Article Text

Abstract
Background Increase in left ventricular filling pressure (FP) and diastolic dysfunction are established consequences of progressive aortic stenosis (AS). However, the impact of elevated FP as detected by pretranscatheter aortic valve replacement (TAVR) echocardiogram on long-term outcomes after TAVR remains unclear.
Objective To understand the impact of elevated FP in patients with severe AS who undergo TAVR.
Methods This was a retrospective study of all patients who underwent TAVR between 1 January 2014 and 31 December 2017. The presence of elevated FP was determined in accordance with the latest guidelines using the last available comprehensive echocardiogram prior to TAVR.
Results Of 983 patients who were included in our study, 422 patients (43%) were found to have elevated FP and 561 patients (57%) had normal FP prior to TAVR. Patients with elevated FP had a mean age of 81.2±8.6 years and were more likely to be males (62%), diabetic (41% vs 35%, p=0.046), and have a higher prevalence of atrial fibrillation (Afib) (53% vs 39%, p<0.001). The 5-year all-cause mortality after TAVR was significantly higher in patients with elevated FP when compared with patients with normal FP (32% vs 24%, p=0.006). The presence of elevated FP, history of Afib and prior PCI emerged as independent predictors of long-term mortality after TAVR.
Conclusion Elevated FP is associated with increased mortality in patients with severe AS undergoing TAVR. Assessment of FP should be incorporated into the risk assessment of AS patients to identify those who may benefit from early intervention.
- heart valve diseases
- transcatheter aortic valve replacement
- heart failure, diastolic
Data availability statement
No data are available. Due to the patient specific nature of our data, sharing it with individuals outside of this research project will not be possible.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Two-thirds of all patients with aortic stenosis (AS) who undergo transcatheter aortic valve replacement (TAVR) have coexisting diastolic dysfunction (DD) and baseline DD is a predictor of clinical outcomes in patients undergoing TAVR.
WHAT THIS STUDY ADDS
Our study shows that in patients with severe AS, the presence of coexisting elevated filling pressure (FP) is associated with worse long-term outcomes after TAVR compared with those with normal FP, irrespective of left ventricular (LV) dysfunction.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE AND/OR POLICY
In patients with severe AS, assessment of LV FP can help in identifying those who could benefit from early intervention and have better long-term outcomes after TAVR.
Introduction
Aortic stenosis (AS) is the most prevalent valvular heart disease across the world and affects more than a million people in the USA. Left ventricular (LV) hypertrophy, scarring and change in the cardiac skeleton are undesirable yet expected consequences of progressive aortic valve stenosis. These changes subsequently lead to a decrease in LV compliance and a compensatory increase in LV filling pressure (FP). Elevated FP is a marker of diastolic dysfunction (DD) and has been associated with poor outcomes in patients with AS.1 Elevated FP may also precede reduction in LV systolic function in patients with AS, thereby acting as an early sign of myocardial dysfunction.2 3
Prior studies have revealed that about two-thirds of all patients with AS who undergo transcatheter aortic valve replacement (TAVR) have coexisting DD and that baseline DD is a predictor of clinical outcomes in patients undergoing TAVR.4 5 However, most studies have only examined outcomes up to a year after TAVR. Since TAVR has now been widely accepted as the standard of care for all patients with severe AS,6–9 there is expected to be an increase in the prevalence of patients who undergo TAVR in the near future. So, understanding the effect of baseline LV pressure changes on long-term outcomes after TAVR is important to understand its impact on reversing LV pressure changes and to expand its application. Furthermore, patients with atrial fibrillation (Afib) are an important cohort who have traditionally been excluded from most studies assessing the impact of DD in patients with severe AS and so they are not depictive of real-world settings, where around 40% of these patients have coexisting Afib.10 11 Therefore, we aimed to evaluate the impact of elevated FP in a more inclusive cohort of AS patients to understand their 5-year outcomes post-TAVR.
Methods
All patients who underwent TAVR between 1 January 2014 and 31 December 2017, were included. Patients with a history of surgical aortic valve replacement, no AS (who underwent TAVR for other indications), patients with incomplete echocardiographic values, those who underwent TAVR via non-transfemoral access, patients with mitral stenosis and those with severe mitral regurgitation were excluded. Patients were then categorised into two groups depending on the presence or absence of elevated FP as per the latest guidelines.12
Assessment of FP: All patients had a comprehensive echocardiogram performed before TAVR and the most recent comprehensive echocardiogram before TAVR was used to collect the variables required for our study. All echocardiograms were performed at the Cleveland Clinic by experienced technicians as per standardised protocols and were averaged over at least three consecutive cardiac cycles. Patients were defined as having elevated FP if E/A was ≥2 or if E/A was between 0.8 and 2 and if they qualified two of the following three criteria: (1) average E/e’>14, (2) tricuspid regurgitation (TR) velocity >2.8 m/s or (3) left atrial (LA) volume index >34 mL/m2. Patients who did not fulfil this criterion and those who had E/A≤0.8 were classified as having normal FP.
