Article Text

Abstract
Objective To assess whether hypertension is an independent risk factor for mortality among patients hospitalised with COVID-19, and to evaluate the impact of ACE inhibitor and angiotensin receptor blocker (ARB) use on mortality in patients with a background of hypertension.
Method This observational cohort study included all index hospitalisations with laboratory-proven COVID-19 aged ≥18 years across 21 Australian hospitals. Patients with suspected, but not laboratory-proven COVID-19, were excluded. Registry data were analysed for in-hospital mortality in patients with comorbidities including hypertension, and baseline treatment with ACE inhibitors or ARBs.
Results 546 consecutive patients (62.9±19.8 years old, 51.8% male) hospitalised with COVID-19 were enrolled. In the multivariable model, significant predictors of mortality were age (adjusted OR (aOR) 1.09, 95% CI 1.07 to 1.12, p<0.001), heart failure or cardiomyopathy (aOR 2.71, 95% CI 1.13 to 6.53, p=0.026), chronic kidney disease (aOR 2.33, 95% CI 1.02 to 5.32, p=0.044) and chronic obstructive pulmonary disease (aOR 2.27, 95% CI 1.06 to 4.85, p=0.035). Hypertension was the most prevalent comorbidity (49.5%) but was not independently associated with increased mortality (aOR 0.92, 95% CI 0.48 to 1.77, p=0.81). Among patients with hypertension, ACE inhibitor (aOR 1.37, 95% CI 0.61 to 3.08, p=0.61) and ARB (aOR 0.64, 95% CI 0.27 to 1.49, p=0.30) use was not associated with mortality.
Conclusions In patients hospitalised with COVID-19, pre-existing hypertension was the most prevalent comorbidity but was not independently associated with mortality. Similarly, the baseline use of ACE inhibitors or ARBs had no independent association with in-hospital mortality.
- hypertension
- COVID-19
- pharmacology
- clinical
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Conflicting data have been presented on the impact of hypertension, ACE inhibitors and angiotensin receptor blockers (ARBs) on mortality in hospitalised patients with COVID-19. There is a dearth of literature exploring these outcomes within both a generalisable population and a healthcare system that have not been overwhelmed by the pandemic.
What does this study add?
In this multicentre analysis of 21 Australian hospitals, neither hypertension nor treatment with ACE inhibitors or ARBs was independently associated with mortality. By comparison, factors commonly associated with hypertension such as increasing age, heart failure or cardiomyopathy, chronic kidney disease and chronic obstructive pulmonary disease were predictors of mortality.
How might this impact on clinical practice?
Clinicians should be aware that among patients hospitalised with COVID-19, pre-existing hypertension and treatment with ACE inhibitors or ARBs do not portend an increased risk of mortality.
Background
By the end of January 2021, SARS-CoV-2, the causative virus of COVID-19, had infected over 100 million and killed over 2 million people internationally.1 Hypertension has been recognised as the most common comorbidity among patients hospitalised with COVID-19.2–4 However, it remains unclear whether hypertension is an independent risk factor for mortality or whether the presence of hypertension is a marker of other factors that confer an adverse prognosis such as advanced age, coronary artery disease, heart failure and renal disease. This has important implications for identifying patients at high risk of adverse outcomes and for prioritising the management of comorbidities in patients with and at risk of COVID-19. The primary aim of this study was therefore to assess whether hypertension is independently linked with increased mortality from COVID-19.
Additionally, there has been conjecture about the effects of ACE inhibitors and angiotensin receptor blockers (ARBs) on COVID-19 prognosis in light of the fact that the virus responsible for COVID-19, SARS-CoV-2, binds to the ACE2 receptor in order to enter host cells.5 With the potential upregulation of ACE2, secondary to ACE inhibitor and ARB use,6 7 there exists a possible risk of increased viral entry into host cells. However, on the other hand, previous animal studies have suggested that ACE2 may have protective effects against acute respiratory distress syndrome.8 Initial observational data on this matter have been conflicting.9 10 Therefore, the secondary aim of this study was to assess the impact of ACE inhibitors and ARBs on mortality in patients with a background of hypertension admitted to hospital with COVID-19.
