Article Text

Abstract
Background Patients with implantable cardioverter defibrillators (ICD) experience anxiety, depression and reduced quality of life (QoL).
Objectives This mixed-methods systematic review evaluates whether ICD support groups have a beneficial effect on mental well-being.
Methods Literature searches were carried out in MEDLINE, Embase, CINAHL, PsycINFO and Web of Science. Eligible studies investigated patient-led support groups for ICD patients aged 18 years or older, using any quantitative or qualitative design. The Mixed-Methods Assessment Tool was used to assess quality. Meta-analysis of measures of mental well-being was conducted. Thematic synthesis was used to generate analytic themes from the qualitative data. The data were integrated and presented using the Pillar Integration Process.
Results Ten studies were included in this review. All studies bar one were non-randomised or had a qualitative design and patients had self-selected to attend a support group. Five contributed to the quantitative data synthesis and seven to the qualitative synthesis. Meta-analysis of anxiety and QoL measures showed no significant impact of support groups on mental well-being, but qualitative data showed that patients perceived benefit from attendance through sharing experiences and acceptance of life with an ICD.
Discussion ICD support group attendance improved the patients’ perceived well-being. Attendees value the opportunity to share their experiences which helps to accept their new life with an ICD. Future research could consider outcomes such as patient acceptance and the role of healthcare professionals at support groups.
- Defibrillators, Implantable
- Ventricular Fibrillation
- Meta-Analysis
Data availability statement
Data sharing not applicable as no datasets generated and/or analysed for this study.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Patients with implantable cardioverter defibrillators (ICDs) experience anxiety, depression and reduced quality of life (QoL). Patient support groups are recommended in national guidelines for follow-up of patients with ICDs.
WHAT THIS STUDY ADDS
Patients perceive an improvement in overall mental well-being from attending ICD support groups, although this is not supported by quantitative measures of anxiety and QoL. Acceptance may be a more sensitive measure of the effect of support groups.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Support groups may be helpful for patients struggling to accept their ICD, and patient discussion should be encouraged to allow sharing of experiences. Further research is needed to determine the optimal format of support groups.
Introduction
Implantable cardioverter defibrillators (ICDs) were introduced to prevent sudden cardiac death (SCD), most frequently caused by coronary artery disease (80% of cases).1 ICDs were originally implanted as a secondary prevention strategy, with guidelines being expanded in the early 2000s to include patients at risk of SCD (primary prevention). Implant rates in England quadrupled between 2002 and 2020.2 3
Patients with ICDs experience anxiety and depression.4 5 This may be present in patients with or without ICD-delivered shocks, but is increased by higher incidence of shocks.6 The delivery of a shock to restore sinus rhythm has been shown to cause a transient reduction in quality of life (QoL).7 Anxiety and reduced QoL are associated with increased readmissions and 1-year mortality for ICD patients.8 It has also been suggested that there is a correlation between anxiety and the occurrence of arrhythmia.9
A range of psychological and educational interventions to improve psychological outcomes for patients with ICDs have been investigated.10–16 The results of these studies are promising but methodological limitations restrict the extent to which they can be generalised and applied to clinical practice. At present, UK guidance for ICD follow-up17 and high-profile cardiac charities18 19 encourage participation in patient support groups. Patient support groups are defined as groups with aims determined by the participants (rather than the providers) and without structured curriculum or end date.20 Support groups also provide an option for supportive care using limited healthcare resources.21
There are many support groups for patients with chronic conditions such as cancer and heart failure.22–24 These groups provide benefits for the patients, such as the opportunity to meet and talk with people with the same condition or experiences, and for information provision and exchange.22–24 Although ICD recipients share experiences of patients with other long-term conditions, their risk of recurrent shocks is something unique to these patients and it remains to be seen whether support groups also have a beneficial impact on well-being in ICD patients.
The objectives of this mixed-methods systematic review are to: (1) evaluate the effectiveness of patient support groups on mental well-being in patients living with ICDs using a meta-analysis and (2) define the perceived benefits and challenges of attending a support group, using a qualitative synthesis.
