Article Text

Abstract
Objective The purpose of the study was to investigate the excess risk of acute myocardial infarction (AMI) and death from coronary artery disease (coronary heart disease, CHD) in relation to age, level of glycaemic control and renal complications in patients with type 2 diabetes.
Methods A total of 431 579 patients with type 2 diabetes mellitus registered in the Swedish National Diabetes Register from 1 January 1998 to 31 December 2012, and 2 173 620 controls from the general population were included. Cox regression was used to study the excess risk of AMI and CHD.
Results During follow-up of 5.1 years in the diabetes group and 5.4 years in the control group, 36 124 (8.4%) and 115 712 (5.3%) CHD events were registered, with corresponding incidence rates/1000 person-years of 14.64 (95% CI 14.49 to 14.79) and 8.73 (95% CI 8.68 to 8.78), respectively. The HR after adjustment for sex and age was 1.67 (1.65–1.69) which was reduced to 1.42 (1.41–1.44) with further adjustment for level of education, country of birth, diabetes duration and comorbidities. The multivariable-adjusted HR for AMI and CHD death with a time-updated glycated haemoglobin level of 6.9% or lower (≤52 mmol/mol) together with normoalbuminuria and estimated glomerular filtration rate ≥60 mL/min for patients with diabetes compared with controls was 0.95 (95% CI 0.92 to 0.98, p<0.001).
Conclusions In this study, the excess risk of AMI and CHD death was higher for patients with type 2 diabetes compared with controls but converged to that in the general population in patients with on-target HbA1c levels and without renal complications.
- diabetes mellitus
- myocardial infarction
- coronary artery disease
- cardiovascular disease
- renal complications
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- diabetes mellitus
- myocardial infarction
- coronary artery disease
- cardiovascular disease
- renal complications
Key questions
What is already known about this subject?
Cardiovascular disease is the principal cause of death and disability among patients with type 2 diabetes mellitus.
What does this study add?
In this population-based study, it was observed that the excess risk for major coronary events was higher in patients with type 2 diabetes compared with controls but converged to that in the general population in those with time-updated on-target HbA1c levels and without renal complications.
Furthermore, the excess risk of major coronary events at any age was higher for women with type 2 diabetes compared with men.
How might this impact on clinical practice?
Earlier detection of diabetic nephropathy and optimal glycaemic control are required as an effective strategy in preventing major coronary events.
Introduction
The number of adults with diabetes in the world increased from 108 million in 1980 to 422 million in 2014.1 Diabetes mellitus is a major cause of illness and premature death in most countries.2 Cardiovascular disease (CVD) is the major contributor to excess risk of death in patients with diabetes3 and responsible for more than 65% of deaths.4
In particular, diabetes is associated with increased risk of coronary heart disease (CHD).5 A meta-analysis of 102 prospective studies5 including individual data from nearly 700 000 persons (baseline years: 1960–2007) showed that diabetes confers about a twofold excess risk for CHD and similar HRs for coronary events6 compared with a large population-based prospective study conducted on 500 000 participants (baseline years: 2006–2010). Additionally, diabetes was more strongly related to fatal than non-fatal myocardial infarction. HRs for CHD were higher for women than men and in younger than older individuals. Among those with known diabetes at baseline, poor glycaemic control, measured by fasting blood glucose, was associated with higher risk. However, the data underlying from this meta-analysis are now relatively outdated and may not accurately reflect diabetes outcomes in a more contemporary setting. Recent data7 conducted in type 1 and type 2 diabetes individuals from the Swedish National Diabetes Register (NDR) show that mortality and the incidence of cardiovascular outcomes declined substantially among patients with diabetes. Accordingly, more recent data are needed to analyse these issues.