Australia provides a unique context to investigate these questions. Healthcare resources have been overwhelmed internationally,11–13 requiring stricter rationalisation of access to intensive care units (ICUs) in many regions and rapid construction of new hospitals in some settings. The extent to which this pandemic context has confounded the results of international clinical studies investigating COVID-19 outcomes is unknown. Australia has maintained control of COVID-19 case numbers such that hospital systems been able to maintain a high level of supportive care to all patients as required. The current manuscript presents analysis of the Australian Cardiovascular COVID-19 (AUS-COVID) Registry, which is the largest Australian multicentre COVID-19 cardiovascular registry of hospitalised patients.
Methods
Trial oversight
The AUS-COVID Registry is a collaboration between 21 hospitals across Australia and was designed and overseen by a steering committee. The protocol and case report form are available online at https://wwwaus-covidcom. The registry was prospectively registered with the Australian and New Zealand Clinical Trials Registry (ACTRN12620000486921).
Patients
The registry included all index hospitalisations of consecutive patients aged 18 years or older with laboratory-proven SARS-CoV-2 infection entered in the AUS-COVID Registry by 22 January 2021. Patients with suspected but not laboratory-proven SARS-CoV-2 infection were excluded. Patients were also excluded if their medical or medication history was not available or if they were transferred to another hospital in which case mortality outcomes were not available. Given that many of the included sites were major tertiary centres, patients transferred from another hospital were excluded to avoid recruitment bias.
Outcomes
The registry captured over 150 datapoints extracted from the patient’s medical record covering demographics, baseline comorbidities, baseline medications, laboratory results, treatment and outcomes. Potential variables for inclusion were age, sex, hypertension, coronary artery disease, heart failure or cardiomyopathy, atrial fibrillation or flutter, severe valvular disease, stroke or transient ischaemic attack (TIA), hypercholesterolaemia, diabetes mellitus, peripheral arterial disease, current or recent smoker (<1 year), chronic obstructive pulmonary disease (COPD), asthma and chronic kidney disease (estimated glomerular filtration rate (eGFR) <60 mL/min/1.73 m2). Coronary artery disease was defined as the presence of prior myocardial infarction, percutaneous coronary intervention, coronary artery bypass grafting, angina or >50% stenosis of an epicardial vessel on CT coronary angiogram or invasive angiography based on available data on the electronic medical record. Other comorbidities were based on the documented medical history available from electronic and paper medical records.
Statistical analysis
Continuous variables were reported as mean (SD). Categorical variables were presented as proportions. Independent samples t-test was used to compare between group differences for normally distributed continuous variables. Pearson’s Χ2 test and Fisher’s exact test were used to compare proportions between groups for categorical variables when expected cell sizes were ≥5 and <5, respectively. Multivariable binary logistic regression was performed to calculate adjusted ORs (aORs) for mortality. Potential variables were included in the multivariable model if they had a p value of <0.1 in the univariable model. A secondary analysis was performed in patients with pre-existing hypertension, with the use of an ACE inhibitor or ARB on admission as additional variables. Statistical analysis was performed using IBM SPSS Statistics Subscription (V.1.0.0.1508). Results were considered statistically significant if the two-sided p value was <0.05.
Patient and public involvement
Patients or the public were not involved in the design, or conduct, or reporting, or dissemination plans of our research.
