found in the gnomAD or dbSNP databases, and were not previously reported in the literature. Each of these rare APOB variants were detected as singletons in the ASPREE cohort (MAF=0.0008) and met our criteria for LoF (table 2).
Prevalence of LDL-C-lowering variants in a population of 13,131 healthy older CHD-free individuals (ASPREE)
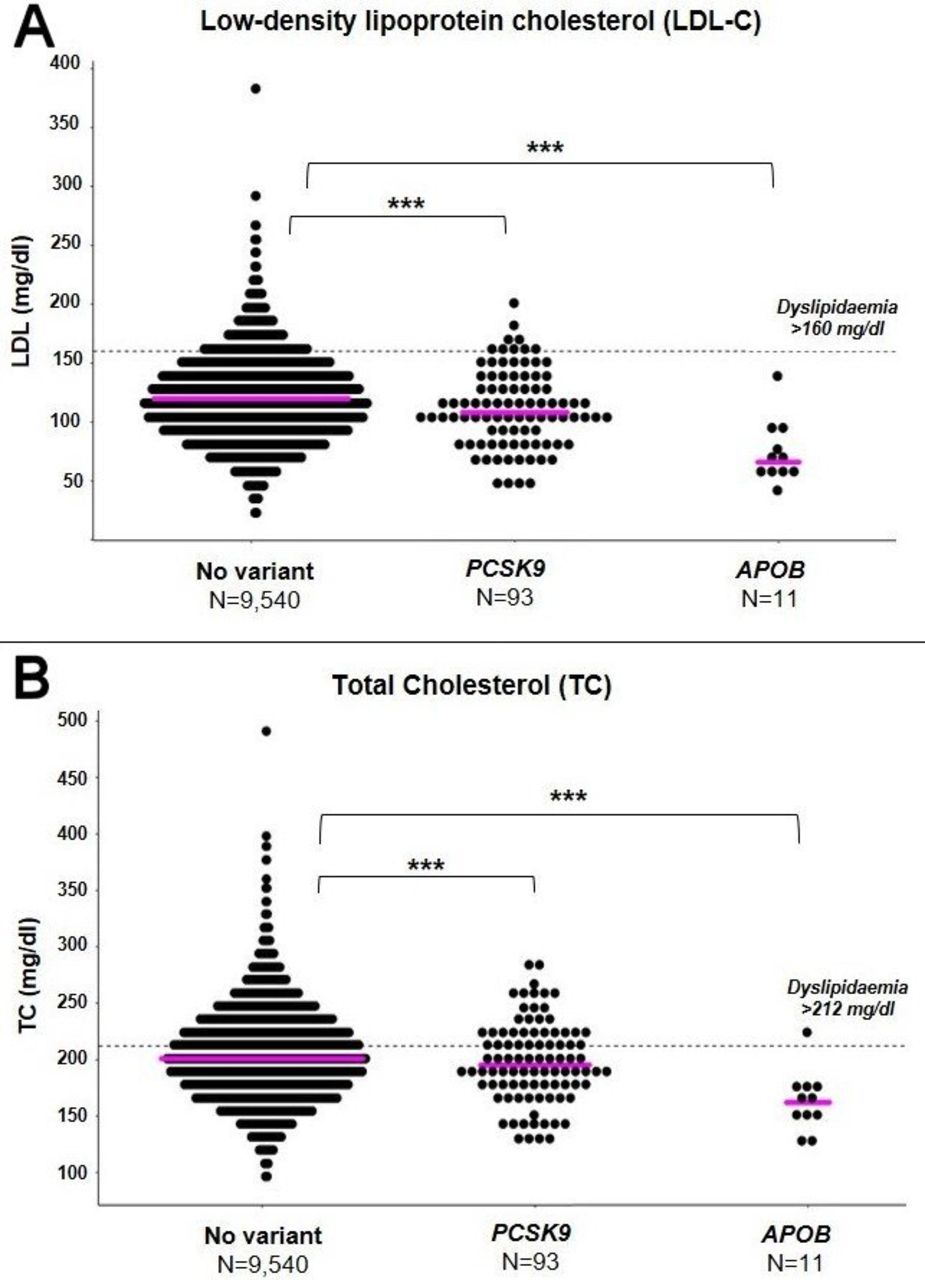
The serum LDL-C and TC concentrations for carriers of rare APOB or PCSK9 variants were found to be consistently lower than the n=9450 non-carrier controls in the study (figure 2, table 2). For some rare variants, the reduction in LDL-C was up to 77.4 mg/dL (eg, APOB c.7300C>T (p.Gln2434Ter)). Based on raw LDL-C and TC levels uncorrected for statin use, rare variant heterozygous carrier status in ASPREE (when considered as a group of n=104 participants) was associated with 11.6 mg/dL (9.7%) lower serum LDL-C (p<0.001) and 7.8 mg/dL (3.9%) lower serum TC (p<0.001) versus non-carriers, adjusted for age, gender, diabetes, hypertension, smoking status, alcohol use and BMI (figure 3, table 3).