Previous studies5 8 have shown that type 2 diabetes confers a stronger excess risk of CVDs in women than men, with women having 27% and 44% higher relative risks of stroke and CHD, respectively, compared with men. The mechanisms underpinning these sex differences are not fully understood. Suggested explanations include a higher risk-factor burden, more extensive coronary artery disease, as well as hormonal imbalances, suboptimal treatment targets and silent ischaemia.9
Although excess risk for coronary events in patients with type 2 diabetes has been shown to vary with age,10 sex5 8 and glycaemic control,11 few have been adequately powered to the overall risk for acute myocardial infarction (AMI) or CHD death in patients with type 2 diabetes in relation to glycaemic control and renal complications. In this study, we investigated the contemporary excess risk of CHD associated with type 2 diabetes in a nationwide registry of adults with diabetes.
Participants and methods
To access population-based data on patients with type 2 diabetes we used the Swedish NDR. The NDR has been described previously.12 Type 2 diabetes was defined as treatment with diet with or without oral glucose-lowering agents, or insulin with or without oral glucose-lowering agents. The latter category only applied to patients ≥40 years at diabetes diagnosis.
Patients with at least one entry in the NDR from 1 January 1998 to 31 December 2012 were included. For 433 618 (91.5%) patients with type 2 diabetes, five age, sex and county-matched controls were randomly selected from the general population in Sweden.13 Because of the large number of controls required, only four matched controls were available for 22 012 (4.6%) patients with type 2 diabetes, three controls for 2124 (0.5%), two controls for 368 (0.1%) and one control for 302 (0.1%). For 15 622 (3.3%) patients with type 2 diabetes no matched controls were available.
Information on comorbidities and cause-specific mortality for cases and controls was retrieved by linkage to the Swedish Patient Register and Cause of Death Register. Education and country of birth were retrieved from the Longitudinal Integration Database for Health Insurance and Labour Market studies.14 Education was categorised as low (compulsory only), intermediate and high (university or similar). Country of birth was categorised as Sweden or other. The currently used cohort has also been linked with the Swedish Prescribed Drug Register which included information from the entire Swedish Population after July 2005 .15
Patients and controls were followed from baseline until death or 31 December 2013. In total, 42 211 (8.9%) patients with type 2 diabetes and 90 034 (4.0%) matched controls had experienced AMI before index date and, therefore, were excluded. Further, 12 patients and 138 controls were excluded due to inconsistent vital status data, leaving 431 579 (91%) patients with type 2 diabetes and 2173 620 (96%) controls in the analyses.
Outcomes
Primary outcome during follow-up was major coronary events (AMI and death from CHD). The Inpatient Register provides nationwide coverage of all inpatient admissions from 1987 onwards. International Classification of Diseases (ICD) codes were retrieved for AMI, CHD, hospitalisation for heart failure, atrial fibrillation, stroke, cancer diagnoses, renal dialysis and transplantation after 1987. Dates and diagnoses for death from cardiovascular, cancer, diabetes, external and all other causes were retrieved from the cause of death register. For ICD codes, see the online supplementary appendix.
Supplemental material
AMI and CHD death rates were assessed across categories of updated mean glycosylated haemoglobin (HbA1c) levels 16 to compare rates of coronary events in patients and matched controls according to glycaemic control. HbA1c analyses were performed according to the International Federation of Clinical Chemistry standard measured in mmol/mol and converted to levels according to the National Glycohemoglobin Standardization Program for dual reporting.17
Analysis of AMI and CHD death were also performed for two renal variables: (1) normoalbuminuria, microalbuminuria, macroalbuminuria and stage 5 chronic kidney disease (CKD), and (2) estimated glomerular filtration rate (eGFR) 15 to <30, 30 to <60, 60 to <90 and ≥90 mL/min and stage 5 CKD. Stage 5 CKD was defined as need for dialysis or eGFR <15 mL/min.
Microalbuminuria was defined as two positive tests from three samples taken within 1 year, with an albumin/creatinine ratio of 3–30 mg/mmol (30–300 mg/g) or U-albumin of 20–200 µg/min (20–300 mg/L). Macroalbuminuria was defined as albumin/creatinine ratio >30 mg/mmol and eGFR was calculated using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI)18
Systolic blood pressure (SBP) was the mean value of two supine readings with a cuff of appropriate size and after at least 5 min of rest. Low-density lipoprotein (LDL), high-density lipoprotein (HDL) and total cholesterol were measured in mmol/L.
