Article Text

Abstract
Objective We compared percutaneous coronary intervention (PCI) with coronary artery bypass grafting (CABG) for the treatment of left main coronary artery (LMCA) disease by conducting a systematic review and meta-analysis of randomised controlled trials (RCTs).
Methods RCTs of PCI versus CABG in patients with LMCA stenosis were identified from MEDLINE, the Cochrane Library and search of bibliographies to November 2016. Study-specific HRs with 95% CIs were aggregated for all-cause mortality, major adverse cardiac and cerebrovascular events (MACCE), and other cardiovascular events at time points of 30 days, 1 year and 3 years and beyond.
Results Six RCTs comprising 4700 patients were included. There were no significant differences in risk of all-cause mortality in pooled analysis of relevant trials at 30 days (0.61, 95% CI 0.27 to 1.36), 1 year (0.66, 95% CI 0.42 to 1.04), and 3 years and beyond (1.04, 95% CI 0.81 to 1.33), comparing PCI with CABG. There was no significant difference in the risk of MACCE at 30 days (0.72, 95% CI 0.51 to 1.03) and 1 year (1.16, 95% CI 0.94 to 1.44); however, PCI was associated with a higher risk of MACCE compared with CABG during longer-term follow-up (1.27, 95% CI 1.12 to 1.44). Composite outcome of death, stroke or myocardial infarction was lower with PCI at 30 days (0.67, 95% CI 0.49 to 0.92). Repeat revascularisation was increased at 1 year and at 3 years and beyond for PCI.
Conclusions All-cause mortality rates are not significantly different between PCI and CABG at short-term and long-term follow-up. However, PCI is associated with a reduction in the risk of major cardiovascular outcomes at short-term follow-up in patients with LMCA stenosis; but at long term, MACCE rate is increased for PCI.
- interventional cardiology
- coronary intervention (pci)
- coronary stenting
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Left main coronary artery (LMCA) disease has a worse prognosis than any other form of obstructive coronary artery disease.
Treatment options for unprotected LMCA disease include percutaneous coronary intervention (PCI) and coronary artery bypass grafting (CABG); however, based on results of randomised controlled trials (RCTs) with short-term follow-ups, European and US guidelines on revascularisation and management of coronary artery disease recommend that most patients with LMCA disease preferably undergo CABG.
Some trials have suggested that PCI might be a valid alternative to CABG in the treatment of LMCA disease; however, the evidence has been inconsistent.
What this study add?
All-cause mortality rates are not significantly different between PCI and CABG treatment groups at both short-term and long-term follow-up.
This meta-analysis suggests that PCI compared with CABG may be associated with a reduction in the risk of major cardiovascular outcomes at short-term follow-up in patients with LMCA stenosis. However, at long term, repeat revascularisation and major adverse cardiac and cerebrovascular event rates are increased for PCI.
How might this impact on clinical practice?
The overall data suggest that PCI, which is associated with shorter hospital stay and rapid return to normal daily activities with well-documented early safety outcomes, may be an acceptable treatment alternative to CABG in patients with LMCA disease, in the context of short-term major cardiovascular outcomes.
Introduction
Left main coronary artery (LMCA) disease has a worse prognosis than any other form of obstructive coronary artery disease.1 Modern invasive therapy of percutaneous coronary intervention (PCI) instead of coronary artery bypass grafting (CABG) for the treatment of unprotected LMCA disease has largely increased in clinical practice due to an extensive body of favourable evidence from both observational studies and randomised trials.2 However, the European and US guidelines on revascularisation and management of coronary artery disease still recommend that most patients with LMCA disease should preferably undergo CABG.3 4 Recent evidence from large randomised controlled trials (RCTs) have suggested that PCI with contemporary new generation drug-eluting stents (DESs) is an acceptable alternative for selected patients with LMCA disease.5 6 Some trials have suggested that PCI might be a valid alternative to CABG in the treatment of LMCA based on a suitable coronary anatomy. In a meta-analysis of four RCTs, Capodanno and colleagues showed no significant differences in 1-year rates of all-cause mortality and major cardiovascular outcomes, when PCI was compared with CABG.7 Previous guidelines and current clinical practice approaches are, however, based on RCTs with relatively short follow-up times or subgroup analyses with limited number of fatal cardiovascular outcomes.8–11 Indeed, trials with longer-term follow-up and adequate number of events are required to examine whether observed differences between PCI and CABG would be similar over time, with respect to various major adverse events.