Methods
Design and registration
This mixed-methods systematic review was prospectively registered (PROSPERO: CRD42021262058) and reported in line with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement.25
Inclusion criteria
Participants
The patients in the studies had to be 18 years or older and have had an ICD implanted, including single or dual, or biventricular devices.
Comparators
To be defined as a patient support group, it must have (1) aims determined by the participants rather than the providers and (2) no structured curriculum with a defined beginning or end. This definition of a patient support group is that used in a published scoping review.20 Involvement of healthcare professionals (HCPs) to provide education was permitted provided the objectives of the group were patient-led. Forms of HCP-led psycho-social support, including cognitive behavioural therapy, exercise programmes and psycho-educational interventions with a clear curriculum and set duration were excluded. The comparison was standard care of the ICD without attendance of a support group.
Outcomes
For quantitative studies the main outcomes were selected a priori and are ‘changes in measures of mental well-being’. The definition of ‘mental well-being’ is complex but it is widely understood to mean more than simply absence of mental illness and includes the ability to cope with stressors and work productively.26 We chose to include measures of QoL, anxiety and depression as outcomes which are aspects of mental well-being. Instruments to assess these outcomes included general (ie, State-Trait Anxiety Index) and ICD specific (ie, Florida Shock Anxiety Scale (FSAS)) measures. QoL measures included but were not limited to the Short-Form 36 (SF-36) and the Quality of Life Index (QLI). ‘Social support’ was added later in the analysis as it was frequently measured. For qualitative studies, the outcomes were anxiety, depression, QoL, benefits and challenges of attending support groups.
Types of evidence
A range of study designs, including quantitative, qualitative and mixed-methods designs, were included to allow for review of the totality of existing evidence.
Search strategy and screening
Five databases were searched in July 2021. The initial search strategy was developed for MEDLINE (see table 1) and adapted for Embase, CINAHL, PsychINFO and Web of Science.
Medline search strategy
A search filter was used to include all papers published from January 1980 until July 2021. A search of grey literature included hand searches of conference abstracts between 2019 and 2021 (British Cardiovascular Society and Heart Rhythm Congress). Reference lists of included articles were searched for potential eligible papers. Non-English language articles were excluded. KHS screened all records by title before two authors (KHS/PAC) screened potentially eligible abstracts and full-texts. Where there was disagreement, a third reviewer’s (MA) opinion was sought.
The database search was repeated in July 2022 to check for new publications. No eligible papers were identified.
Quality assessment
The Mixed-Methods Assessment Tool (MMAT)27 was used by two independent reviewers (KHS and PAC/KC) to assess quality and risk of bias. The MMAT was designed to appraise the methodological quality of five categories of studies (qualitative research, randomised controlled trials, non-randomised studies, quantitative descriptive studies and mixed-methods studies), and was therefore chosen as the most suitable tool for the current study due to the methodological variety of studies included.
Data extraction and analysis
KHS extracted the design, population, sex, age, comparator, outcome measures, instruments used and key findings from the included articles. Quantitative results were grouped by outcomes indicative of ‘better mental well-being’ including measures of anxiety and QoL. A meta-analysis using pooled outcome measurements was conducted using Review Manager V.5.4.28 This approach has been used in other published studies.29 30 To allow comparison of data from different instruments, mental well-being data of each parameter was normalised to the average control value for that parameter. Where multiple measures were used in a study, a single parameter was chosen for the analysis with preference to measures of anxiety over generalised QoL. Adjusted data were pooled to calculate weighted standardised mean difference and 95% CIs. Overall effect was calculated using a Z-test.
Qualitative results were uploaded verbatim to NVivo V.11 and thematic synthesis methods31 used to generate themes. KHS deductively coded for anxiety and depression, and quality of life, and developed inductive codes around perceived benefits and challenges of attending support groups. The quantitative and qualitative data were then integrated and are presented in a joint display using the Pillar Integration Process (PIP).32 A mixed-methods systematic review using the PIP was chosen as the PIP permits grouping of outcomes based on conceptual ideas, rather than the quantity of each item or the research methods used.32
Patient and public involvement
The results of this study were disseminated to members of a Patient and Public Involvement group.