Statistical analysis
Crude event rates are given as events per 1000 patient-years, with 95% CIs and unadjusted incidence rate ratios between patients with type 2 diabetes versus controls estimated by exact Poisson regression. Survival analyses were performed using Cox regression adjusted for sex and time-updated (value recorded closest to the time preceding each event) age in model 1, additionally including time-updated diabetes duration (assuming 0 year for controls and 1 year corresponding to 10th percentile, 4 years to 25th percentile, 8 years to 50th percentile, 13 years to 75th percentile and 19 years to 90th percentile in the distribution of time-updated diabetes duration; 8 years of diabetes duration was interpreted as main analysis) as the continuous covariate in model 2, and further adjusted for education level, country of birth and comorbidities prior to baseline (CHD, atrial fibrillation, heart failure, stroke, valve disease and cancer) in model 3. Model 3 (main model) and, respectively, model 3a for males and model 3b for females were also used to evaluate the association between different outcomes and time-updated HbA1c categories, time-updated albuminuria categories and time-updated eGFR categories in patients with type 2 diabetes versus controls. The effect per 10 mmol/mol higher updated mean HbA1c and time-updated HbA1c categories on events in diabetes population was evaluated separately for men and women, performing model 1-3 as per above, and further adjusting for 3A) time-updated mean SBP, time-updated mean BMI, time-updated smoking and time-updated status on blood pressure lowering medication, 3B) time-updated mean HDL, time-updated mean LDL, time-updated status on lipid lowering medication, 3C) time-updated insulin method, 3D) time-updated albuminuria categories. Interactions for diabetes with sex and prespecified years (<2005 and ≥2005) were also investigated. In these analyses, the time-updated baseline comorbidities prior to 2005 were included in adjustments. Analyses of AMI and CHD death by renal disease status were performed using methods similar to those for time-updated mean HbA1c. The proportional hazards assumption was fulfilled. Post-hoc analysis studying baseline HbA1c instead of time-updated mean HbA1c was performed, and analysis of AMI events alone excluding death due to CHD events.
All tests were two tailed and conducted at the 0.05 significance level. All analyses were performed using SAS software V.9.4 (SAS Institute).
Results
Baseline characteristics of population
Among 431 579 patients with type 2 diabetes and 2 173 620 controls, the proportion of women and the distribution according to age were similar. However, fewer patients with diabetes compared with controls were born in Sweden and had a university education or higher. Baseline characteristics of the two groups are shown in table 1. All coexisting cardiovascular conditions were more common among patients with diabetes than controls. The mean HbA1c at baseline in the diabetes group was 7.1% (54.4 mmol/mol), mean diabetes duration was 5.5 years, mean blood pressure was 140/79 mm Hg, mean low-density lipoprotein was 3.0 mmol/L and 84.4% were non-smokers.
Baseline characteristics of patients with type 2 diabetes and matched controls from the general population
Rates of coronary events in individuals with type 2 diabetes versus controls
The unadjusted rates of major coronary events stratified according to baseline age and sex are shown in table 2. Overall coronary event rates per 1000 person-years were 14.6 among persons with type 2 diabetes (36 124 of 431 579 patients, 8.4%) and 8.7 among controls (115 172 of 2 173 620 patients, 5.3%). In men with type 2 diabetes, coronary event rates were 16.12 (95% CI 15.90 to 16.34) per 1000 person-years (21 343 of 234 556 patients, 9.1%) as compared with 10.03 (95% CI 9.96 to 10.10) among controls (71 180 of 1 170 663 patients, 6.1%). Coronary event rates in women with type 2 diabetes were 12.93 (95% CI 12.72 to 13.14) per 1000 person-years (14 781 of 197 023 patients, 7.5%) as compared with 7.22 (95% CI 7.15 to 7.29) among controls (43 992 of 1 002 957 patients, 4.4 %).
