Article Text

Abstract
Objectives The aim of this study was to investigate the impact of acute left ventricular unloading by percutaneous left ventricular assist device on pulmonary congestion and pneumonia in patients with cardiogenic shock (CS).
Methods In this retrospective study, we analysed patients with CS who received the Impella percutaneous left ventricular assist device (n=50) compared with those who received intra-aortic balloon pump (IABP) support (n=50). Pulmonary congestion was longitudinally assessed while on support by calculating characteristic findings on the chest X-ray using the Halperin score. The rate of pneumonia and early mortality were assessed as a secondary endpoint.
Results The groups (Impella vs IABP) did not differ in terms of age, Sequential Organ Failure Assessment (SOFA) score, Acute Physiology, Chronic Health Evaluation (APACHE) II score or serum lactate levels. Pulmonary congestion decreased in patient treated with Impella at each time point postimplantation. No change in congestion status was observed in patients supported with IABP. Multivariate analysis indicated Impella support as an independent predictor for pulmonary decongestion (OR 4.06, 95% CI 1.15 to 14.35, p=0.030). The rate of early pneumonia was lower in the Impella group compared with the IABP group (54% vs 74%, p=0.037). Failure of pulmonary decongestion during mechanical circulatory support independently predicted early pneumonia (OR 0.28, 95% CI 0.12 to 0.70, p=0.006).
Conclusion Pulmonary decongestion may facilitate treatment of pneumonia in patients with CS. Left ventricular unloading by Impella device might support pulmonary decongestion, although a larger prospective trial in this patient population is required.
- cardiogenic shock
- left ventricular assist device
- aortic balloon pump
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Treating pneumonia in patients with cardiogenic shock (CS) is challenging because increased left ventricular filling pressure and pulmonary congestion hamper antibiotic approaches. Little is known about the impact of counterpulsation with intra-aortic balloon pump (IABP) or ventricular unloading by mechanical circulatory support (MCS) on pulmonary congestion and on the incidence of pneumonia.
What does this study add?
In this study, we assessed the occurrence and course of pulmonary congestion and pneumonia in a cohort patient with CS supported with Impella pump compared with patients with CS receiving IABP. We report for the first time the course of pulmonary congestion in patients with CS treated with MCS. Successful decongestion was dependent on the type of MCS and was improved in the Impella group. Furthermore, the rate of early pneumonia was lower in patients with pulmonary decongestion.
How might this impact on clinical practice?
Pulmonary decongestion might facilitate treatment of pneumonia. The present study encourages practicing physicians to strive for pulmonary decongestion in patients with CS. The data will help physicians make a more informed decision when choosing the appropriate support device in the clinic to improve the chance of pulmonary decongestion.
Introduction
Cardiogenic shock (CS) is defined by inadequate tissue perfusion due to reduced cardiac output. Despite early revascularisation strategies, the mortality rates of CS remain high at approximately 50%.1 Two out of three patients with CS will develop pulmonary congestion subsequent to left ventricular failure.2 Impaired left ventricular function leads to a back-up of fluid in the lungs and increased pulmonary artery and pulmonary capillary pressure causing pulmonary oedema.
Pneumonia often results from persistent pulmonary congestion and reduced alveolar bacterial clearance.3 Pneumonia progressing to severe sepsis may escalate into respiratory distress syndrome with inherent high mortality. Treating pneumonia in patients with CS is particularly challenging because increased left ventricular filling pressure and pulmonary congestion hamper antibiotic approaches. Refractory pneumonia is common in this patient population.3–5
Counterpulsation therapy with intra-aortic balloon pump (IABP) has been typically used in CS in addition to inotropic drug therapy.6 While a small increase in cardiac output is observed, IABP does not result in a marked decrease of left ventricular filling pressure and would not affect pulmonary congestion.7
Percutaneous ventricular assist devices like the microaxial Impella pump unload the left ventricle and augment cardiac output which maintains blood pressure and improves end-organ perfusion.6 8 9 The benefit of mechanical circulatory support (MCS)-dependent enhanced forward blood flow may extend beyond its impact on cardiac function. Data demonstrate that the use of Impella in patients with myocardial infarct complicated by CS lowers pulmonary capillary wedge pressure.10 This would be expected to decrease pulmonary congestion.