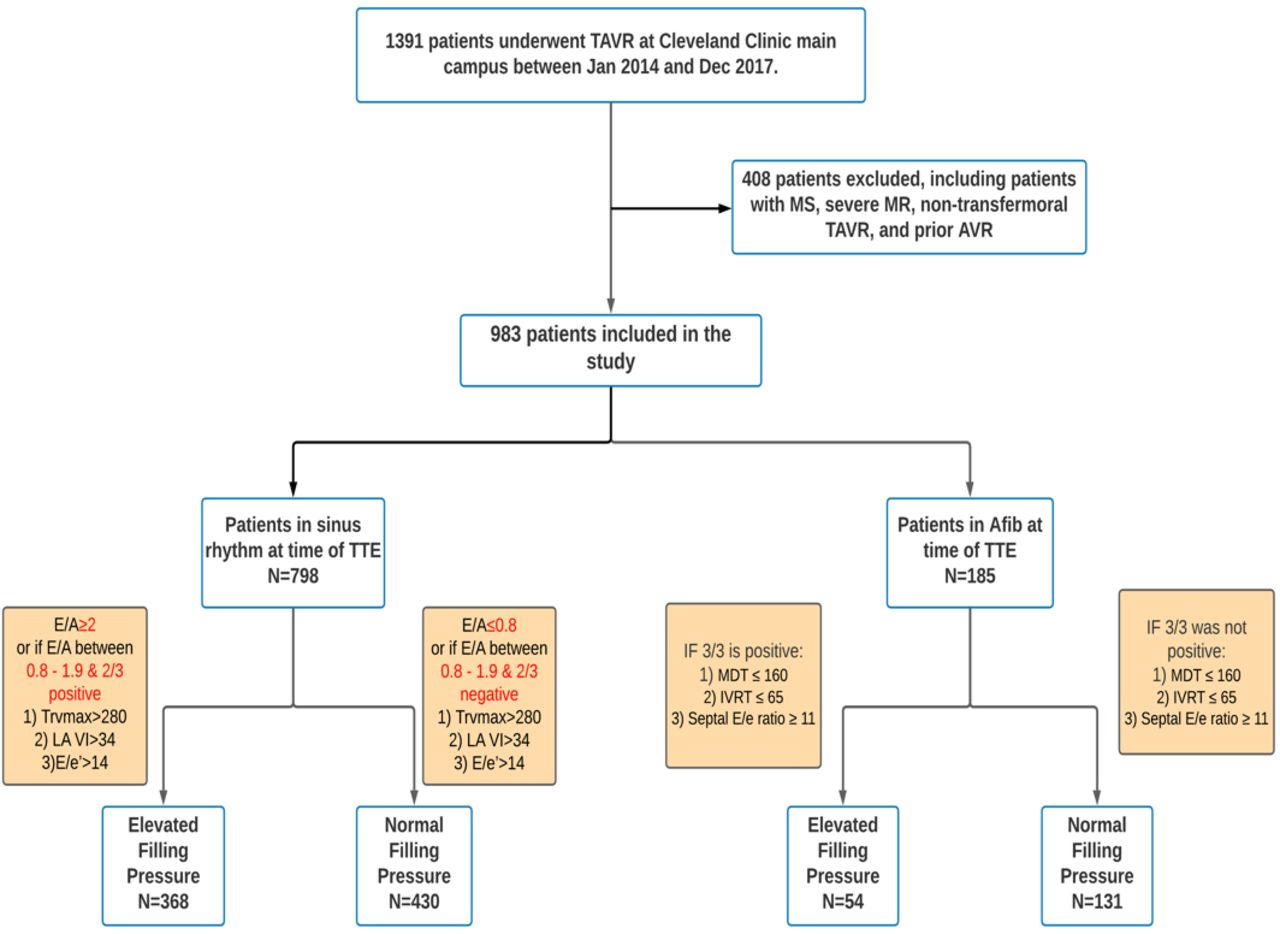
Patients with a history of Afib were also included in our study. If these patients were not in Afib at the time of echocardiogram (paroxysmal Afib) and E/A was available, the above-mentioned criterion was applied to them. For patients who were in Afib at the time of echocardiogram, we used a combination of mitral deceleration time (MDT), isovolumetric relaxation time (IVRT) and Septal E/e’ ratio to determine if they had elevated FP or not as per the current guidelines and pre-existing evidence.12–14 These patients were classified as having elevated FP only if they qualified all three of the following criteria (1) MDT ≤160 ms, (2) IVRT ≤65 ms and (3) septal E/e ratio ≥11 cm/s. The study protocol is represented graphically in figure 1.