AMI or CHD death per 1000 patient-years by sex and age categories at baseline with 95% CIs estimated by exact Poisson confidence limits
Relative risk for coronary events in the type 2 diabetes population versus controls
In Cox regression analyses, the HR for AMI and death from CHD among persons with type 2 diabetes versus controls was 1.67 (95% CI 1.65 to 1.69) with adjustment for sex and time-updated age, 1.57 (95% CI 1.55 to 1.59) with adjustment for 8 years’ diabetes duration and 1.42 (95% CI 1.41 to 1.44) with additional adjustment for country of birth, education level, diabetes duration and comorbidities at baseline (model 3).
When evaluating AMI (without taking CHD death into account) and adjusting for time-updated age and sex the HR for persons with type 2 diabetes compared with controls was 1.82 (95% CI 1.79 to 1.85), and when additionally adjusting for diabetes duration and obtaining the HR at 8 years of duration it was 1.71 (95% CI 1.68 to 1.74), and when additionally adjusting for country of birth, education level, and comorbidities at baseline (model 3) it was 1.58 (95% CI, 1.56 to 1.61).
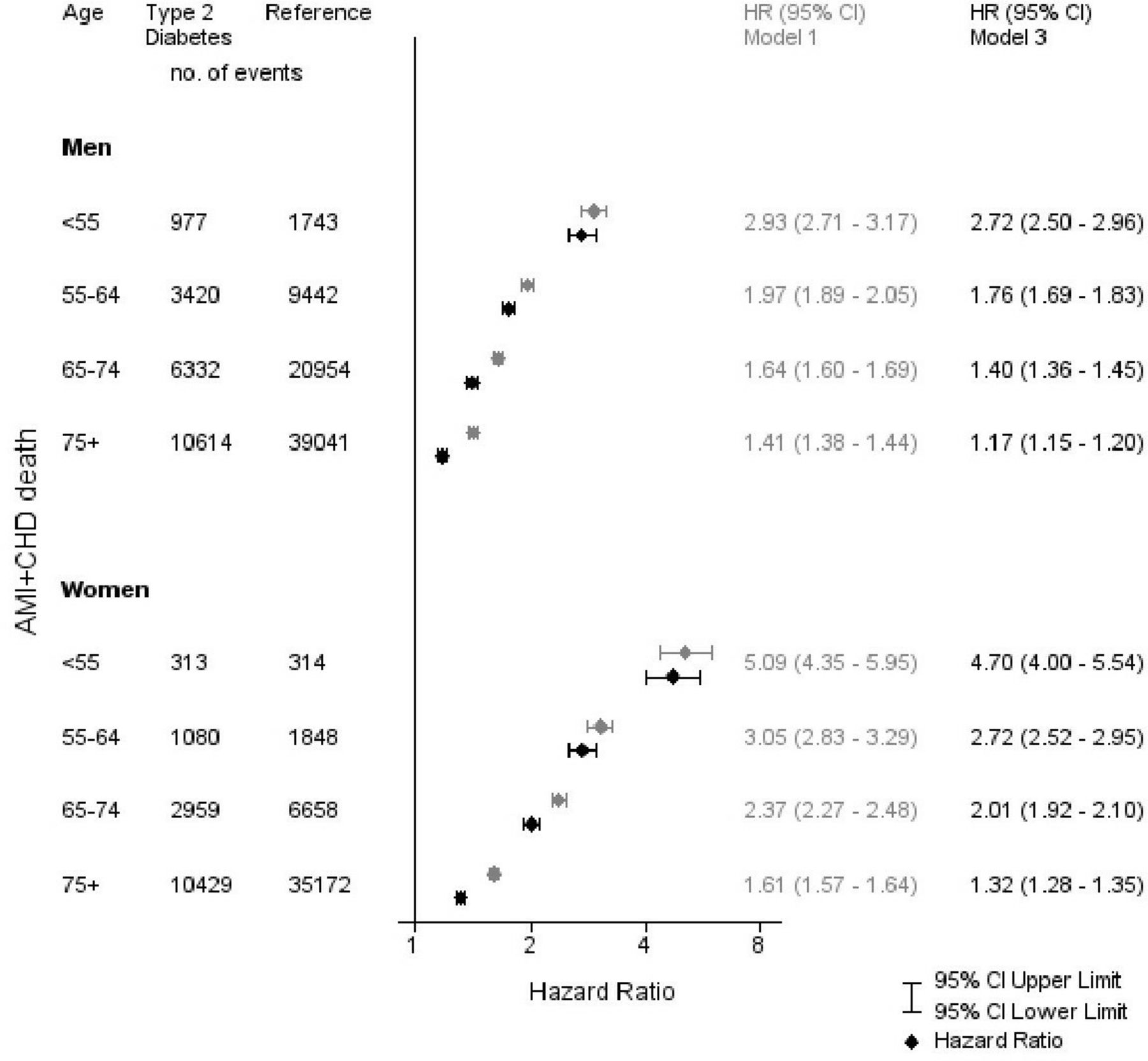
HRs for coronary events decreased with older age and were lower for men compared with women in all age groups (figure 1). In the fully adjusted model 3, the HR decreased monotonically from 2.72 (95% CI 2.50 to 2.96) among men aged <55 years to 1.17 (95% CI 1.15 to 1.20) for men aged ≥75 years. The corresponding HRs for women were 4.70 (95% CI 4.00 to 5.54) and 1.32 (95% CI 1.28 to 1.35), respectively.

{kind=link}
Adjusted HRs for acute myocardial infarction (AMI) and coronary heart disease (CHD) death, according to age category in men and women, in models 1 and 3.
There was also a time interaction in which the adjusted HR for coronary events in patients with diabetes was lower during the last follow-up period (2005 or later) than during the initial 7 years of follow-up (HR in the initial 7 years: 1.57 (95% CI 1.52 to 1.62); HR in the last 8 years’ follow-up: 1.39 (95% CI 1.37 to 1.41), p<0.001 for interaction).