However, to date, no data exist about the impact of counterpulsation with IABP or ventricular unloading by MCS on pulmonary congestion and on the incidence of pneumonia. Therefore, in this study, we assessed the occurrence and course of pulmonary congestion and pneumonia in a cohort of patient with CS supported with Impella pump compared with patients with CS receiving IABP.
Methods
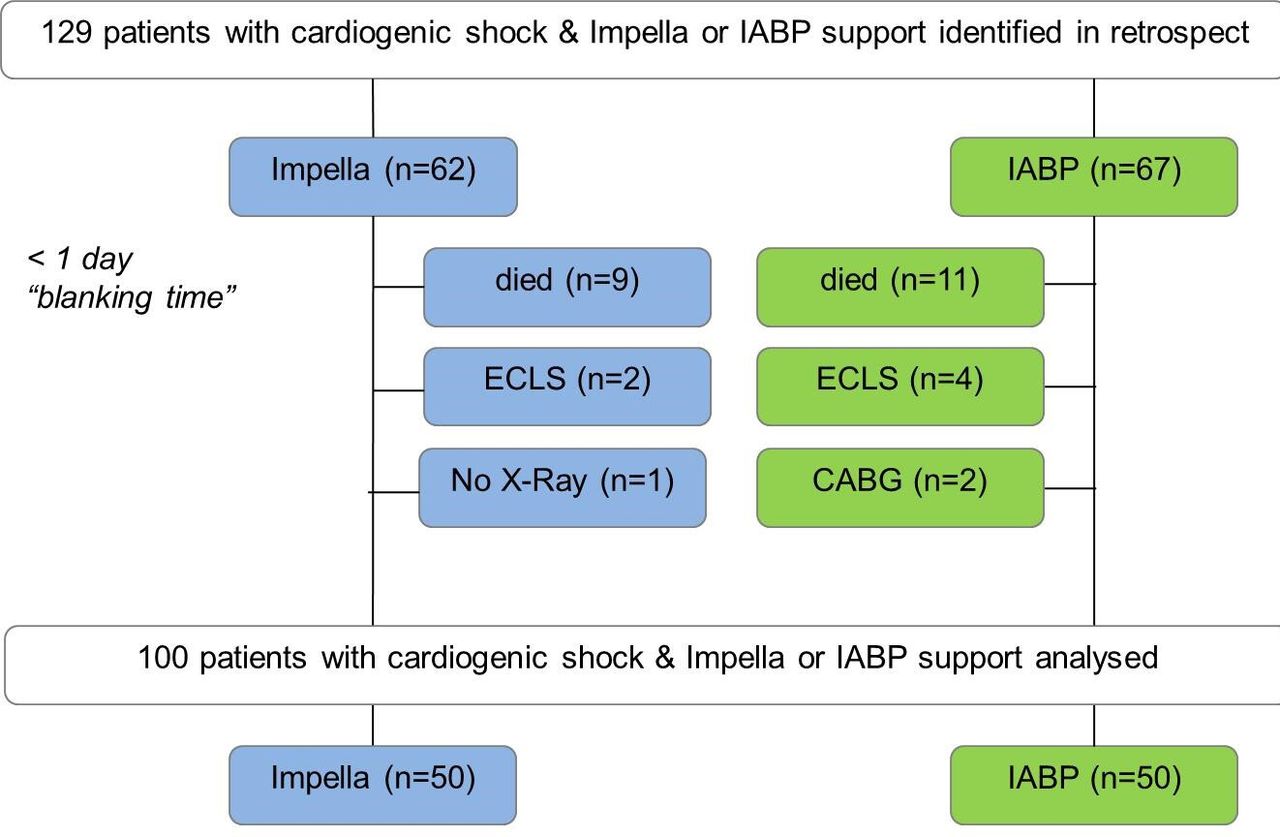
In this retrospective observational study, we assessed pulmonary congestion in patients with CS receiving Impella or an IABP device. Between January 2013 and June 2017, 127 patients with CS were included. The decision for IABP or Impella was left to the discretion of the interventional cardiologist. From 2013 to 2015, the IABP device was the dominant haemodynamic support in our centre. Beginning in 2015, our centre shifted away from IABP in favour of the Impella as a response to the IABP SHOCK trial (figure 1).