Results from the recently reported Evaluation of XIENCE versus Coronary Artery Bypass Surgery for Effectiveness of Left Main Revascularization (EXCEL) trial indicate that in patients with LMCA disease, PCI with everolimus-eluting stents was non-inferior to CABG with respect to the composite of outcomes of death, stroke or myocardial infarction (MI) at 3 years.6 In the most recent published Nordic-Baltic-British left main revascularisation study (NOBLE),5 key findings suggested that CABG could be a better treatment option than PCI with respect to all composite adverse events, although all-cause mortality and fatal cardiovascular events were not different between the two treatment strategies for LMCA. Differences in the definition of main outcomes with various follow-up times may explain the inconsistencies observed between published studies; therefore, there is need to conduct a more detailed synthesis of existing evidence with comprehensive assessment of outcomes. Given the high level of clinical interest in this topic and with the publication of newer trials since the last relevant meta-analysis on the topic in modern cardiology era, we conducted an updated meta-analysis to evaluate both short-term and long-term all-cause mortality and major cardiovascular outcomes when PCI was compared with CABG for the treatment of LMCA disease.
Methods
Data sources and search strategy
We conducted this review using a predefined protocol and in accordance with PRISMA guidelines (online supplementary appendix 1).12 We sought randomised intervention studies published before 9 November 2016 (date last searched) using MEDLINE and the Cochrane electronic databases. The computer-based searches combined terms related to (1) the interventions (eg, PCIs and CABG) and (2) population (eg, LMCA) in humans, without any language restriction. Details on the search strategy are provided in online supplementary appendix 2. Full texts were retrieved from studies that satisfied all selection criteria. Reference lists of selected studies and relevant reviews identified on the topic were searched for additional publications that were missed by the original search.
Supplementary file 1
Study selection and eligibility criteria
Randomised intervention studies were sought that had reported on the use of PCI versus CABG for the treatment of LMCA stenosis and reported data on a variety of safety and efficacy outcomes. RCTs or prespecified subanalyses of RCTs were eligible for inclusion if they (1) assessed the effects of PCI compared with CABG in randomised patients; (2) enrolled patients with isolated LMCA or patients with LMCA and multivessel coronary artery disease; and (3) and reported outcomes such as all-cause mortality, major adverse cardiac and cerebrovascular events (MACCE) (defined as the composite of death, MI, cerebrovascular accident (CVA) or stroke, or target vessel revascularisation (TVR)), MI, CVA and repeat revascularisation. We only included studies that conformed to our prespecified outcome definitions and excluded studies that used broader outcome definitions (involving incident heart failure, cardiac arrhythmia, peripheral arterial disease, venous thrombosis or pulmonary embolism). Non-randomised studies were not included in the current analysis.
Data extraction
After an initial screen of abstracts by one reviewer (JAL), potentially relevant articles were acquired. Each article was assessed by two independent reviewers (JAL, SKK) using the inclusion criteria and a consensus was reached in case of any inconsistency, with the involvement of a third (TM). A predesigned data extraction form was used to obtain relevant information. These included, where appropriate, study-level information on study design; baseline population including proportion of men; location; average age at baseline; numbers enrolled and randomised; allocation concealment; blinding; and outcomes of all-cause mortality, MACCE, MI, stroke and repeat revascularisations at time points of 30 days, 1 year, 3 years, 5 years and 10 years. Where available, risk estimates for each outcome of interest were also extracted.
Assessing the risk of bias
Two reviewers independently rated the methodological quality of the studies using the Cochrane Collaboration’s risk of bias tool.13 This tool evaluates seven possible sources of bias: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting and other bias. For each individual domain, studies were classified into low, unclear and high risk of bias.