Relative changes in serum low-density lipoprotein cholesterol (LDL-C) and total cholesterol (TC) levels per variant detected, in variant carriers versus non-carriers. Shown are waterfall plots of the relative changes in serum LDL-C (A) and TC (B) concentrations at enrolment (mg/dL) for carriers of proprotein convertase subtilisin kexin type 9 (PCSK9) and apolipoprotein B (APOB) variants, compared with the mean concentration from n=9450 non-carrier controls (normalised to 0 mg/dL). Variant name labels are shown vertically above the plots, and include the total number (N) of carriers detected per variant. For variants detected in more than one participant, the mean LDL-C and TC levels for all carriers of that variant are plotted.

{kind=link}
{kind=link}
{kind=link}
Proprotein convertase subtilisin kexin type 9 (PCSK9) and apolipoprotein B (APOB) rare variant carrier status in ASPirin in Reducing Events in the Elderly (ASPREE) is associated with reduced serum low-density lipoprotein cholesterol (LDL-C) and total cholesterol (TC) levels. Shown is a comparison of serum LDL-C (A) and TC (B) levels at enrolment for carriers of rare variants (minor allele frequency (MAF) <0.01) in PCSK9 (n=93) and APOB (n=11), compared with non-carrier controls (n=9540) from the ASPREE study. Results indicate that rare APOB/PCSK9 rare variant carrier status is associated with reduced serum LDL-C and TC levels versus non-carriers. Linear regression was used to compare statistical differences between groups adjusting for covariates. Median values are shown as coloured solid lines (magenta). Statistical significance is denoted as ***p≤0.001. Dyslipidaemia (dotted lines) is defined as serum LDL-C >160 mg/dL, or serum TC >212 mg/dL.14 To convert values from mg/dL to mmol/L multiply by 0.02586.
Variant carrier status is associated with reduced serum LDL-C and TC levels
After adjusting for statin use (dividing LDL-C and TC levels by 0.7 and 0.8, respectively for those taking statin medication), rare variant heterozygous carrier status was associated with 19.4 mg/dL (14.6%) lower adjusted serum LDL-C (p<0.001) and 16.4 mg/dL (7.5%) lower adjusted serum TC (p<0.001) versus non-carriers. The prevalence of lipid-lowering statin prescriptions among rare variant carriers was 16% (n=17/104), which was lower than that observed in non-carriers (35%, n=3324/9540).
The estimated median untreated LDL-C level in non-carriers was 131.5 mg/dL (110.4–154.7), compared with 112.1 mg/dL (92.8–139.2) in rare PCSK9/APOB variant carriers. At the per-gene level, rare variant carrier status for PCSK9 and APOB variants separately was also associated with significantly lower LDL-C levels for both genes (p<0.001).
For the more common PCSK9 R46L variant (rs11591147-T, ASPREE MAF=0.03541), heterozygous and homozygous carrier status were associated with 15.5 mg/dL (11.8%) lower and 25.2 mg/dL (19.2%) lower statin-corrected LDL-C levels, respectively (p≤0.001) (table 3).
Discussion
In this study, we identified rare PCSK9 and APOB variants that are associated with lower serum LDL-C levels among a population of healthy older individuals without a history of CHD events. Most of the variants detected were enriched in frequency among the healthy older CHD-free ASPREE population, compared with a large reference population of similar genetic ancestry (gnomAD-NFE). Serum LDL-C and TC concentrations for rare variant carriers were consistently lower than non-carriers in the study, and rare variant carrier status was associated with 19.4 mg/dL (14.6%) lower serum LDL-C and TC concentrations, after adjusting for statin use. The prevalence of statin prescriptions in variant carriers were less than half that observed in non-carriers. Together, these results indicate that lipid-lowering genetic variants are enriched in healthy older individuals without CHD, and play a role in coronary disease-free survival throughout the human lifespan.
Consistent with other studies,1–9 we observed that LoF variants in the PCSK9 and APOB gene are associated with lower serum LDL-C concentrations. However, to our knowledge, the prevalence shown in ASPREE during ageing free of atherosclerotic cardiovascular disease manifestations has not previously been demonstrated. Variants analysed were found to lower serum LDL-C and TC levels among the ASPREE population, with the difference in LDL-C concentrations between ASPREE rare variant carrier and non-carriers being ~20 mg/dL after adjusting for statin use. At an average participant age of 75 years, this represents the effect of potentially a lifetime of exposure to genetically determined lower LDL-C.
Meta-analysis of statin trials suggests for a 38 mg/dL reduction in LDL-C, there is a 20%–22% reduction in CHD risk, in the setting of relatively short clinical trials.27 Mendelian randomisation studies, however, demonstrate the importance of lifetime exposure to low LDL-C, suggesting that genetically determined low LDL-C is associated with a greater magnitude of CHD risk-reduction, compared with equivalent reduction through statin use.28 It is therefore likely that ASPREE rare variant carriers detected in this study, who have experienced a lifetime of exposure to genetically lower LDL-C, have benefited substantially from lower CHD risk. However, it is noteworthy that the rare variants detected likely account for only a fraction of the reduced CHD risk in the ASPREE population (n=13 131), with a range of other genetic and lifestyle factors contributing.