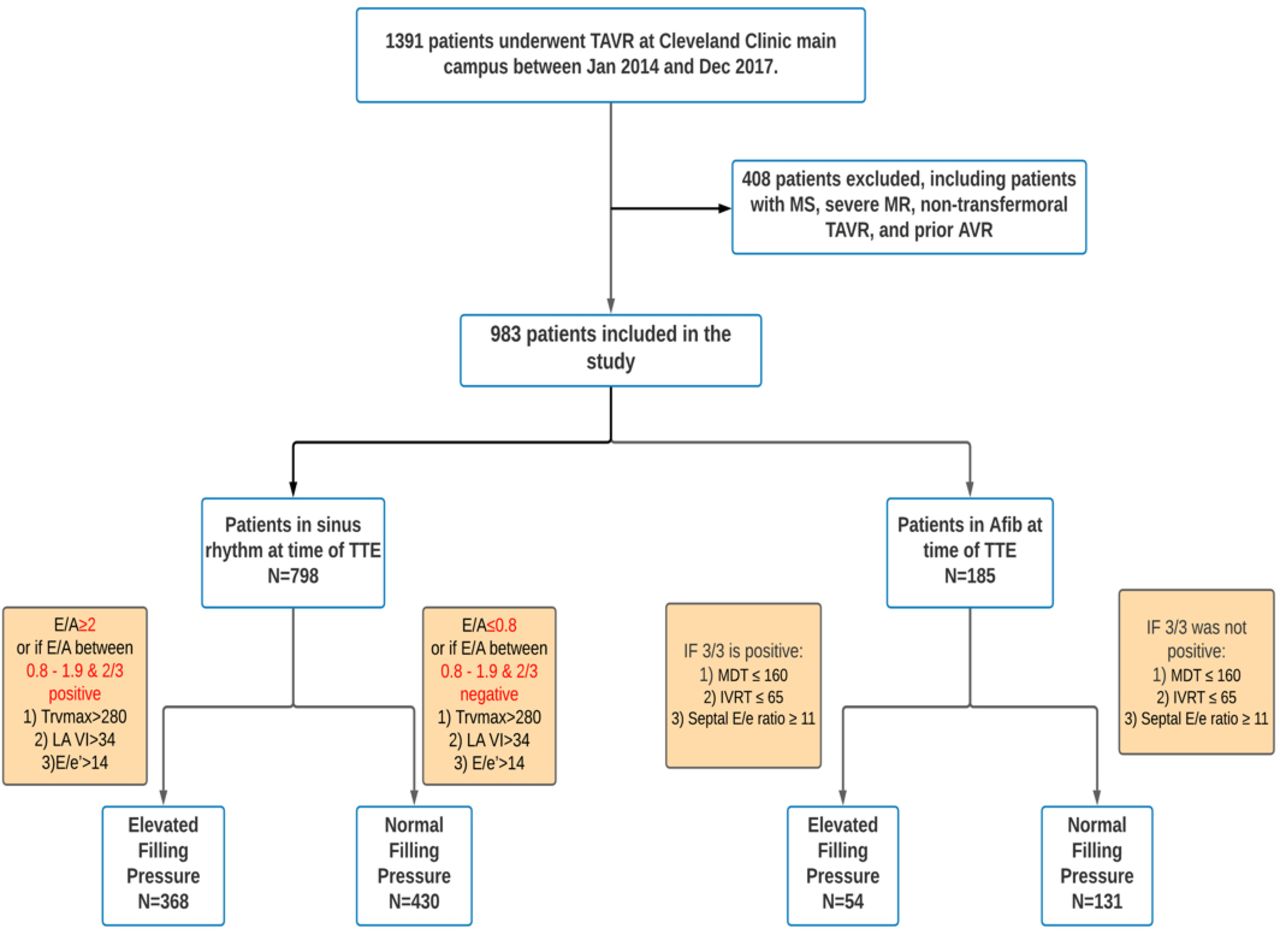
Study flowsheet. AVR, aortic valve replacement; IVRT, isovolumetric relaxation time; MDT, mitral deceleration time; TAVR, transcatheter aortic valve replacement; TTE, transthoracic echocardiogram.
The primary endpoint of our study was 1-year and 5-year all-cause mortality. Secondary endpoints included hospitalisation for heart failure, stroke or TIA, postprocedure permanent pacemaker or defibrillation, conversion to open surgery and valve dysfunction.