Statistical analyses
Summary measures were presented as HRs with 95% CIs. The inverse variance-weighted method was used to combine summary measures using random-effects models to account for the effect of between-study heterogeneity. Subsidiary analyses employed fixed effects models. Statistical heterogeneity across studies was quantified using the Cochrane χ2 statistic and the I2 statistic.14 In analysis specified post hoc which was based on available data, we conducted a subgroup analysis by SYNergy between percutaneous coronary intervention with TAXus and cardiac surgery (SYNTAX) scores to compare major cardiovascular outcomes between the two treatment groups. We assessed the potential for small study effects such as publication bias through formal tests, namely Begg’s funnel plots and Egger’s regression symmetry tests.15 STATA release V.14 (Stata LP) software was used for all statistical analyses.
Results
Study identification and selection
Our initial search of relevant databases and manual scanning of reference lists identified 676 potentially relevant citations. After screening based on titles and abstracts, 31 articles remained for further evaluation. Following detailed assessments, 20 articles were excluded. The remaining 11 articles5 6 8–11 16–20 based on six unique RCTs met our inclusion criteria and were included in the meta-analysis (online supplementary appendix 3).
Study characteristics and quality
Table 1 summarises the key characteristics of the randomised trials included in the review. In aggregate, the included trials published between 2008 and 2016 comprised 4700 participants (2349 assigned to PCI and 2351 assigned CABG) with LMCA disease. All RCTs were prospective, open-label multicentre trials. Three trials were single country studies conducted in Poland, Germany and South Korea, and the other three recruited patients from multiple countries in Europe and North America. The baseline age of participants ranged from 18 to 80 years. Except for one trial which was a prespecified subgroup analysis of patients with LMCA disease from the SYNTAX trial, all eligible studies were RCTs that compared PCI and CABG in LMCA disease. All six trials demonstrated a high risk of bias for blinding of participants and personnel, as assessed using the Cochrane Collaboration tool. In addition, all trials had an unclear or high risk of bias for allocation concealment and a low risk of bias in all other areas of study quality (online supplementary appendix 4).
Characteristics of randomised clinical trials of PCI versus CABG included in meta-analysis
All-cause mortality
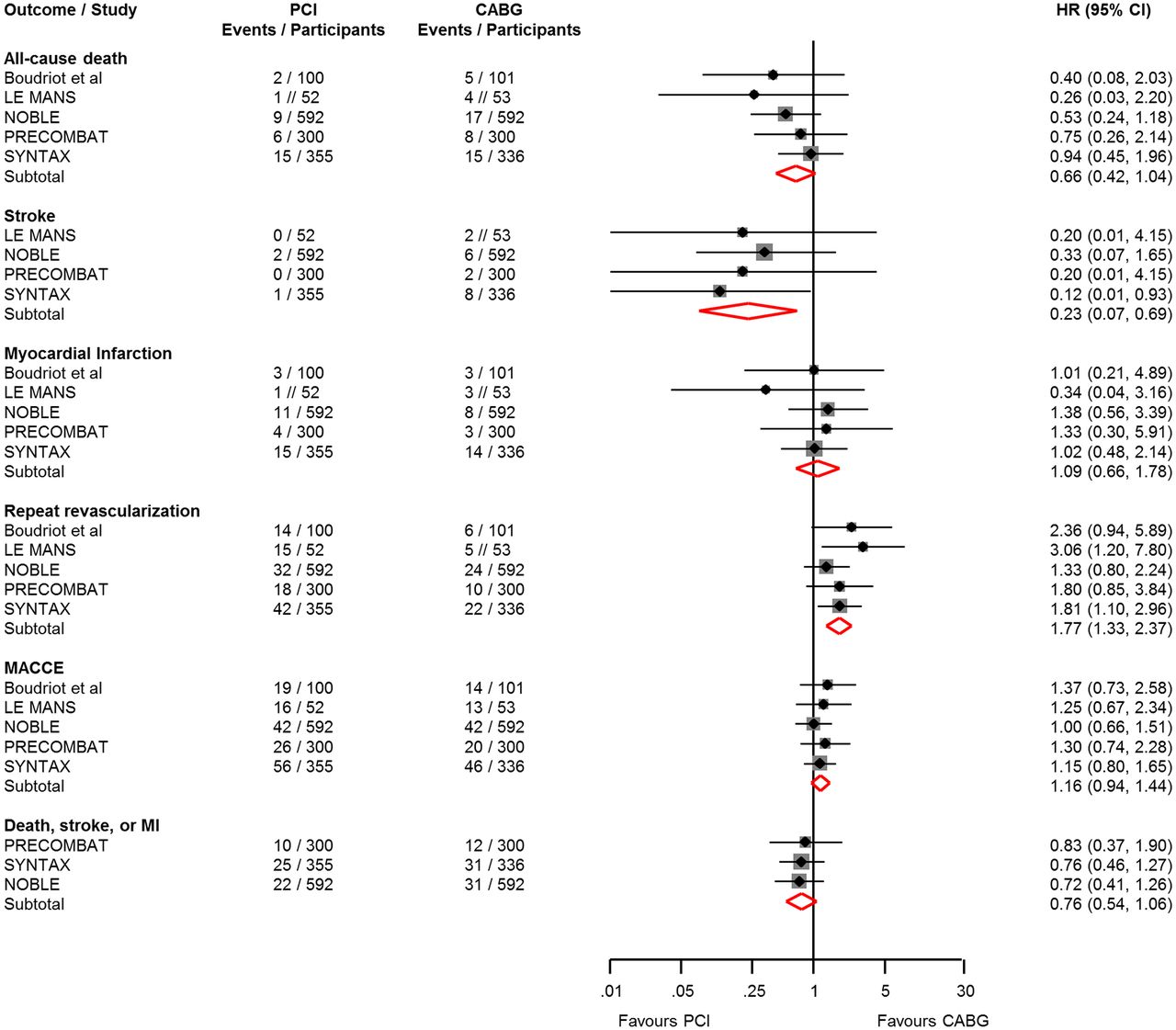
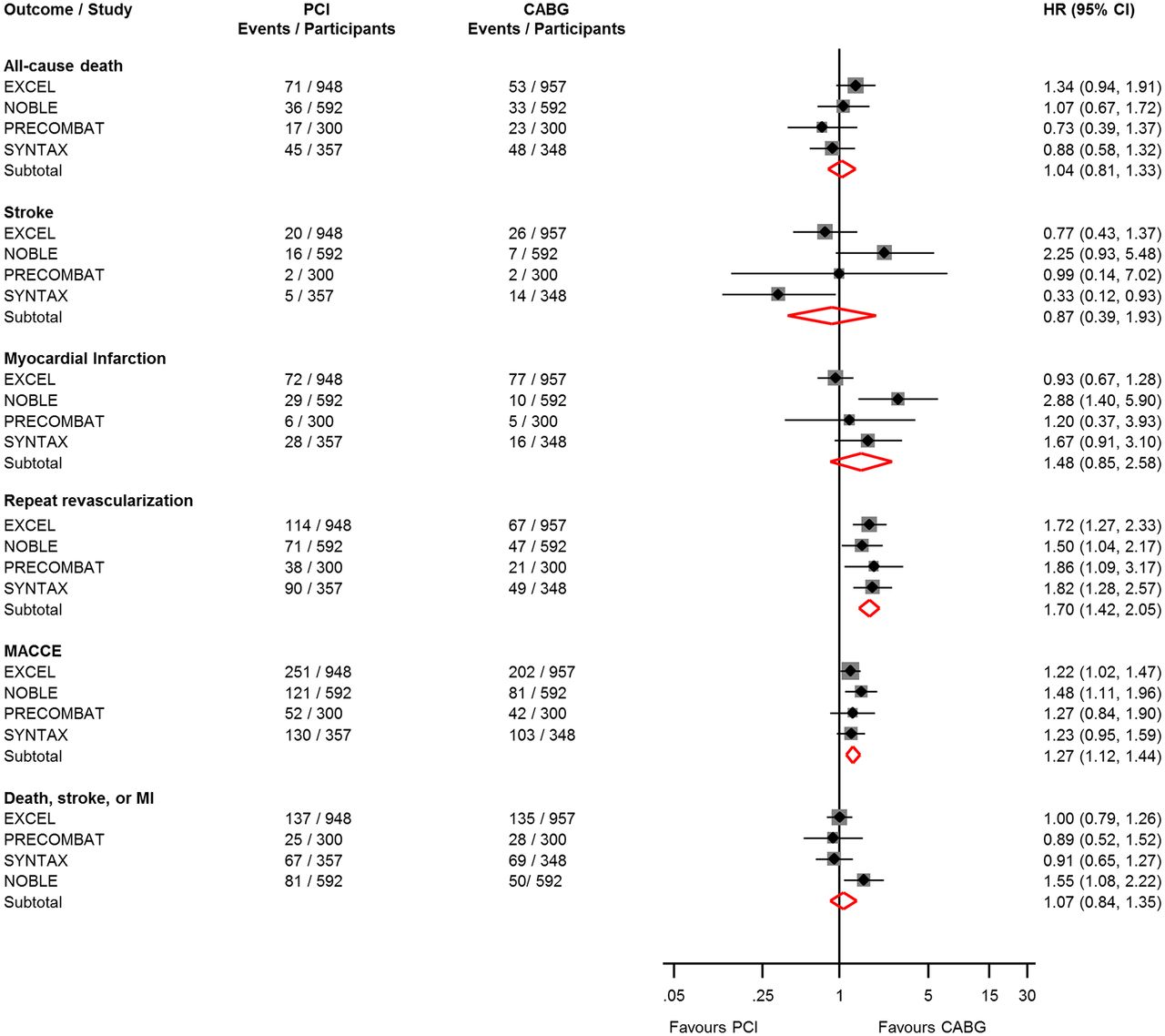
All-cause mortality outcomes during the follow-up from 30 days until 3 years and beyond are shown in figures 1-3. There was no statistically significant difference in risk of all-cause mortality in pooled analysis of relevant trials at 30 days (three trials), 1 year (five trials) and at 3 years and beyond (four trials) of follow-up when PCI was compared with CABG: 0.61 (95% CI 0.27 to 1.36), 0.66 (95% CI 0.42 to 1.04) and 1.04 (95% CI 0.81 to 1.33), respectively; although a trend towards lowered risk of all-cause death after PCI was observed during the 1-year follow-up (figure 2). Evidence of heterogeneity between the contributing trials at all time points was not significant (I2=5%, 0%–90%; P=0.348), (I2=0%, 0%–79%; P=0.676) and (I2=21%, 0%–88%; P=0.282), respectively.