Risk for coronary events related to glycaemic control and renal complications in the type 2 diabetes population compared with controls
The adjusted HRs for AMI and death from CHD for time-updated mean HbA1c categories, albuminuria and eGFR are shown in tables 3 and 4. HRs for coronary events in the fully adjusted model among persons with type 2 diabetes were 1.19 (95% CI 1.17 to 1.21, p<0.001) and 2.77 (95% CI 2.62 to 2.93, p<0.001) with time-updated mean HbA1C ≤6.9% (52 mmol/mol) and HbA1C levels ≥9.7%(≥83 mmol/mol), respectively, as compared with controls. When HbA1C was not time-updated (at baseline), the corresponding HRs were 1.22 (95% CI 1.20-1.24) and 2.40 (95% CI 2.29-2.51), respectively. In men and women with type 2 diabetes and time-updated mean HbA1C ≤6.9% (52 mmol/mol), HRs for coronary events were 1.15 (95% CI 1.13 to 1.18, p<0.001) and 1.26 (95% CI 1.22 to 1.30, p<0.001), respectively, as compared with controls.
Adjusted HRs for AMI or CHD death and 95% CIs for time-updated mean HbA1c, albuminuria and eGFR categories versus the reference group examined by Cox regression
Adjusted HRs for AMI or CHD death and 95% CIs for time-updated mean HbA1c categories together with albuminuria and eGFR versus the reference group examined by Cox regression
Among patients with eGFR of 60–90 mL/min and CKD stage 2, HRs for coronary events were 1.17 (95% CI 1.15 to 1.19, p<0.001), and four times as high as that among controls (4.25, 95% CI 3.79 to 4.78, p<0.001) with eGFR <15 mL/min or dialysis (ie, end-stage renal disease or CKD stage 5). In men and women with type 2 diabetes and time-updated mean HbA1c 6.9% (≤52 mmol/mol), normoalbuminuria and eGFR ≥60 mL/min, HRs for coronary events were 0.94 (95% CI 0.90 to 0.98, p=0.0014) and 0.98 (95% CI 0.93 to 1.04, p=0.56), respectively, compared with controls.