Results
Study characteristics
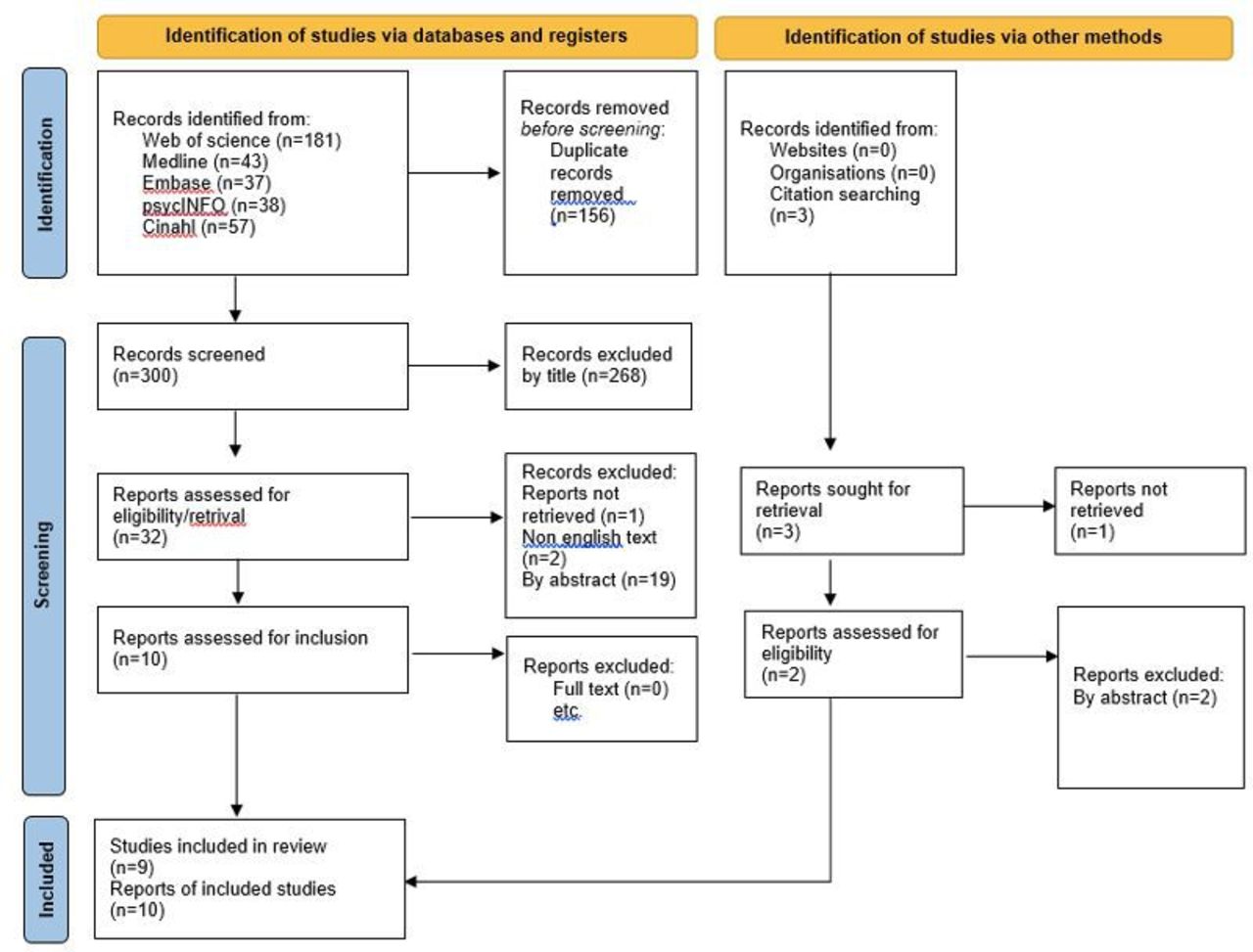
From 456 records identified, 10 papers were eligible for inclusion (figure 1). Most records were excluded because they did not include a support group. Two studies were excluded because the support group intervention was restricted to a set period and therefore had a set curriculum.10 