Statistical analysis
Continuous variables are reported as mean±SD if normally distributed or median and IQR if non-normal. Categorical variables are reported as frequency and percentage. To compare continuous variables between the two groups, independent samples t-tests were used for normally distributed variables and Wilcoxon rank-sum test for non-normal distribution. For categorical variables, differences between the two groups were studied using Pearson χ2 test. Univariable and multivariable logistic regression analysis were used to predict factors associated with elevated FP and poor outcomes.
Only significant variables in univariable analysis were selected in the multivariable model for overall survival and ORs with 95% CIs were calculated. Cox proportional hazards analysis was done to evaluate the prognostic values of the predictors. Backward stepwise logistic regression was done to evaluate for predictors of elevated FP. Kaplan-Meier survival curves along with log-rank p values were calculated for survival analysis. A p<0.05 was used to for statistical significance. Data analysis was conducted using STATA statistics/Data analysis software (V.16.1; StataCorp), and Rstudio (V.1.4.1717 2009–2021 RStudio, Boston, Massachusetts, USA). Finally, due to the design and retrospective nature of our study, it was not possible to involve patients or the public in the design, or conduct, or reporting, or dissemination plans of our research.
Results
Patient population
There was a total of 1391 patients who underwent TAVR at our hospital during the study frame, out of which, 408 patients were excluded from our study due to incomplete echocardiographic results (n=21), presence of mitral stenosis(n=111), presence of severe mitral regurgitation (n=18), history of prior AV replacement (110), patients with no AS (n=1) and patients with non-transfemoral access (n=147). Of the remaining 983 patients that were included in our study, 422 patients (43%) were identified as having an elevated LV FP prior to TAVR and 561 patients (57%) had normal FP prior to TAVR.
Baseline characteristics
The mean age of our cohort was 81.27±8.66 years, 59% were males and 94% of patients belonged to the Caucasian race. Baseline characteristics between both groups are presented in table 1. Mean age was similar between both groups (81.47 vs 81.13, p=0.542), both groups consisted predominantly of men (62% vs 57%), and there was no significant difference in the baseline body mass index between both groups (28.76 vs 29.23, p=0.271). The elevated FP group had higher prevalence of Diabetes (41% vs 35%, p=0.046), Afib (53% vs 39%, p<0.001) and history of prior CABG (32% vs 26%, p=0.041).
Comparison of baseline characteristics and echocardiographic variables between patients with and without elevated FP
Echocardiographic characteristics
Compared with the group with normal FP, the elevated FP group had higher Left Ventricular End Diastolic Volume Index, (57.49 vs 51.69, p=0.003), higher mean right ventricular systolic pressure (49.89 vs 37.59, p<0.001), lower aortic valve area (0.68 vs 0.71, p=0.026), lower AS peak gradient (69.64 vs 74.93, p<0.001) and lower left ventricular outflow tract stroke volume (67.20 vs 71.67, p<0.001). The mean LVEF was 52.13 in the elevated FP group whereas 57.38 in the normal FP group (p<0.001).
FP variables
Among the variables used to classify FP, the elevated FP group had significantly higher mitral E velocity (127.16 vs 93.47, p<0.001), mitral E/A ratio (7.73 vs 0.74, p=0.023), septal E/e’ (24.22 vs 17.51, p<0.001) and lateral E/e’ ratio (18.92 vs 13.64, p<0.001) compared with the normal FP group. The LA volume index and TR velocity were also significantly elevated in the elevated FP group (p<0.001). MDT and IVRT were significantly lower in the elevated FP group when compared with the normal FP group (p<0.001), (table 2).
Comparison of echocardiographic variables used to assess FP
Univariate and multivariate analysis
Stepwise logistic regression revealed that mitral E/A ratio was associated with the highest ability to predict elevated FP (OR 588.231, 95% CI1.032 to 1.099). Mitral E velocity and TR velocity were also associated with elevated FP. Univariate analysis by cox regression revealed that comorbidities such as diabetes, Afib, prior PCI, presence of pacemaker or defibrillator, and elevated FP were associated with significantly worse outcomes (table 3). On including the significant variables in our multivariate analysis model, we found that elevated FP remained an independent predictor of poor outcomes after TAVR (HR 1.303, 95% CI 1.025 to 1.657). In addition, the presence of prior PCI (HR1.359, 95% CI 1.064 to 1.736) and a history of Afib (HR 1.370, 95% CI 1.070 to 1.754) were also found to be associated with poor outcomes after TAVR (table 4). On adjusting the model for the presence of Afib, the results remained the same (online supplemental table 1).