Risk of AMI and CHD death by 10 mmol/mol HbA1c increase
The relationship between continuous time-updated mean HbA1c (per 1% (10 mmol/mol) increase) and risk of CHD events was investigated among patients with type 2 diabetes. The HR for AMI and CHD death was 1.23 (95% CI 1.22 to 1.24) when adjusted for age and sex, 1.21 (95% CI 1.20 to 1.23) and 1.26 (95% CI 1.24 to 1.27) for men and women respectively, and 1.19 (95% CI 1.18 to 1.20) when adjusted for time-updated diabetes duration, education, birth in Sweden and comorbidities prior to baseline, 1.18 (95% CI 1.16 to 1.19) and 1.21 (95% CI 1.19 to 1.22) for men and women respectively. In further adjustments, models 3A–3D, the HRs for 1% increase in HbA1c on AMI and CHD death ranged between 1.17–1.23 for women and 1.16–1.18 for men.
Discussion
The present population-based study involving more than 400 000 individuals with type 2 diabetes from the Swedish NDR and more than 2 million matched controls showed an excess risk of AMI and death from CHD in type 2 diabetes of 67%, which decreased to 42% after adjustment for country of birth, diabetes duration, education level and comorbidities. Furthermore, the excess risk of AMI and CHD death at any age was higher for women with type 2 diabetes compared with men.
A previous meta-analysis of 64 cohorts19 including more than 800 000 individuals showed that the relative risk for CHD associated with diabetes compared with no diabetes was 2.82 (95% CI 2.35 to 3.38) in women and 2.16 (95% CI 1.82 to 2.56) in men.
In several studies20 21 where the risk of CHD was analysed separately in men and women, the effect of diabetes was greater in women than men. Although there was a higher absolute risk for AMI and CHD in men with type 2 diabetes, the higher relative risk in women may have been due to the superior survival of women without diabetes. A pooled analysis19 showed that the presence of diabetes conferred a 44% (95% CI 27% to 63%) greater excess risk of CHD in women compared with men. This greater excess coronary risk may be explained by biological gender differences that confer more adverse cardiovascular risk profiles among women than men with diabetes.
In our study the excess risk of AMI and CHD death was higher in individuals with type 2 diabetes with worsening glycaemic control and renal complications. Other studies have also found an association between renal complications and mortality.22 23 However, higher relative risk for AMI and CHD death was found in younger patients, whereas absolute risk was higher in older patients.
The excess risk for AMI and CHD death in the fully adjusted model was lower compared with previous studies5 6 and converged to that in the general population in both men and women with type 2 diabetes without prior AMI, on-target HbA1c and no renal complications. In two cohorts aged 50 years or older with type 2 diabetes from November 1986 to November 2008, higher mean HbA1c values were associated with increased risk of all-cause of mortality and cardiac events.24
A previous study25 showed the benefit of glucose lowering, assuming a 15% reduction in the rate of cardiovascular events for every 1 percentage point reduction in HbA1c. The benefits of glycaemic treatment vary depending on patient age at diagnosis.
Furthermore, reduced eGFR (<60 mL/min/1.73 m2) at baseline and during follow-up was associated with increased risk of incident CHD in patients with type 2 diabetes.26 A previous study3 showed that long-term HbA1c on target and absence of kidney disease are associated with low mortality risk. Recently, a large Swedish study27 involving more than 400 000 patients with type 2 diabetes showed that individuals with on-target HbA1C, without renal complications and with normal blood pressure and lipid profiles appeared to have little or no excess risk of cardiovascular events as compared with the general population. In our study, the excess risk of coronary artery disease was evaluated in both men and women and the model was also adjusted for time-updated diabetes duration and comorbidities prior to baseline. Furthermore, unlike previous investigations, study covariates (HbA1c and eGFR) were time updated, thus all follow-up data were taken into account and opposed to only data at baseline.