Results
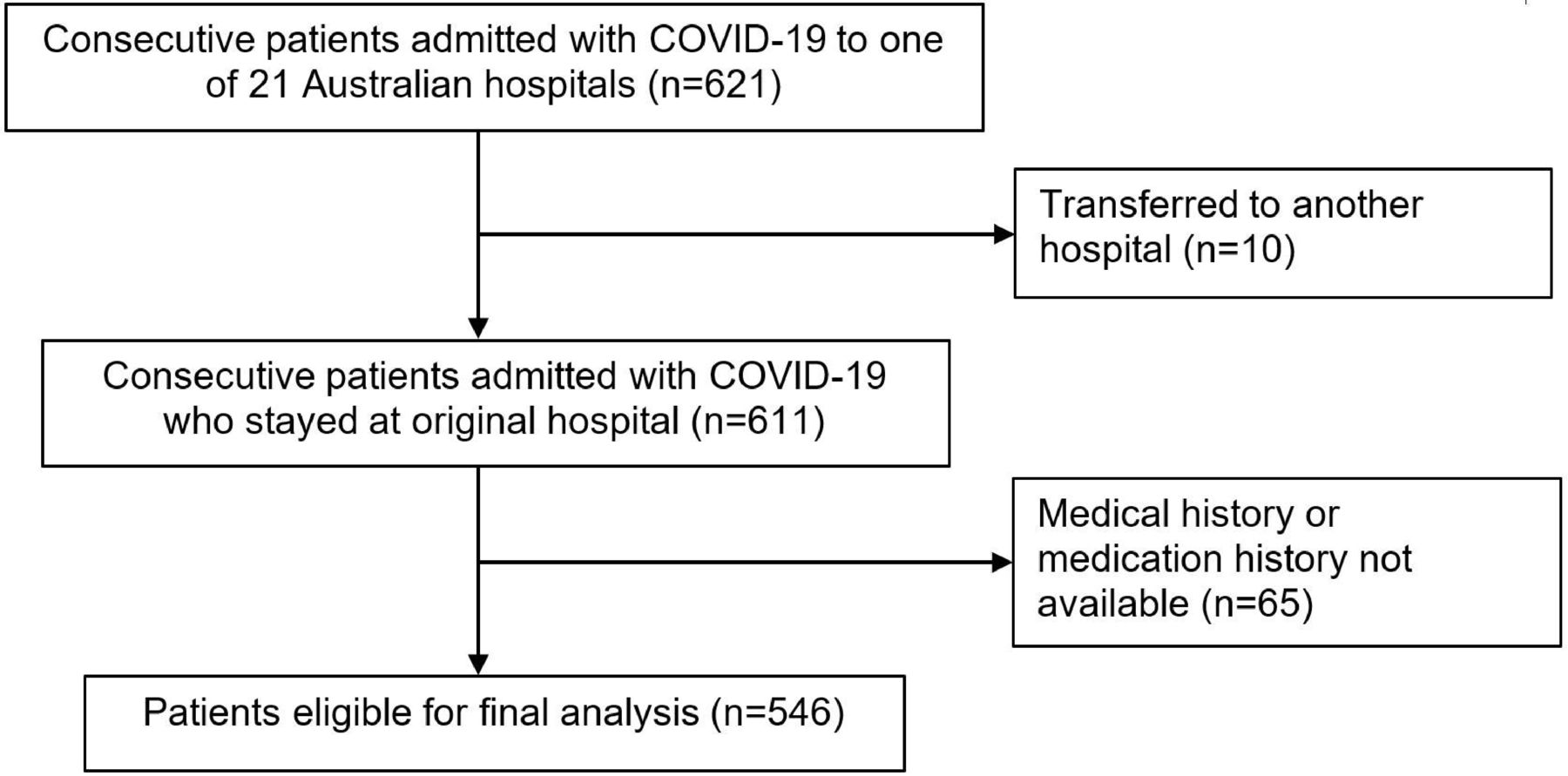
Six hundred twenty-one patients were admitted with SARS-CoV-2 infection across 21 Australian hospitals. Five hundred forty-six patients were eligible for inclusion in the primary analysis. Ten patients were excluded because they were transferred to another hospital and a further 65 patients were excluded because their medical or medication history was not available.(figure 1)
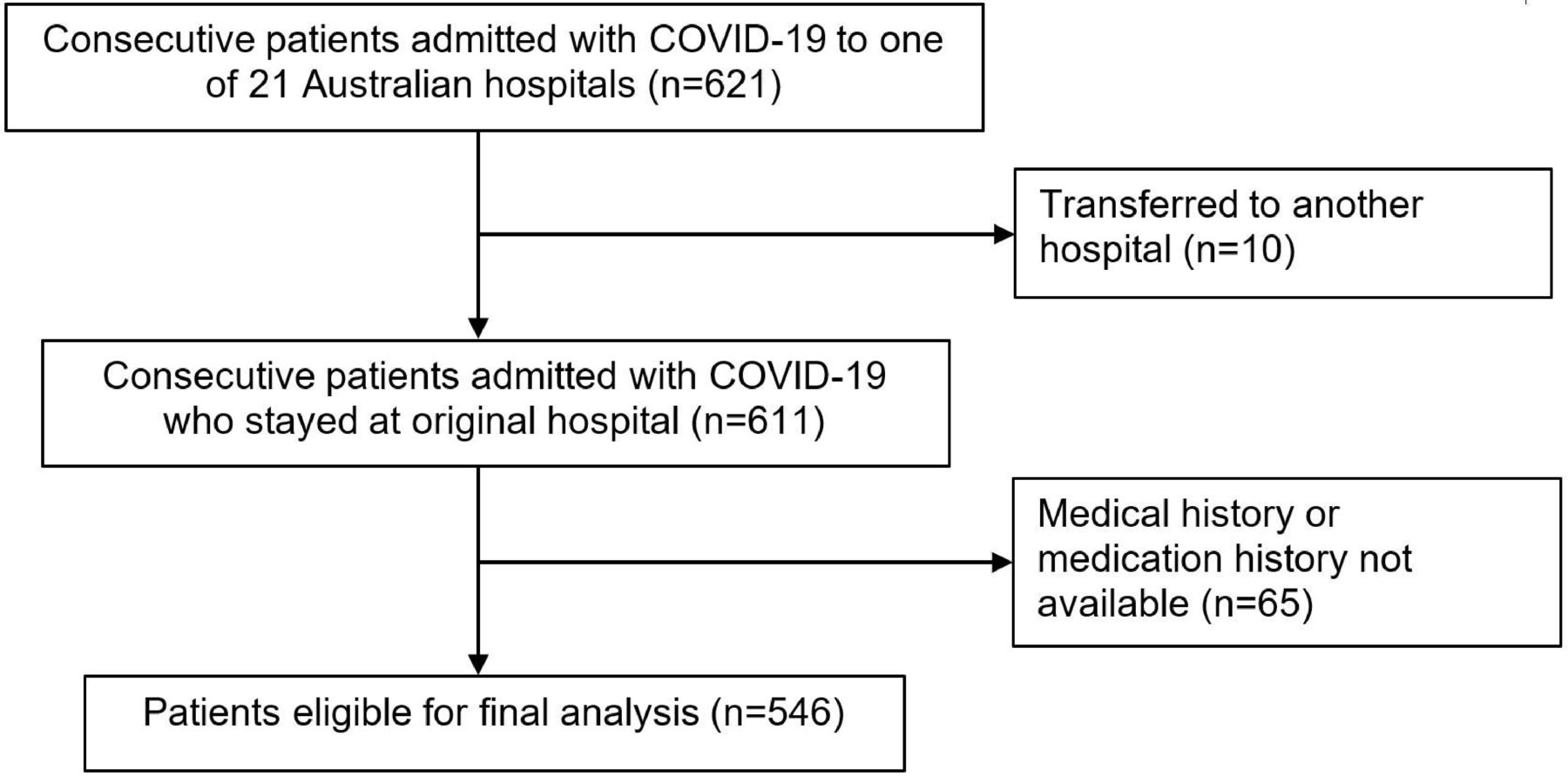
STROBE flow diagram of study population. Patient selection flow diagram. Five hundred and forty-six patients were eligible for final analysis out of 621 consecutively admitted patients. STROBE, Strengthening the Reporting of Observational Studies in Epidemiology.
The mean age of included patients was 62.9 (±19.8) years. Two hundred and eighty-three (51.8%) patients were male, 92 (16.8%) were nursing home residents and 35 (6.4%) were healthcare workers. Baseline comorbidities are presented in table 1. Two-hundred and seventy (49.5%) patients had a history of hypertension, 158 (28.9%) had hypercholesterolaemia, 143 (26.2%) had diabetes mellitus, 64 (11.7%) had coronary artery disease and 46 (8.4%) had chronic kidney disease.