Flow chart of study design. IABP, intra-aortic balloon pump; CABG, coronary artery bypass graft; CS, cardiogenic shock; ECLS, extracorporeal life support.
CS was defined as a systolic blood pressure <90 mm Hg or the need for continuous infusion of inotropes or vasopressors to maintain a systolic blood pressure >90 mm Hg with clinical and laboratory evidence of end-organ damage (oliguria, altered mental state, cool extremities).11 We excluded patients who arrived under ongoing resuscitation, those who died immediately on admission or those who were upgraded on extracorporeal life support (ECLS) in the first 48 hours. The duration of mechanical support was individual and was dependent on clinical, haemodynamic and biological parameters. All data were collected from patient charts and medical records until primary discharge including laboratory parameters, complications and therapy strategies. All participants who survived gave written informed consent for the use of their anonymous medical data relating to the defined hospitalisation.
The percutaneous left ventricular assist device (Impella 2.5 or CP; Abiomed, Aachen, Germany) is a microaxial flow pump and is placed percutaneously via femoral artery and crosses the aortic valve into the left ventricle. The system aspirates blood from the left ventricle and expels it into the ascending aorta. The Impella 2.5 and CP deliver up to 2.5 and 3.5 L/min of antegrade flow, respectively.
The IABP (Arrow International, Reading, Pennsylvania, USA) is inserted percutaneously using a femoral approach (7F). The 40 cubic centimetre balloon is positioned in the descending aorta and is rapidly inflated during diastole and deflated during systole. Due to diastolic inflation and displacement of the blood, coronary blood flow and systemic perfusion are improved.6
The primary endpoint of our study was absolute pulmonary congestion. This was assessed by calculating the Halperin score using the characteristic findings of the patient chest X-ray.12 Serial computerised chest X-rays were analysed at baseline (0 hour), 24 hours and 72 hours after implantation of MCS support by a radiologist and two cardiologists who were blinded to the image order. Each lung was divided into three regions and were scored with 0–65 points (0 points=no congestion; 65 points=frank alveolar oedema). The Halperin score is the summation of all six regional scores and ranges from 0 to 390. Severity of pulmonary congestion was further classified by the Halperin score such that 0, normal; 10–60, mild congestion; 61–119, moderate congestion, 120–179, severe congestion; 180–269, interstitial oedema; ≥270, interstitial and alveolar oedema. Marked pulmonary decongestion was defined as a reduction of the Halperin score by a minimum of 60 points (10 points for each region) during the first 72 hours. For each time point, the average of the measurements from the three observers was used for analysis.
The rate of pneumonia was assessed as a secondary endpoint. Pneumonia was defined as a new infiltrate on chest X-ray plus two of three additional criteria: a temperature greater than 38.5°C or less than 36.0°C, and a leucocyte count of more than 10 cells×109/L or less than 3 cells×109/L and new purulent sputum (thick yellow, green, brown or blood-stained mucus).13
Safety endpoints included severe or life-threatening bleeding and moderate bleeding during the hospital stay, as assessed according to the Global Use of Strategies to Open Occluded Coronary Arteries (GUSTO)14 and peripheral ischaemic vascular complications requiring surgical or interventional therapy.