Supplemental material
Univariate and multivariable analysis of overall survival by Cox regression
Stepwise logistic regression showing factors associated with elevated filling pressure
Outcomes
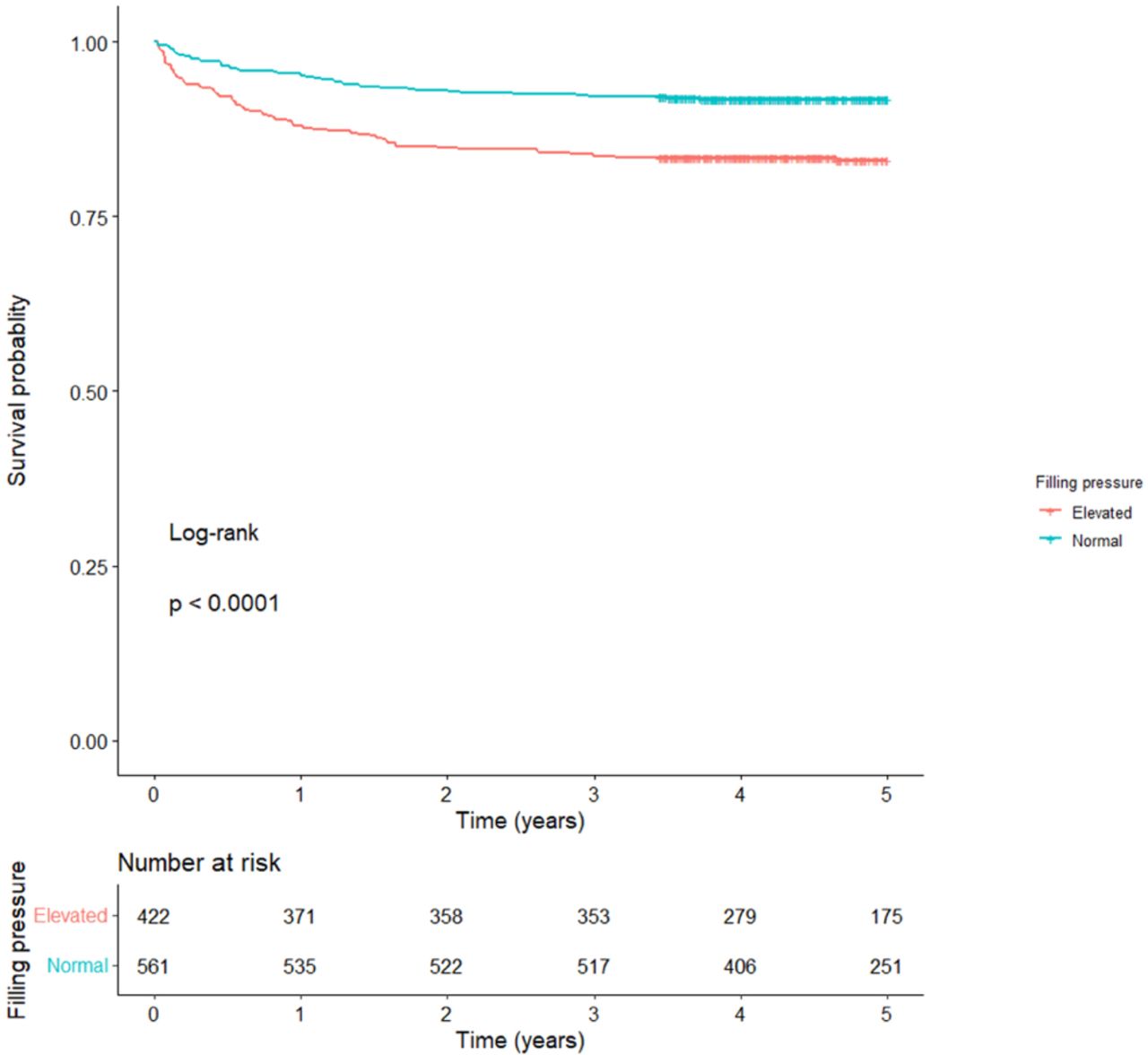
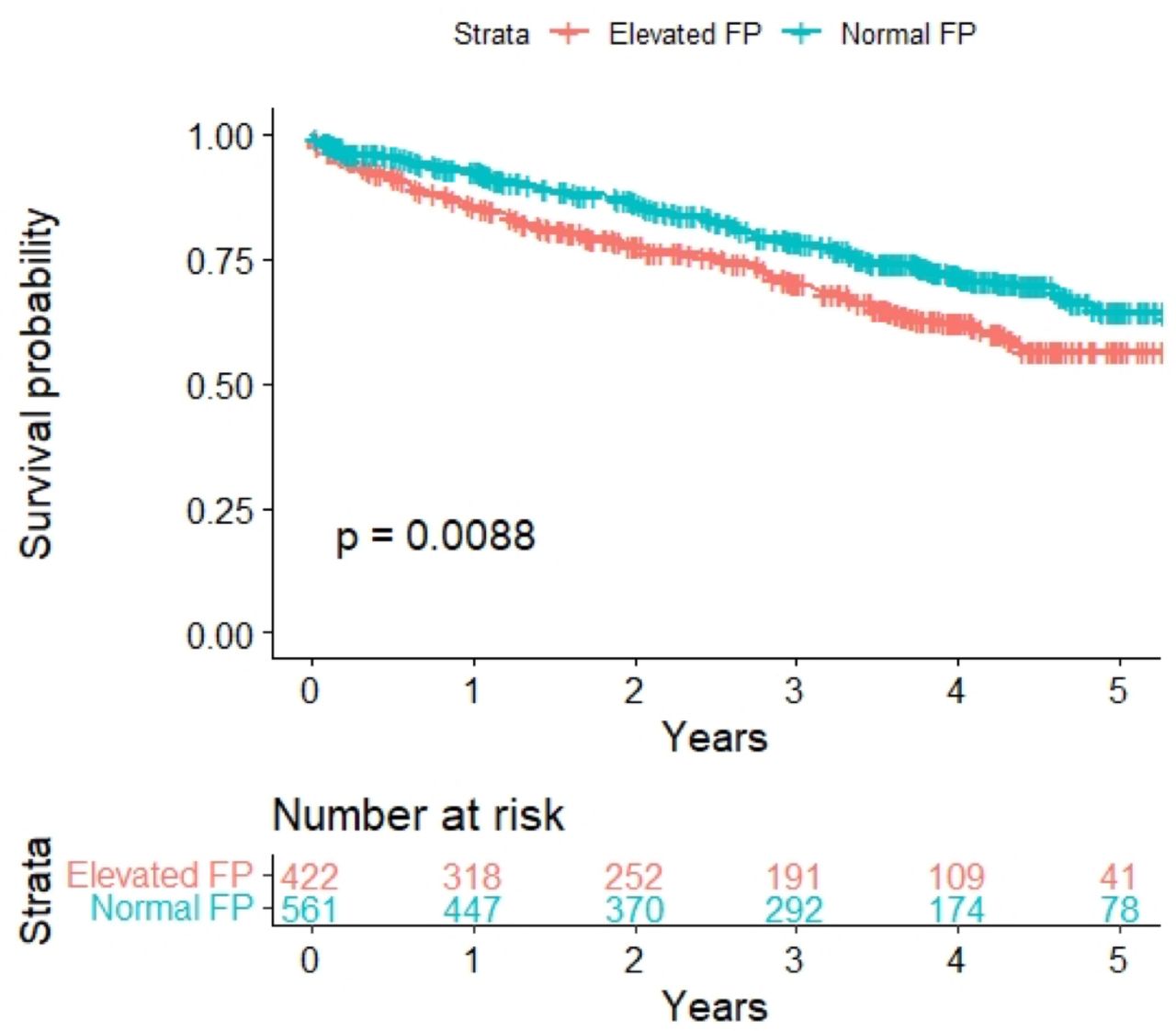
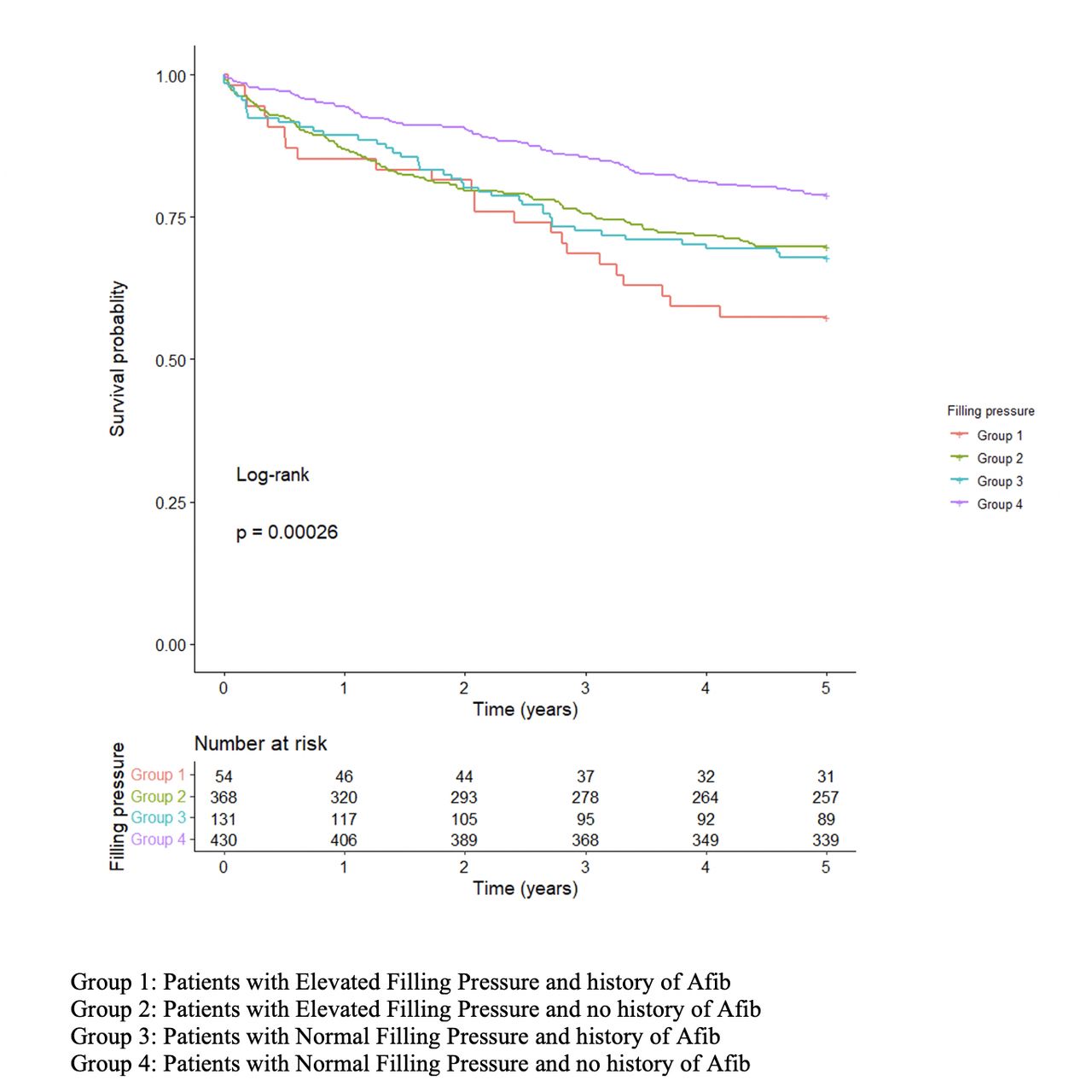
The difference in clinical outcomes between the two groups is described in table 5. The all-cause mortality was significantly worse for patients with elevated FP at 1 year (25% vs 20%) and 5 years (90% vs 24%, p=0.006)(figure 2). when compared with patients with normal FP. Post-TAVR aortic regurgitation at 30 days was similar between both groups (17% vs 19%, p=0.336) and so was the incidence of device implantation after TAVR (17% vs 16%, p=0.623). There were significantly higher readmissions for heart failure or valve-related complications in the elevated FP pressure group at 1 and 5 years (12% vs 5%, p<0.001% and 17% vs 8%, p<0.001)(figure 3). Patients with the combination of elevated