Baseline demographics and comorbidities on admission
Ninety-nine (18.1%) patients were admitted to the ICU; 56 (10.3%) patients were intubated; 81 (14.8%) patients died in hospital.
Hypertension was more common in patients who died (71.6% vs 45.6%, p<0.001), as was advanced age (81.7 vs 59.6 years, p<0.001), coronary artery disease (25.9% vs 9.2%, p<0.001), heart failure or cardiomyopathy (22.2% vs 3.7%, p<0.001), stroke or TIA (17.3% vs 5.6%, p<0.001), atrial fibrillation or flutter (19.8% vs 8.2%, p=0.004), severe valvular disease (6.2% vs 1.7%, p=0.031), diabetes mellitus (40.7% vs 23.7%, p=0.002), COPD (21.0 vs 6.2%, p<0.001) and chronic kidney disease (21.0 vs 6.2%, p<0.001). Sex was not significantly different between patients who died and those who survived (male 53.1% vs 51.6%, p=0.81).
The unadjusted ORs from the univariable binary logistic regression are presented in table 2. Hypertension had an unadjusted OR of 3.01 (95% CI 1.80 to 5.04, p<0.001) for in-hospital mortality. Other variables that were significant on the univariable analysis were age (OR 1.10, 95% CI 1.08 to 1.13, p<0.001), coronary artery disease (OR 3.44, 95% CI 1.91 to 6.18, p<0.001), heart failure or cardiomyopathy (OR 7.53, 95% CI 3.69 to 15.37, p<0.001), atrial fibrillation or flutter (OR 2.77, 95% CI 1.46 to 5.24, p=0.002), severe valvular disease (OR 3.76, 95% CI 1.20 to 11.79, p=0.023), stroke or TIA (OR 3.53, 95% CI 1.75 to 7.10, p<0.001), diabetes mellitus (OR 2.22, 95% CI 1.36 to 3.63, p=0.002), COPD (OR 3.99, 95% CI 2.08 to 7.68, p<0.001) and chronic kidney disease (OR 3.99, 95% CI 2.08 to 7.68, p<0.001).
Unadjusted ORs for in-hospital mortality by baseline characteristics
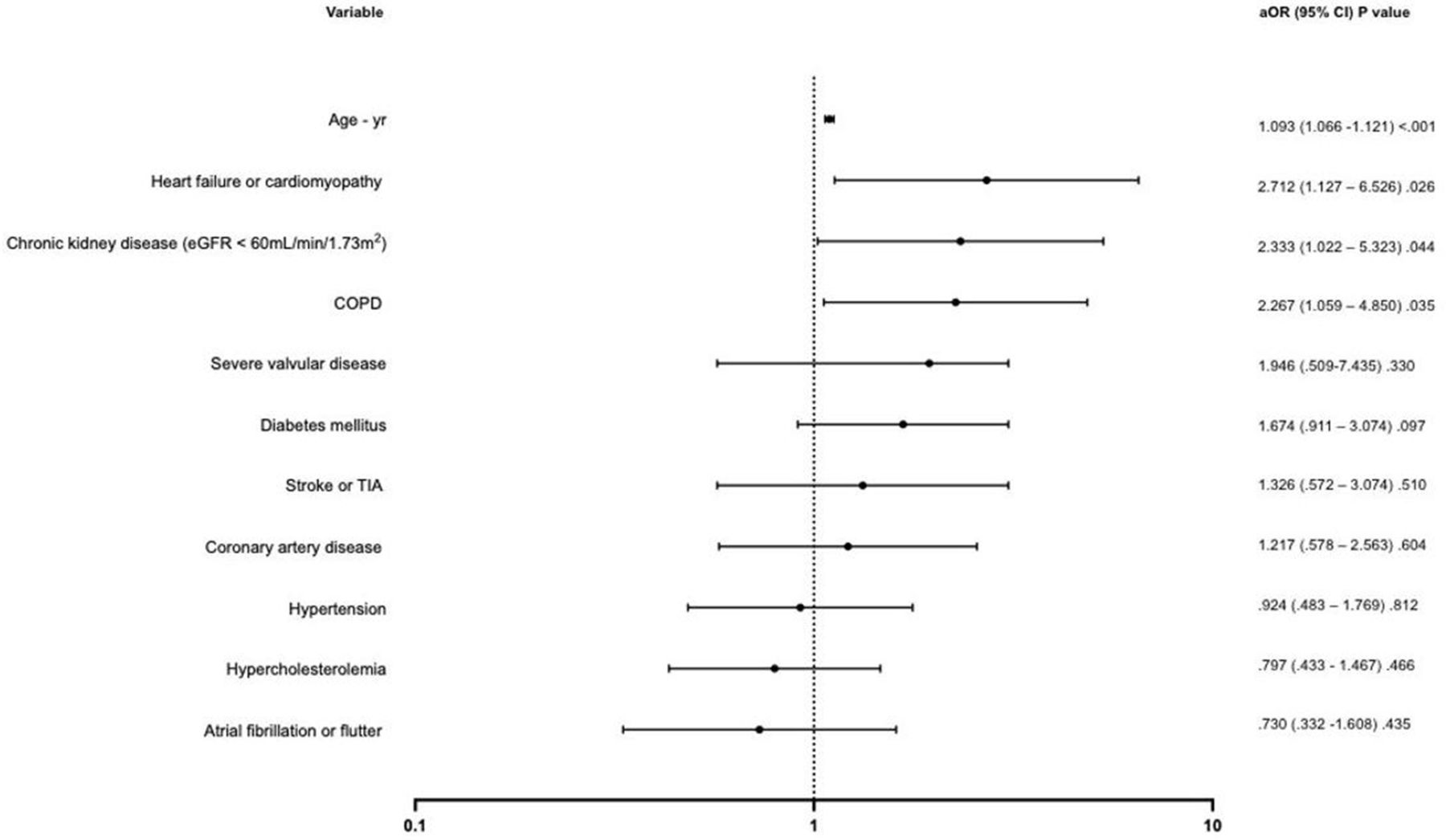