Effect of PCI on 30-day risk of all-cause mortality and major cardiovascular outcomes. CABG, coronary artery bypass grafting; CI, confidence interval (bars); EXCEL, Evaluation of XIENCE versus Coronary Artery Bypass Surgery for Effectiveness of Left Main Revascularization; MACCE, major adverse cardiac and cerebrovascular events; MI, myocardial infarction; NOBLE, Nordic-Baltic-British left main revascularisation study; PCI, percutaneous coronary intervention.

Effect of PCI on 1-year risk of all-cause mortality and major cardiovascular outcomes. CABG, coronary artery bypass grafting; CI, confidence interval (bars); EXCEL, Evaluation of XIENCE versus Coronary Artery Bypass Surgery for Effectiveness of Left Main Revascularization; MACCE, major adverse cardiac and cerebrovascular events; MI, myocardial infarction; NOBLE, Nordic-Baltic-British left main revascularisation study; PCI, percutaneous coronary intervention.

{kind=link}
{kind=link}
{kind=link}
Effect of PCI on 3 to 5-year risk of all-cause mortality and major cardiovascular outcomes. CABG, coronary artery bypass grafting; CI, confidence interval (bars); EXCEL, Evaluation of XIENCE versus Coronary Artery Bypass Surgery for Effectiveness of Left Main Revascularization; MACCE, major adverse cardiac and cerebrovascular events; MI, myocardial infarction; NOBLE, Nordic-Baltic-British left main revascularisation study; PCI, percutaneous coronary intervention.