Statistical analysis was performed using SPSS statistics, V.24 (IBM, Armonk, USA). Categorical variables are reported as absolute values and percentages, whereas continuous data are expressed as median with IQR. Categorical data were compared by χ2 test or Fisher’s exact test. Continuous variables were tested for normal distribution with the D'Agostino and Pearson omnibus normality test. In case of a normal distribution, Student’s unpaired t-test was performed to compare the means between the two groups. Continuous variables not following a normal distribution were compared using the Mann-Whitney U test. A one-way repeated measures analysis of variance was used to compare the three time points (0 hour, 24 hours, 72 hours) of the claimed Halperin score and laboratory parameters. Sphericity was checked by performing a Mauchly’s test. Correcting for violations of sphericity was performed by the method of Geisser and Greenhouse.
Univariate and multivariate logistic regression analyses were used to identify clinical predictors for pulmonary decongestion and pneumonia. Candidate variables for the multivariable model were those with a p value<0.1 in the univariate analysis. All tests were two-tailed, and a p value of <0.05 was considered to be statistically significant.
Results
We screened 129 patients receiving MCS for CS at our institution, with 67 patients considered for IABP and 62 patients for Impella support. In the IABP group, 11 patients died during the first 24 hours, 4 patients were upgraded to ECLS and 2 patients were referred to the operating theatre for surgical revascularisation. In the Impella group, nine patients died during the first 24 hours, two patients were upgraded to ECLS and one patient did not get a chest X-ray (figure 1). Taken together, 50 patients in both the Impella and the IABP groups were enrolled into this study. In 27 patients, the Impella 2.5 and in 23 patients the Impella CP was implanted.
In the majority of cases, CS was related to acute myocardial infarction (64% in the Impella group vs 78% in the IABP group, p=0.181) (table 1). In patients with non-myocardial infarction, CS was based on decompensated dilated cardiomyopathy in 11 out of 17 patients (65%) in the Impella group and in 7 out of 11 patients in the IABP group (63%) (p=0.954). The overall resuscitation rate was 54%. Patients in both the Impella and the IABP groups were severely ill, as reflected in the Acute Physiology, Chronic Health Evaluation (APACHE II) score (22 (17; 26) vs 25.5 (18; 29), respectively, p=0.076) and the Sequential Organ Failure Assessment (SOFA) score (9 (7; 11) vs 8.5 (6; 12), p=0.572). There was no major difference in baseline laboratory values or comorbidities between the groups (table 1). Prophylactic antibiotics were given in almost all patients in the study with no difference between the groups (n=42 in the Impella group and n=40 in the IABP group, p=0.603). Further, 40 patients (80%) of the Impella group and 38 patients (76%) of the IABP group were mechanically ventilated during MCS support (table 2).
Baseline characteristics of the study population
Clinical outcomes
During MCS lactate, lactate dehydrogenase, glutamate-oxaloacetate transaminase and glutamate-pyruvate transaminase decreased in both groups (online supplemental tables 1 and 2).
Supplemental material
At baseline, patients in both groups had similarly marked pulmonary congestion as indicated by a Halperin score of 233 (168; 280) points in the Impella group and 200 (164; 250) points in the IABP group (p=0.926). Further, 64% of the patients in the Impella group and 60% of the patients in the IABP group (p=0.680) had pulmonary congestion classified as interstitial oedema or worse using the definition of congestion severity outlined in the Methods section.