33 Tables 2 and 3 include the summary characteristics and results for the 10 studies: one randomised controlled trial (RCT),34 two observational studies,35 36 two mixed-methods studies,37 38 four qualitative studies39–42 and one service evaluation.43
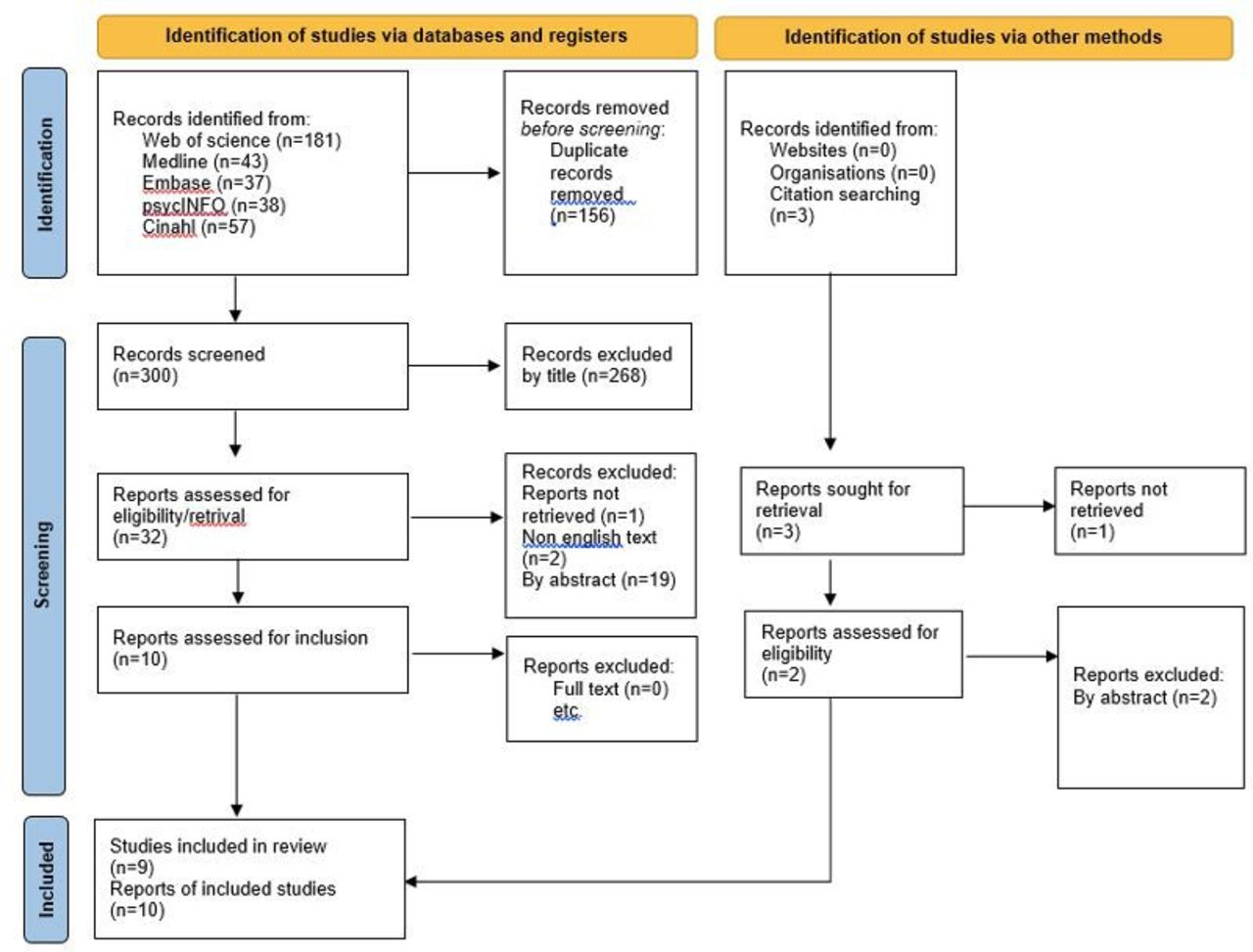
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 flow diagram.