Major adverse cardiac and cerebrovascular events
Figure 1-3 presents summary of HRs for MACCE at time points 30 days, 1 year, and 3 years and beyond for PCI compared with CABG. Comparing PCI with CABG, there was no significant difference in the risk of MACCE at 30 days and at 1 year: 0.72 (95% CI 0.51 to 1.03) and 1.16 (95% CI 0.94 to 1.44), respectively. However, pooled analysis of four trials showed PCI to be associated with an increased risk of MACCE compared with CABG at 3 years and beyond (1.27, 95% CI 1.12 to 1.44). The pooled HR was 1.27 (95% CI 1.12 to 1.44) using a fixed effects model, without evidence of heterogeneity between the trials (I 2 =0%, 0%–85%; P=0.716). In the only trial that reported clinical endpoints at 10-year follow-up, there was no difference in the risk of MACCE, when PCI was compared with CABG (HR 0.64 95% CI 0.37 to 1.11).9
Other cardiovascular outcomes
Risks for other cardiovascular outcomes including stroke and MI at short-term and long-term points for PCI compared with CABG in trials based on pooled analysis are shown in figures 1-3. At 30 days and 1 year, stroke was less frequent event when PCI was compared with CABG: 0.39 (95% CI 0.16 to 0.94) and 0.23 (95% CI 0.07 to 0.69), respectively. However, the risk of stroke was similar during the long-term follow-up (figure 3).
The risk of MI was not different in pooled analysis of relevant trials at 30 days (four trials), 1 year (five trials), 3 years and beyond (four trials), and at 10 years (one trial): HRs were 0.76 (95% CI 0.54 to 1.06), 1.09 (95% CI 0.66 to 1.78), 1.48 (95% CI 0.85 to 2.58) and 0.88 (95% CI 0.24 to 3.33), respectively. There was no statistically significant evidence of heterogeneity between the included trials at 30 days and 1 years: (I2=0%, 0%–85%; P=0.414) and (I2=0%, 0%–79%; P=0.833) respectively, although there was moderate evidence of heterogeneity between trials with long-term follow-up (I2=67%, 5%–89%; P=0.027).
Composite endpoint of death, stroke or MI was lower after PCI compared with CABG at short-term follow-up (30 days) (figure 1). PCI reduced the risk of the composite outcomes of death, stroke or MI at 30 days (two trials) (HR 0.67, 95% CI 0.49 to 0.92), whereas there was no difference in the risk of composite endpoints between two intervention strategies at 1 year (three trials) (HR 0.76, 95% CI 0.54 to 1.06) and 3 years and beyond (four trials) (HR 1.07, 95% CI 0.84 to 1.35). Comparing PCI with CABG, the difference in the risk of repeat revascularisation at 30 days (four trials) was not significant (HR 0.64, 95% CI 0.34 to 1.21), while the risk of repeat revascularisation was increased at 1 year (five trials) (HR 1.77, 95% CI 1.33 to 2.37) and at 3 years and beyond (four trials) (HR 1.70, 95% CI 1.42 to 2.05) (figure 3).
Subgroup analysis
Comparing PCI with CABG, there was no significant difference in the risk of MACCE at 5 years in patients with low, intermediate or high SYNTAX scores at baseline (online supplementary appendix 5). Similarly, there was no difference in the risk of composite endpoint of death, stroke or MI in patients with low, intermediate or high SYNTAX scores at baseline (online supplementary appendix 6).
Publication bias
Under visual examination, funnel plots for those analyses that involved five or more studies were symmetrical and Egger’s regression tests showed no statistical evidence of publication bias for all analyses (online supplementary appendix 7).
Discussion
In this meta-analysis from all available RCTs involving patients with unprotected LMCA stenosis, PCI when compared with CABG was found to be associated with a lower risk of stroke and the composite outcomes of death, stroke or MI during the shortest-term follow-up. However, there was no significant difference in all-cause mortality outcomes between both treatment groups at short-term and long-term follow-up. PCI was related to an increased risk of MACCE and repeated revascularisations when compared with CABG during longer-term follow-up. Based on pooled analysis of the few available trials that reported these data, the rates of MACCE and composite outcomes of death, stroke or MI at 3–5 years were not significantly different between the two treatment groups in patients with low, intermediate or high SYNTAX scores at baseline. Though several meta-analyses have recently been published on this topic,21–30 providing complementary evidence to each individual study. In general, our findings concur well with the results of these studies; we also report a number of relevant findings that have not been comprehensively reported. First, we reported differences in short-term and long-term outcome events between PCI and CABG; we felt this was the most appropriate way of summarising the data given that individual studies reported their outcomes at specific time points. Given that outcome events are time-dependent, such findings would be useful in selecting most appropriate invasive treatment strategy among patients with LMCA stenosis. Unlike some of the recent reviews,21 22 25–27 our study reported outcomes based on the time points of 30 days, 1 year, 3 years and beyond, and 10 years though we do acknowledge that 10-year outcomes were only reported in one of the studies.9 Second, we conducted several formal tests to assess for evidence of publication bias, which is a strength of this updated meta-analysis.