Pulmonary congestion continually declined in patients while on Impella support as indicated by the Halperin score (figure 2A) (p=0.001): At 24 hours post-implantation, the Halperin score declined to 180 (138; 236). At the 72 hours time point, further decrease was observed (175 (130; 210) points, t24h vs t72h). On the contrary, in the IABP group pulmonary congestion did not change with time and was 220 (160; 275) points after 24 hours and 205 (154; 250) points after 72 hours (p=0.510) (figure 2B). This distribution of congestion severity also shifted more in the Impella-supported patients. More patients in the Impella group were decongested to a lower classification of congestion using the definition of congestion severity outlined in the Methods section (figure 2C,D). In the Impella group, the percentage of patients with pulmonary congestion classified as interstitial oedema or worse decreased after 72 hours support to 42% (p=0.026). Patients with the presence of alveolar oedema deceased from 26% at baseline to 2% by 72 hours (p=0.001). Additionally, the distribution of patients with mild, moderate or severe congestion increased from 36% at baseline to 58% by 72 hours (p=0.028). This distribution did not change in the IABP group (60% of the patients with pulmonary congestion classified as interstitial oedema or worse pre-support and post-support, p=1.0).
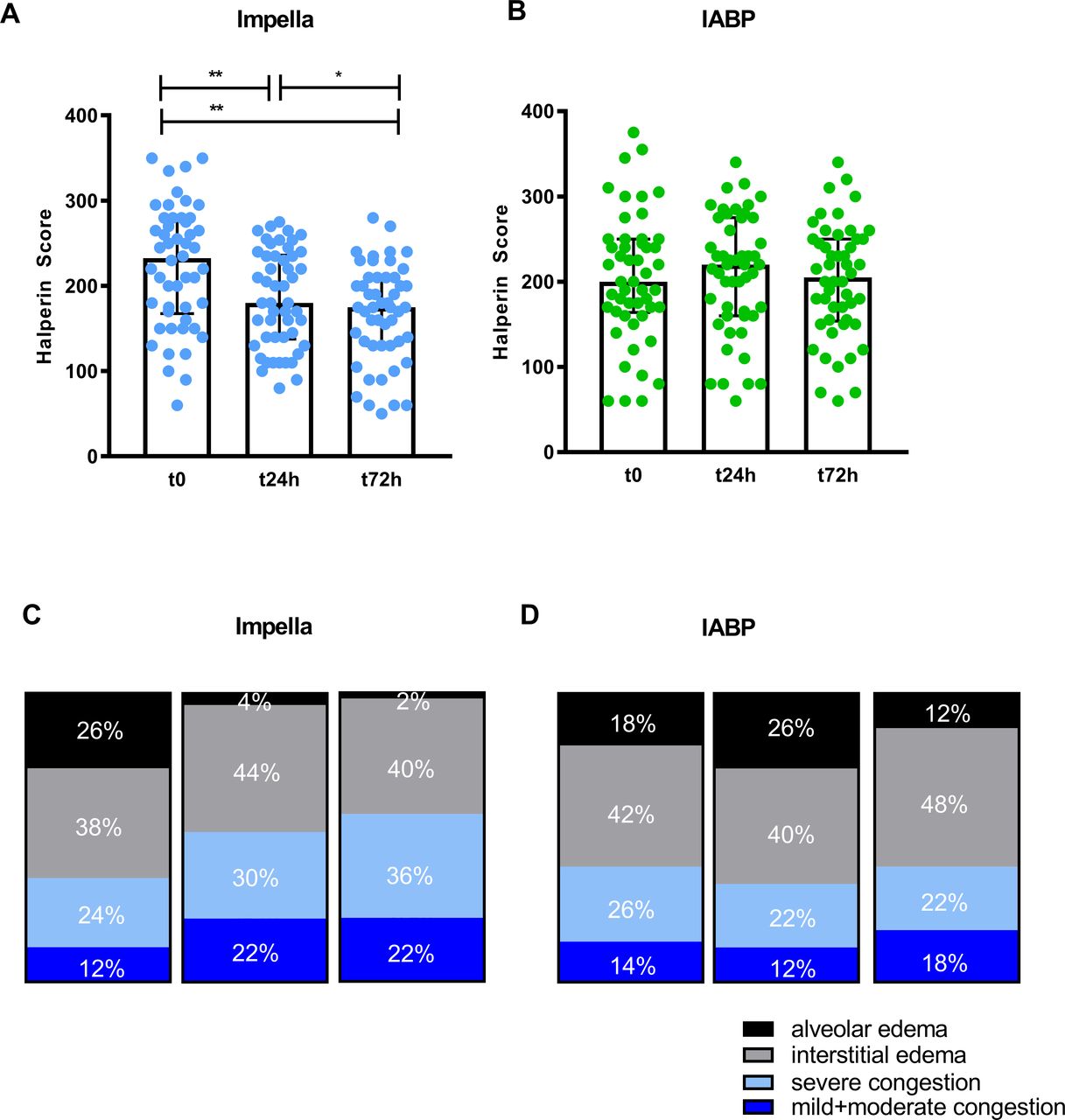
Pulmonary congestion decreased during Impella support but not under intra-aortic balloon pump (IABP) support. (A+B) Scatter plots of Halperin score progression reflecting pulmonary congestion in patients with Impella/IABP support t0 hour, 24 hours and 72 hours after implantation. Continuous data are expressed as median with IQR. (C+D) Severity of pulmonary congestion was further classified by the Halperin score such that 0, normal; 10–119, mild+moderate congestion; 120–179, severe congestion; 180–269, interstitial oedema; 270–329, interstitial and alveolar oedema; ≥330; alveolar oedema. *p≤ 0.05, **p≤ 0.001.
Marked pulmonary decongestion (reduction of more than 60 points of Halperin score) was achieved in 24 patients with Impella support and in 11 patients with IABP support (47% vs 20%, p=0.006).