Summary of characteristics and results from included quantitative studies
Summary of characteristics and results from included qualitative studies
One study was based in Australia42 and one in Turkey.34 The remainder were from the USA. In all studies the support group attendees were predominantly male (range 53%–91%). The support groups varied considerably in terms of attendee age, format and frequency (table 4).
Assessment of heterogeneity of support group attendees, format and frequency
Four papers34–37 contributed to the quantitative synthesis and were used in the meta-analysis for mental well-being (figure 2). Three of the four reported the mean value of age of attendees but one37 reported only a range. We contacted the authors for this information, but the raw data was no longer available.

{kind=link}
{kind=link}
Effect of ICD support groups on mental well-being. Forest plot for change in measure of mental well-being in patients with ICD attending a support group compared to usual care. CI, confidence interval.
Seven papers37–43 contributed to the qualitative synthesis. The data from the two mixed-methods studies were extracted and analysed as separate quantitative and qualitative data because quality assessment indicated the rationale for, and integration of, mixed methodology was poor as indicated by the MMAT (table 5). Table 5 shows how each study was appraised using the relevant questions to the category of study. Higher quality is indicated by higher proportion of positive responses to the questions. Overall, the more recent qualitative studies were of better quality than those published prior to 2000. Quantitative studies included in our meta-analysis had satisfactory quality, answering ‘yes’ to six out of seven questions.
Quality assessment using the Mixed-Methods Appraisal Tool
Integrated synthesis of quantitative and qualitative data are shown in table 6, where priority was given to studies with better quality ratings as determined by the MMAT (table 5).
Integrated synthesis of outcomes from ICD support groups
Quantitative analysis
Anxiety and depression
Three studies34 36 37 measured anxiety using validated instruments: State Trait Anxiety Inventory, Visual Analogue Scale-Anxiety (VAS-A) and FSAS. No quantitative data on depression was found. Only two studies34 37 measured the effect of support groups on anxiety over time; neither demonstrated a significant difference between support group attendees and non-attendees. Anxiety measured by the FSAS decreases over time in all groups.34 There was an increase in anxiety over time measured by the VAS-A, but no change in state anxiety.37
Support group attendees tended to be more anxious than non-attendees in observational studies.36 37 Attendees had significantly higher trait anxiety than non-attendees,36 although this was not significant for state anxiety.37
Quality of life
QoL was measured in two quantitative studies using the SF-3634 and QLI.35 Neither study recorded a significant difference in overall summary scores between support group attendees and non-attendees. There was significant improvement in specific subscales of the SF-36 (social functioning, role-physical, mental health, vitality and bodily pain) in support group attendees.34 Age and frequency of shocks were not related to QLI, however, greater comorbidity was found to correlate with reduced QoL.35
Social support
Social support was not identified as an outcome a priori for this review but was measured in three quantitative studies34 36 37 and was seen in the qualitative data; it was therefore included in the analysis to assess whether this contributes to the benefit of support groups.
Social support was measured using Saracon’s 6-item Social Support questionnaire,36 in sub-dimensions of the Medical Outcomes Study survey37 and SF-36.34 Support group attendance was associated with lower satisfaction with social support.36 However, a descriptive study found support group attendees experienced a higher level and value of support than non-attendees.35 There was no difference between groups in social functioning,34 37 where social functioning increased over time in both groups in an RCT.34
Effect of support groups on mental well-being
The effect of support groups on mental well-being was examined by normalising anxiety and QoL outcomes to the average control value (Fig. 2). The absolute data used in this meta-analysis are shown in Table 7. The standardised mean difference between intervention and control groups was 0.02 (95% CI −0.2 to 0.23). The support group attendees scores were not significantly higher than the control group average, z=0.16, p=0.87, indicating that attending support groups had no significant effect on mental well-being for patients with ICDs.