A shorter hospital stay and rapid return to normal daily activities with documented early safety outcomes can be included as some of the advantages of PCI treatment. Previous studies have indicated that the implantation of DES for LMCA lesions might be a safe and feasible approach based on short-term and long-term follow-up results.6 9 31 The short-term risk of clinical adverse events has been similar between PCI and CABG for the treatment of LMCA stenosis.32 In a previous meta-analysis of three randomised trials and nine observational studies, the findings suggested that PCI with DESs is associated with favourable outcomes for mortality; composite endpoint of death, MI or stroke; and a higher risk of target vessel revascularisation compared with CABG in patients with LMCA disease.32 This meta-analysis with short-term outcomes suggested that there were trends towards lower risk of death, the composite endpoint of death, MI or stroke in the PCI-DES group compared with the CABG group at 1-year follow-up.32 Another meta-analysis of four randomised trials suggested that PCI was associated with non-statistically significant 1-year rates of MACCE, death and MI; a lower risk of stroke; and a higher risk of TVR compared with CABG among patients with LMCA.7 The current large data derived from all published RCTs on the topic and comprising approximately 5000 patients show statistically significant lower combined death, stroke and MI rates among patients treated with PCI compared with CABG at short-term follow-up (30 days). Although PCI seems to be a superior treatment option in the short term, both invasive treatment options are currently recommended for LMCA depending on the severity of coronary artery disease; however, major long-term clinical outcomes have been previously unclear.31
The current meta-analysis suggests that during longer-term follow-up from 3 to 5 years, additional adverse events are less frequent among patients treated with CABG and both treatment options result in similar prognostic profiles in the long term. Moreover, repeated revascularisation rate is higher among patients treated with PCI during long-term follow-up. Follow-up times over 3 years is required to examine whether additional differences between PCI and CABG may emerge over time; a full 5-year follow-up is currently being undertaken in the NOBLE and EXCEL trials.5 6 Moreover, patient-level meta-analysis of previous large-scale trials is of pivotal importance, particularly to assess the optimal stenting strategy and types of DES for LM bifurcation in patients with stable or unstable coronary artery disease. Over the last decade, improvements in PCI techniques and stent technology and an accumulation of operator experience have exponentially increased the number of PCIs performed to treat LMCA stenosis.
The original SYNTAX study11 has indicated that CABG should remain the standard treatment strategy for patients with complex lesions (high or intermediate SYNTAX scores), but PCI is a good option for patients with less complex coronary artery disease (low SYNTAX scores) or LMCA disease (low or intermediate SYNTAX scores). However, the SYNTAX scoring system may not always be useful to define patients with LMCA disease who are suitable for either PCI or CABG treatment. Indeed, the clinical use of the SYNTAX score may be more useful in patients with multivessel coronary artery disease than selecting patients for LMCA treatment strategies.
The previously published LE MANS trial using mainly bare metal stent (BMS) has reported the longest follow-up outcomes until now after random assignment of LMCA revascularisation strategies, although a relatively small number of patients largely limited the study conclusions.9 Thus, the overall evidence of using BMS in LM stenosis in older RCTs is quite limited and most of the current knowledge of the value of PCI in LM stenosis is based on the use of DES, which is the most recommendable stenting strategy in recent times. The LE MANS trial indicated a reduction of angina pectoris symptoms and improvement of left ventricular systolic function at 1-year and 5 year follow-up after LMCA revascularisation by PCI.33 In another relatively small randomised study comparing PCI and CABG, individual components of the combined endpoint revealed mixed results, whereas non-inferiority was confirmed for the difference in death and MI, although it was not established for the difference in repeat revascularisations.8 This was mainly caused by the higher rate of repeat revascularisation after PCI. However, fewer periprocedural adverse events occurred in the PCI group, which is likely due to its less invasive approach.8 At both short-term and long-term follow-up, PCI seemed to be protective of MI events, but the difference between the two invasive treatment strategies was not statistically significant, which could be attributed to the low event rate.