The excess risk of AMI and CHD death in persons with type 2 diabetes diminished over time and was lower during the last eight calendar years of the study than during the first 7 years of follow-up.
Integrated diabetes care, improved patient education and recent advances in prevention, treatment and management can effectively help patients cope with the vast array of complications that can arise from diabetes and, therefore, may have reduced rates of cardiovascular complications among patients.
Screening patients with type 2 diabetes for cardiovascular risk is an important strategy for cardiovascular events.28
Additionally, previous studies29 30 have shown that intensive glycaemic control over long-time period is associated with reduced risk of major cardiovascular events and total mortality.
Our study implies that good glycemic control and avoiding renal complication are essential to reduce risk for coronary artery events in patients with type 2 diabetes. The current results thus support diabetes guidelines advocating early detection of diabetes, good glycaemic control, and encouraging use of lipid-lowering and antihypertensive medications. CVD risk will likely continue to converge to that in the general population if risk factors according to guidelines can be obtained in a broader population of type 2 diabetes. The greater excess risk of coronary artery disease among women with diabetes needs to be further investigated.
Furthermore, future diabetes care should also focus on reducing cardiovascular risk in patients who have existing renal complications and this group of patients should be treated more aggressively with regard to lipid-lowering agents, smoking cessation and lifestyle interventions.
Strengths of the current study include a large population of patients with type 2 diabetes and use of NDR data allowing for comprehensive understanding and ascertainment of information. The epidemiological definitions of type 2 diabetes and outcomes are well validated. For most patients, at least one measurement of HbA1c, grade of albuminuria and eGFR was collected. More than 2 million controls were included, and information on education level and coexisting diseases was available over a period of at least 11 years before start of follow-up.
There are several limitations of this study. First, some variables that may be associated with AMI and CHD death were not available on an individual level for controls. Second, residual bias could persist owing to unmeasured or imprecisely measured potential confounding factors (eg, dietary intake and physical activity, respectively). Third, our data were derived from a higher income country with equitable access to diabetes care at low cost to patients.
In summary, the excess risk of AMI and CHD death in patients with type 2 diabetes without prior AMI was higher than controls, and primarily in those with worsening glucose control and renal function, although it converged to that in the general population in patients with HbA1c on target and without renal complications. Higher excess risk for AMI and CHD death was also found in women than men with diabetes.
Acknowledgments
We thank all the data-collecting clinicians and staff at the National Diabetes Register, and Joseph W Murphy for editorial assistance.
References
Footnotes
Contributors MT and ML drafted the manuscript, with AR revising it for important intellectual content. AP performed the statistical analysis. SG and AMS contributed to data collection. All authors contributed to the study design, data interpretation and to manuscript drafting and approval. ML is the guarantor of this work and, as such, had full access to all data in the study and takes responsibility for the integrity of data and accuracy of the analysis.
Funding The study was financed by grants from the Swedish Society of Medicine and the Health and Medical Care Committee of the Regional Executive Board, Region Västra Götaland, Sweden, the Swedish State under the Agreement Concerning Research and Education of Doctors; the Swedish Heart and Lung Foundation; and the Swedish Research Council (SIMSAM).
Competing interests None declared.
ML has received honoraria or been consultant for Astra Zeneca, DexCom, Eli Lilly, MSD, Rubin Medical and Novonordisk and received research grants from Astra Zeneca, DexCom and Novonordisk.
Patient consent for publication Not required.
Ethics approval Regional Ethics Review Board at University of Gothenburg, Sweden.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All data relevant to the study are included in the article or uploaded as supplementary information.