Strengths of the study include the sample size and unique ascertainment of the ASPREE population. The sequenced cohort comprised 13 131 individuals with an average age of 75 years, with no previous diagnosis of CHD or other cardiovascular events. It is rare for a population ascertained with these characteristics to be made available for genetic analysis. The sequenced cohort was the result of a unique set of circumstances made possible by the strict ASPREE inclusion criteria and age cut-off, and associated research biobank.14 29
Another strength of the study is that ASPREE participants were well characterised, each receiving a medical assessment by a general practitioner at enrolment, to confirm eligibility for the trial, and to rule out previous diagnoses of CHD.14 This provided confidence that detected variant carriers were CHD event-free at enrolment. Other strengths of the study include the depth of sequencing, focus on canonical lipid metabolism genes with established biological effect and stringency of variant curation used, to ensure only high-confidence variants were included in analyses.
Limitations of the study include our results not necessarily being generalisable to populations of non-European ancestry. Furthermore, we caution the comparison of rare variant prevalence between ASPREE and reference populations such as gnomAD, due to the potential for technical artefacts introduced by differences in sequencing technologies and variant curation, and population stratification related to differences in genetic ancestry. These well-known sources of variability are compounded when attempting to compare rare variant frequencies between studies.30 Nonetheless, our results suggest that rare PSCK9/APOB variants are enriched in healthy older CHD-free individuals (table 2), consistent with previous studies showing that LDL-C-lowering variants are associated with reduced risk for CHD and longevity.1–9
Regarding the genes analysed in our study, we focused on only the most established two canonical lipid metabolism genes where rare LoF variants have been demonstrated to have a high effect in reducing LDL-C levels (PCSK9 and APOB).1 3 8 9 We did not examine gain-of-function variants in the LDLR gene, or LoF variants in other genes that have been associated with LDL-C reduction (eg, NPC1L1, LPA, APOC3, ANGPTL3/4 and ASGR1) as these genes were not included on the sequencing panel used. We also could not calculate polygenic scores due to the targeted nature of the sequencing assay, and could not assess subclinical atherosclerosis due to absence of data on coronary artery calcium and carotid intima-media thickness. We did not functionally validate the detected rare variants.
Our study demonstrates the unique contribution of healthy older populations to exploring genetic determinants of health and lifespan. Historically, healthy older populations have not been the focus of large human genetic studies, mainly due to the difficulties in ascertaining large numbers of samples in this age group. However, studies focused on well-characterised populations of healthy older individuals represent an underexplored opportunity for the detection and improved understanding of protective genetic variants, especially in the context of lipid regulation and CHD.29 An improved understanding of the role played by protective lipid-lowering variants may help inform novel future approaches to CHD risk-reduction and lipid management.
Data availability statement
Data are available from the corresponding author on request.
Ethics statements
Ethics approval
The study received approvals from the Alfred Hospital Research Ethics Committee (Project 390/15). All participants provided written informed consent for genetic research.
Acknowledgments
We thank the ASPREE trial staff in Australia and the USA, the ASPREE participants who volunteered for the trial and the general practitioners and staff of the medical clinics who cared for the participants.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors PL, MR, RS, AJH, JP, GP, ES and JJMcN made substantial contributions to conception and design, acquisition of data or analysis and interpretation of data. PL, MR, AJH, JT, AT, CR, SZ, AMM, SN, GW and JJMcN were involved in drafting the manuscript or revising it critically for important intellectual content. All authors gave final approval of the version to be published. PL and JJMcN agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding The ASPREE Healthy Ageing Biobank is supported by a Flagship cluster grant (including the Commonwealth Scientific and Industrial Research Organisation, Monash University, Menzies Research Institute, Australian National University, University of Melbourne); and grants (U01AG029824) from the National Institute on Aging and the National Cancer Institute at the National Institutes of Health, by grants (334047 and 1127060) from the National Health and Medical Research Council of Australia, and by Monash University and the Victorian Cancer Agency. PL is supported by a National Heart Foundation Future Leader Fellowship (102604).
Competing interests GW has received honoraria and/or research grants from Arrowhead, AstraZeneca, Kowa, Regeneron, Sanofi, Amgen and Novartis. SN has received research support and/or honoraria for Amgen, AstraZeneca, Eli Lilly, Esperion, Novartis, Merck, Pfizer, Iowa and Sanofi-Regeneron. RS serves as Vice-President of Technology Development at Sema4. ES serves as Chief Executive Officer at Sema4. No other conflicts were reported.
Provenance and peer review Not commissioned; externally peer reviewed.