Quantitative data included in analysis
Qualitative analysis
Anxiety and depression
Patients reported that fear of death and of ICD shocks were the source of their anxiety.37 39–41 43
Knowing a stick of dynamite may go off at anytime and you have little warning, is a head game you are invited to participate in each morning when you wake up. (39, p161)
Attending a support group helped them to control their fear and anxiety through knowledge acquisition and decision-making skills, including making contingency plans.39 Patients also felt that positive role modelling and sharing of experiences within the group helped to manage depression.40 41
I need to turn to a source where I find comments, questions, fears, joys, whatever, also shared by me, that indicate I’m normal to this select group. (41, p253)
Patients experienced dependency and low self-esteem post implant,37 affecting relationships43 and preventing acceptance of their ICD.41 Encouragement from other group members to resume normal life activities helped patients manage their depression.37 43
Quality of life
Patients found that the support group helped them find ways to live with their ICD and deal with their limitations.39 40 Attending the group improved their knowledge and understanding of the device,39–42 which in turn led to a return to ‘normal’ life and activities.37 43
Social support
Patient support groups provide a social setting which allow new friendships to form.40 42 Patients reported difficulties with existing support as family and friends do not understand their experiences.41 43 Social bonding in the support group provides a setting for humour regarding ICDs,39 that was found to facilitate healing and coping.40
There were comical things that happened, one guy was holding his dog when it [ICD] went off and for a year the dog wouldn’t go near him … we had a lot of laughs in there. (40, p92)
Online support groups also provided an opportunity to benefit from this friendship.39
Benefits and challenges of attending support groups
Two sub-themes were identified: sharing experiences and support group format.
Sharing experiences
The opportunity to share and compare experiences of life with an ICD is a key perceived benefit of attending a patient support group.39 40 42 Hearing that others felt the same about their life with an ICD provided validation of their own feelings,40 which in turn facilitated healing and acceptance.42 Attending support groups also provided reassurance and promoted acceptance of their ICD by seeing others lead a ‘normal’ life and coping with the uncertainty created by their heart condition and device.39–41 43 Information gained from fellow ICD recipients was more credible than that from healthcare providers, who can talk theory but not from experience.
After hours of bombarding my HCP with questions, you feel something missing; they know what you have, but they are just not going through it themselves; you need people that you can relate to. (39, p162)
Support group format
There was considerable variation in meeting frequency between the included studies (table 4), and patients reported a preference for at least quarterly meetings.42 All the in-person support groups were facilitated by HCPs—most often a specialist nurse—and expert speakers to provide education.36 38 42 43 Not all studies commented on the role of HCPs; only Dickerson et al reported the presence of an HCP at in-person meetings as being essential.40
Williams et al reported that travel time from rural locations was a major barrier to group attendance, while others did not attend as they did not feel in need of support, did not want to be reminded about their ICD, or perceived that they did not fit in the group due to age or sex.42 Serber et al initiated live streaming of in-person group meetings over the internet to address the barrier of attending due to accessibility; in-person attendees found this acceptable, however, the experience of remote attendance was not investigated.38 Patients reported that the benefits of online support were ease of access,39 and timing, as online support was available day and night.41
Discussion
The findings from our meta-analysis suggest that support groups have no significant effect on objectively measured mental well-being. However, the qualitative analysis suggests that patients do perceive a benefit from support group attendance in terms of managing fears through positive role modelling and accepting life with their ICD. This may be because mental well-being is more than the absence of mental illness, and our meta-analysis predominantly included measures of anxiety.
The present study found that self-selected attendees have higher trait anxiety and lower social support than non-attendees36 with increased anxiety over time37 possibly due to facing an issue previously avoided. Some patients preferred not to attend support groups as they did not want to be reminded about their ICD.42 In contrast to existing literature our study found no relationship between shock frequency and QoL, but patients did report that fear of shocks is the source of their anxiety. Support groups help to relieve this anxiety by fostering a sense of belonging41 and providing reassurance that there is life after ICD shocks.40 Positive role modelling from other attendees and sharing stories with other patients also relieves fear and anxiety in a way HCPs cannot.40 41
The lack of a significant effect on mental well-being demonstrated by the quantitative data may be attributable to the fact that the majority of included quantitative studies were observational with self-selected support group attendees, while a usual care comparison group may include patients with lower existing anxiety.36 However, the single RCT34 also did not show reduction in anxiety over time in support group attendees. An alternative explanation is the use of general anxiety and QoL measures that may not be sensitive to the specific fears experienced by ICD patients. The use of different outcome measures to estimate mental well-being is a shortcoming of our meta-analysis, however, it highlights the lack of good quality quantitative data in this important topic.