FP and history of Afib had the worst outcomes when compared with patients with normal FP±history of Afib (figure 4). In addition, comparison of outcomes between patient with and without elevated FP depending on ejection fraction also did not reveal any significant differences (figure 5).
Difference in clinical outcomes between patients with and without elevated left ventricular FPs

Survival analysis of patients with and without elevated FP. FP, filling pressure.
Km estimates for readmissions secondary to heart failure or valve related problem in patients with and without elevated FP. FP, filling pressure.

Survival analysis of patients with and without elevated filling pressure depending on the presence of history of Afib. Afib, atrial fibrillation.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Survival analysis of patients with and without elevated filling pressures depending on ejection fraction (A) KM graph of patients with elevated FP with or without reduced EF (B) KM graph of patients with normal FP with or without reduced EF.EF, ejection fraction; KM, Kaplan Meier; NFP, normal filing pressures; FP, filling pressure.
Discussion
In our study evaluating the impact of elevated LV FP on outcomes after TAVR, we found several key findings pertaining to the long-term care of patients with severe AS. Notably, we found that (1) more than 40% of all patients with severe AS who undergo TAVR have elevated FP, (2) Mitral E/A ratio had the highest likelihood of predicting elevated FP, (3) Patients with elevated FP have a worse post-TAVR course complicated by more frequent readmissions and increased mortality, which extends out to 5 years post-TAVR, (4) The combination of Afib and elevated FP was associated with the worst outcomes of all the group of patients, (5) Patients with elevated FP and preserved EF have equally worse outcomes as those with elevated FP and reduced EF and (6) Diabetes, Afib, Prior PCI and elevated FP emerged as independent markers of worse outcomes after TAVR.