Halperin score did not differ between mechanically ventilated patients and non-ventilated patients (online supplemental table 3). The ratio of the partial pressure of oxygen in arterial blood/fraction of inspired oxygen (pO2/ FiO2) as a marker of oxygenation disturbance did not differ between the Impella group and the IABP group at each time point (pO2/ FiO2 at t0: p=0.137; pO2/ FiO2 at t24h: p=0.707; pO2/ FiO2 at t72h: p=0.823) (online supplemental tables 1 and 2). In the mechanically ventilated patients, there was also no difference in the positive end-expiratory pressure (PEEP) between the Impella and the IABP groups (PEEP at t0: p=0.067; PEEP at t24h: p=0.064; PEEP at t72h: p=0.248).
The Halperin score did neither correlate with pO2/ FiO2 ratio at the corresponding time points (p=0881 (t0); p=0.141 (t24h); p=0.969 (t72h) nor with the PEEP values (p=0.547 (t0); p=0.174 (t24h); p=0.177 (t72h).
Total fluid balance was net positive in both groups and did not differ between the groups (Impella vs IABP): +0.5 (-0.4; 2.3) L vs +0.9 (0.1; 3.0) L, p=0.702 in the first 24 hours; +0.1 (-0.7; 1.4) L vs +0.1 (-0.6; 0.9) L/24 hours, p=0.98 in the following 48 hours). To identify predictors of pulmonary decongestion, we performed an univariate logistic regression analysis with those parameters supposed to be relevant (online supplemental table 4). In the multivariate analysis, Impella support was an independent predictor for pulmonary decongestion in a model including age and percutaneous coronary intervention (table 3).
Effectors of pulmonary decongestion and pneumonia by multivariate regression analysis
The incidence of early pneumonia during MCS support was lower in the Impella group compared with the IABP group. Early pneumonia developed in 27 patients with Impella support compared with 37 patients with IABP support (54% vs 74%, p=0.037) (figure 3A). Impella support had a number needed to treat of 5 to avoid one case of early pneumonia. Diagnosis of pneumonia was made after 3.2±1.3 days in the Impella group and after 3.1±1.3 days in the IABP group (p=0.6813). The incidence of pneumonia did not differ between mechanically ventilated patients and non-ventilated patients (online supplemental table 3).