The present study shows that sharing experiences is key to facilitating device acceptance, a consistent finding for in-person and online support groups. Gaining information is also an important benefit of support groups, although patients reported that they found information and understanding from fellow attendees more credible than that from HCPs.39 41 42 This suggests that support groups should prioritise patient-to-patient communication. Despite this finding, all in-person support groups used a HCP to provide information and education. The online support offered in these studies was in the form of web-based written forums, with the exception of one web-cast group meeting.38 The increased availability and use of video-conferencing technology since the COVID-19 pandemic has made remote meetings a viable option and provides the convenience of online meetings alongside the opportunity for patient-to-patient communication and HCP involvement. None of the reported studies conducted a comparison of in-person and online support. Future research could help guide the most efficient format for support groups, including use of HCP time and personnel and the delivery of online and in-person groups.
Most included studies were based in the USA, and it is striking that no Western European studies were found. A recent UK study44 commented that while there is interest in patient support groups, there are not many. Perhaps even more important is the fact that ICD implant rates in the USA have historically been 4–5 times higher than in Europe.45 This highlights the need for further research in, and implementation of, patient support groups in Europe.
Another area for future research is comparing the support needs of patients with ICDs for primary or secondary prevention of SCD. No data were available regarding participant ICD implant indications, however, the dates of most included studies signifies participants will have had ICDs for secondary prevention of SCD, whereas most implants are now primary prevention.46 Our data showed that patients have a fear of death and of shocks; as survivors of cardiac arrest, secondary prevention patients will have had different experiences leading to these fears compared with patients with ICDs implanted for primary prevention. As sharing experiences appears to be an important benefit of support groups, future research could explore whether primary and secondary prevention patients have sufficiently similar experiences to support each other.
Our mixed-methods systematic review has strengths and limitations. It was inclusive in terms of design, outcomes and publication status and dates. The screening and quality assessment was robust, with clear a priori definitions of the intervention of interest and outcomes provided. There was limited opportunity for meta-analysis from the quantitative data as there was no quantitative data regarding depression, device acceptance, or group format, despite these being important themes identified in the qualitative analysis.
In conclusion, this first mixed-methods systematic review and meta-analysis shows that while there is currently no quantitative evidence that ICD support groups have a significant beneficial effect on mental well-being, qualitative data show that patient support groups are perceived as beneficial by attendees. This suggests that we need other quantitative measures to assess the benefits of support groups for mental well-being. Attendees value the opportunity to share their experiences which helps them to accept their new life with an ICD. Further research is recommended into the optimal format of support groups, level of involvement of HCPs, and whether primary and secondary prevention ICD patients have different supportive needs.
Data availability statement
Data sharing not applicable as no datasets generated and/or analysed for this study.
Ethics statements
Patient consent for publication
References
Footnotes
Contributors KHS, PJP and MA designed the study and took overall responsibility for its content; KHS, PAC and MA assessed study eligibility; KHS, PAC and KC assessed study quality; KHS, HD and MA analysed the data; KHS, HD, MA and KC contributed to the data interpretation; all authors contributed to the drafting of the manuscript and approved the final version to be published. KHS acts as guarantor for the study.
Funding This review was funded by the National School of Healthcare Science under its Higher Specialist Scientist Training Programme; KHS is a funded Higher Specialist Scientist Trainee. The funder had no role in the collection, analysis and interpretation of data; the funder had no role in the writing of and decision to publish this review. The views expressed are those of the author(s) and not necessarily those of the National School of Healthcare Science.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.