To our knowledge, our study is the first to analyse clinical outcomes up to 5 years after TAVR in patients with severe AS and elevated FP (table 6). In patients with AS, the rise in LV FP is a compensatory response to the increase in LV outflow resistance caused by the stenosed valve15 16 and often represents the chronicity of the stenosis. More than 40% of the patients in our cohort had elevated FP, which is much higher than prior studies.5 This signifies that nearly half of all patients with severe AS could have advanced stages of DD and significant LV remodelling by the time of intervention. Though prior studies have shown that regression of myocardial hypertrophy and remodelling may happen in the following months to years after aortic valve replacement,15 17 the outcomes of patients with elevated FP prior to TAVR continues to remain worse even after several years postintervention compared with those who had normal FP and subtle LV remodelling prior to TAVR.
Comparison of prior studies that have evaluated outcomes of as patients with baseline diastolic dysfunction after TAVR
Current guidelines focus on symptoms and LV ejection fraction to determine the timing of intervention in patients with severe AS.18 In our study, patients with elevated FP had significantly worse outcomes regardless of ejection fraction, signifying the high-risk nature of this group. With advancements in procedural techniques and increased familiarity with the procedure, it may be more beneficial to develop an ‘inclusive criterion’ incorporating both diastolic and systolic elements to identify the group of patients with severe AS who may benefit from TAVR rather than adopting the conventional criteria of systolic dysfunction. Such a criterion could also help in targeting patients who may benefit from early intervention in the course of the disease and thus prevent LV remodelling. We also saw that in addition to elevated FP, the presence of coexisting comorbidities in the form of diabetes, Afib and prior PCI are independently associated with poor long-term outcomes after TAVR. Interestingly, the presence of dyslipidaemia and hypertension were associated with better long-term outcomes after TAVR. On closer inspection, we observed that around 79% of the patients in our cohort were on statins and 65% of patients were on ACE inhibitors (ACEI) or angiotensin receptor blockers. Prior studies have clearly established the protective role of statins and ACEI in patients with severe AS who undergo TAVR and we believe that the high prevalence of these medications in our cohort is the reason behind this association.19 20
Around 45% of patients in our study had a history of Afib, which is similar to the prevalence of Afib in patients with AS as seen in prior studies.21–23 LV remodelling and elevated FP from AS can in time lead to LA dilatation and atrial remodelling thereby precipitating Afib,24 25 which can lead to further morbidity and mortality. In the Cardiovascular Health Study by Rosenberg et al, 27% of patients with DD were found to have new-onset Afib.26 Afib has also been shown to be independently associated with poor outcomes after TAVR.23 In our study, the group of patients with coexisting elevated FP and Afib had the worst outcomes, consolidating the high-risk nature of this group. Early intervention of patients with AS and elevated FP could potentially help in reducing the incidence of Afib and thereby improve the outcomes of these patients. However, further randomised studies are needed to explore if such a decreased threshold in intervention translates to improved outcomes.
Limitations
The findings of our study should be interpreted in the context of the following limitations. First, this is a retrospective study and does accompany the limitations of such a study design. The echocardiographic variables were collected from previously recorded transthoracic echocardiograms (TTEs) and were not specifically done for this purpose. However, all our TAVR patients have a detailed TTE prior to the procedure which includes measurement of diastology and FP. Also, though we have drafted our study protocol from the latest diastology guidelines, identifying elevated FP in patients with Afib is an area of diminished clarity. With this in mind, we have used a rather stringent criteria incorporating three different variables, all of which have been independently shown to be predictive of elevated FP in patients with Afib. Therefore, such a criterion is more inclined to under-represent rather than over account for patients with elevated FP and so the results of our study should be generalisable.
Conclusion
Elevated LV filling is associated with significantly worse 5-year outcomes post-TAVR, regardless of ejection fraction. Patients with elevated FP are more likely to have a postdischarge course complicated by recurrent hospitalisations and increased mortality when compared with patients with normal FP. Early assessment of FP using echocardiographic variables should be incorporated into the routine care of patients with AS to identify this group of patients who may benefit from early intervention.
Data availability statement
No data are available. Due to the patient specific nature of our data, sharing it with individuals outside of this research project will not be possible.
Ethics statements
Patient consent for publication
Ethics approval
This research study was approved by the Cleveland Clinic Institutional Review Board.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @Hasanmehmoodlak, @GrantReedMD
Contributors RN and SK: concept, study design and guarantors for overall study. RN: manuscript drafting and editing; BV and RN: statistical analysis; SC, SK, BG, HML, JC: data gathering and manuscript editing; JY, RP, GWR, AK, SCH, SK: project overview, manuscript writing and editing.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.