Other strengths of the current study include it being a comprehensive and updated assessment on the topic to date. The generalisability of our findings was enhanced by the involvement of data from all RCTs published so far. Formal tests were unable to detect publication bias for majority of analyses involving five studies or more and there was no evidence of substantial heterogeneity among contributing studies for all analyses. There are also some limitations of this meta-analysis which deserve consideration. The definition of outcomes such as MACCE was not uniform across all included RCTs. Indeed, MACCE is a combination of outcomes with various severity, which may lead to difficulties in interpretation of the results. The definition of any combined event which included postprocedural MI may be favourable for PCI. On the other hand, revascularisations are commonly performed due to worsened symptoms which may have effect on the preferred treatment strategy between PCI and CABG and their events rates. Though the meta-analysis was very comprehensive, it was based on six available RCTs, which precluded the ability to perform clinically relevant subgroup analyses. Second, there were only a few studies with appropriate number of outcomes at 30 days and 10 years which limit the interpretation of the results based on the shortest and longest follow-up time. Possible differences in quality of life and cost-effectiveness between PCI and CABG should be taken into consideration as supplementary outcomes in future studies; there is a need to investigate whether one of these invasive treatments might be more favourable with regard to quality of life and cost of treatment strategy-related outcomes.
Previous observational evidence has not indicated significant difference in all-cause mortality during the longer-term follow-up period between CABG and PCI.34 35 In earlier LMCA disease studies, first-generation DES and BMS with higher risk of restenosis and thrombosis were used in the PCI intervention groups, which may have had influenced the results of earlier published meta-analysis,7 whereas the most contemporary and largest trials with second-generation DES were included in this new meta-analysis. The study-level meta-analysis is not capable of detecting possible differences between stents. Given the limited data, it was not possible to conduct detailed subgroup or clinically relevant sensitivity analyses based on different stent types or complexity of coronary artery disease or other demographic characteristics. Further trials are needed and individual participant data meta-analysis may be required to show possible benefits in certain subgroups.
On the other hand, surgical techniques have improved during the last years and the use of the left internal mammary artery has been a standard of care option in the recent RCTs. Advanced surgical techniques such as off-pump strategy, arterial graft revascularisation and transoesophageal ultrasonography are largely implemented, which have partly explained lower frequent adverse event rates after CABG in most recent trials. Although PCI versus CABG trials were focused mainly on patients with LMCA with low and intermediate SYNTAX scores,6 11 some recent trials have included patients who had a more complex coronary anatomy.5 However, PCI is not used for all kinds of heavily calcified and tortuous lesions and patients with more complex coronary artery disease cannot be included in RCTs comparing PCI and CABG.
Conclusion
The findings indicate that PCI treatment of LMCA is associated with a reduction in the risk of major cardiovascular outcomes at short-term follow-up. However, all-cause mortality rates were not significantly different between treatment groups at both short-term and long-term follow-up. PCI treatment is associated with an increased rate of repeat revascularisation during long-term follow-up; however, this was an expected finding from this pooled analysis and can be considered as a characteristic of PCI strategy with the treatment of only haemodynamically significant lesions at the time of index LM revascularisation. The study data suggests that PCI is an acceptable alternative to CABG in patients with LMCA disease, although patients with high anatomical complexity of LMCA disease may be preferably treated with CABG. Based on the overall findings, PCI is an acceptable option when the coronary anatomy is suitable; taking into consideration operative risks and expected benefits. However, longer-term follow-up results of RCTs are needed to update LM revascularisation guidelines.
References
Footnotes
Contributors JAL, SKK, MN, KK, LT and THM conceived and designed the study. JAL, SKK, MN, KK, LT and THM acquired data. JAL and SKK analysed and interpreted the data. JAL drafted the manuscript. JAL, SKK, MN, KK, LT and THM critically revised the manuscript for important intellectual content. JAL and THM supervised the study.
Competing interests None declared.
Ethics approval Study level meta-analysis.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The full dataset is available from the corresponding author.