{kind=link}
{kind=link}
{kind=link}
Incidence of early pneumonia was lower in patients with Impella support/pulmonary decongestion. (A) Incidence of early pneumonia in patients with Impella support compared with intra-aortic balloon pump (IABP) support. (B) Incidence of early pneumonia in patients with markedly pulmonary decongestion compared patients without decongestion regardless of the type of mechanical circulatory support (MCS). *p≤ 0.05,**p≤ 0.001.
When analysing the full cohort, patients with pulmonary decongestion regardless of the applied MCS device displayed lower incidences of pneumonia: 15 out of 35 patients with pulmonary decongestion developed early pneumonia, whereas 49 out of 65 patients without pulmonary-decongestion developed pneumonia (43% vs 75%, p=0.0012) (figure 3B). To identify predictors of early pneumonia, we performed a univariate logistic regression analysis with those parameters supposed to be relevant (online supplemental table 5). In the multivariate analysis, early pneumonia was independently predicted by failure of pulmonary decongestion during MCS (table 3).
There were no statistically differences between the Impella group and the IABP group regarding rates of moderate or life-threatening bleedings and ischaemic peripheral vascular complications (table 2).
The overall intensive care unit (ICU) length of stay as well as the hospital length of stay did not differ in the Impella group as compared with the IABP group (12 (4; 18) days vs 8 (2;17) days, p=0.293, respectively, 18 (8; 34) days vs 16 (9; 22) days, p=0.149) (table 2). There was also no difference between patients with early pneumonia compared with patients without early pneumonia in overall ICU length of stay as well as the hospital length of stay (8 (3; 17) days vs 12 (2; 19) days, p=0.954, respectively 15 (9; 25) days vs 20 (7; 29) days, p=0.984).
At 30 and at 90 days, there was no difference in all-cause mortality between the Impella and the IABP groups (48.4% vs 47.8%, p=0.943 at 30 days, respectively, 50% vs 53.7%, p=0.672 at 90 days). There was also no difference in mortality between patients with early pneumonia compared with patients without early pneumonia (41% vs 36%, p=0.657, respectively, 50% vs 42%, p=0.423).
Discussion
We report for the first time the course of pulmonary congestion in patients with CS treated with MCS. Successful decongestion was dependent on the type of MCS and was improved in the Impella group. Furthermore, the rate of early pneumonia was lower in patients with pulmonary decongestion compared with patients without decongestion.
In patients with CS, pulmonary congestion is caused by reduced stroke volume, which leads to an increase in pulmonary capillary hydrostatic pressure.15 Clinically, patients in CS with pulmonary oedema, decreased cardiac index and an elevated pulmonary capillary wedge pressure are classified as ‘cold and wet’ by the Forrester classification and exhibit a high in-hospital mortality of approximately 60%.16 17 Our data indicate that patients with CS treated with Impella support displayed significant pulmonary decongestion, while patients treated with IABP did not. Total fluid balance was positive in both groups, thus Impella support might prevent fluid accumulation in the lungs. The decongestion most likely occurs actively by recovery of cardiac function or passively by ventricular unloading both leading to reduced ventricular and concomitant pulmonary capillary hydrostatic filling pressure.
The IABP has been the most common MCS device for years. However, the randomised controlled IABP-SHOCK II trial did not show any beneficial effects of IABP support on short-term or long-term survival in patients with CS.18
This has been suggested to result from the inability of this device to improve patient haemodynamics, particularly cardiac output.6 7 9 19 In contrast, the Impella, a transaortic axial flow pump, provides superior haemodynamic support compared with IABP.6 7 9 19 This is achieved by directly unloading the left ventricular and augmenting cardiac output and mean arterial pressure which improves end-organ perfusion.6 8 9 Directly unloading the left ventricle decreases ventricular wall stress, external work and myocardial oxygen consumption while enhancing myocardial recovery.6 7
Our study did not capture complete haemodynamic data in this patient population. As these were CS patients in need of emergent treatment, the Swan-Ganz catheter capable of capturing pulmonary capillary wedge pressure was not deployed. However, it is known that the pulmonary capillary wedge pressure decreases in patients on Impella support while IABP does not.7 20 Indeed, in a pig model of subacute heart failure, Ishikawa et al directly measured left atrial unloading while on Impella support.21 Unloading of left atrial pressure haemodynamically favours forward flow through the pulmonary circulation, thereby promoting decongestion. We believe this is the best explanation for the difference we observed here in pulmonary decongestion comparing Impella-treated and IABP-treated patients with CS.
Pappalardo et al demonstrated that the addition of Impella in patients with ECLS was associated with reduced left ventricular pressure, thus preventing worsening of pulmonary oedema.22 In six patients treated with a combination of ECLS and Impella-CP support, increased total blood flow and a reduction of pulmonary capillary wedge pressure resulted in a reduced right ventricular afterload and in improved gas exchange.23
Limited data exist on the incidence of pneumonia in patients with CS. Previous studies have demonstrated that pneumonia is partly responsible for the acute worsening of pre-existing cardiac comorbidities.24 25 Data have shown that pneumonia can lead to new cardiac events like acute coronary syndrome and reduced myocardial function due to increased coronary and systemic inflammation as well as vasoconstriction, endothelial dysfunction and increased metabolic demand.24 25 In this context, the development of pneumonia and sepsis adds to the high risk of mortality in patients with CS. Thus, optimal management of these complications may translate into improved survival.
This study shows that the rate of successful pulmonary decongestion was significantly higher in patients treated with the Impella compared with those treated with IABP. Successful pulmonary decongestion could prevent the incidence of early pneumonia.
It is important to emphasise that the present study focused on the development of early pneumonia, which occurred during the first days of MCS support. We chose this as an endpoint because this type of pneumonia is associated with pulmonary oedema. As pulmonary congestion can be mitigated by the left ventricular unloading, this made of a more ideal target for investigation. We also hypothesised that the above described effective decompression of the left ventricle, left atrium and the resulting pulmonary decongestion in patients on Impella support might promote alveolar bacterial clearance and, consequently, leads to less early pneumonia.
While we observed a numerical trend in 90-day survival of patients with Impella support, our study was not powered to detect a mortality difference. It remains unclear whether early pulmonary decongestion by MCS and lower risk of pneumonia affects survival in patients with CS. In a retrospective analysis of patients with myocardial infarction-related CS, the use of an Impella device was not associated with lower 30-day mortality compared with matched patients from the IABP-SHOCK II trial treated with an IABP or medical therapy.26 The prospective randomised DanGer shock trial is ongoing and compares the outcome of patients with myocardial infarction-related CS treated by Impella versus medical therapy.27
Our study is limited by the retrospective study design and the inherent limitations of such an approach. Our study did not capture complete haemodynamic data in this patient population, which could underline the mechanism of the observed effects.
In conclusion, in this retrospective observational analysis, pulmonary decongestion may facilitate treatment of pneumonia in patients with CS. Left ventricular unloading by Impella device might support pulmonary decongestion, although a larger prospective trial in this patient population is required to decipher the potential prognostic value of MCS-induced decongestion on the development of pneumonia.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors SH: data curation, validation, formal analysis, investigation, writing—original draft. AU: data curation, validation, investigation. JH: data curation, validation, investigation. CJ: data curation, validation, investigation. MK: supervision; writing—review and editing. RW: supervision, writing—review and editing. PH: formal analysis, conceptualisation; project administration; writing—original draft, writing—review and editing. Conception and design: SH, PH, RW, MK. Data collection: SH, AU, JH, CJ, RW, PH. Data analysis and interpretation: SH, AU, PH. Drafting of the article: SH, MK, PH. Critical revision and final approval: all authors.
Funding This investigator-initiated work was supported by an unrestricted research grant from Abiomed Europe GmbH, Aachen, Germany, to PH and RW (04.16).
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.