The multivariable binary logistic regression model was statistically significant (χ2(11)=136.22, p<0.001). The model correctly classified 85.3% of cases. In the multivariable model, age (aOR 1.09, 95% CI 1.07 to 1.12, p<0.001), heart failure or cardiomyopathy (aOR 2.71, 95% CI 1.13 to 6.53, p=0.026), chronic kidney disease (aOR 2.33, 95% CI 1.02 to 5.32, p=0.044) and COPD (aOR 2.27, 95% CI 1.06 to 4.85, p=0.035) were associated with an increased risk of mortality. Hypertension was not independently associated with increased mortality (aOR 0.92, 95% CI 0.48 to 1.77, p=0.81).(figure 2)(table 3)

{kind=link}
{kind=link}
Forrest plot of multivariable logistic regression for in-hospital mortality by baseline characteristics. Adjusted ORs (aORs) for in-hospital mortality derived from multivariable binary logistic regression. COPD, chronic obstructive pulmonary disease; eGFR, estimated glomerular filtration rate; TIA, transient ischaemic attack.
Adjusted ORs for in-hospital mortality by baseline characteristics
A secondary analysis was performed on the 270 patients with pre-existing hypertension. The mean age of these patients was 72.7 (±14) years (online supplemental table 1). Fifty-eight (21.5%) patients died. The use of an ARB was less common in patients who died (20.7% vs 41.5%, p=0.004). There was no difference in use of ACE inhibitors in those who died compared with those who survived (29.3% vs 25.5%, p=0.61). In the multivariable binary logistic regression model, ACE inhibitor (aOR 1.37, 95% CI 0.61 to 3.08, p=0.61) and ARB (aOR 0.64, 95% CI 0.27 to 1.49, p=0.30) use was not associated with increased mortality (online supplemental table 3).
Supplemental material
Discussion
Hypertension
In this multicentre registry of over 500 consecutive patients hospitalised with COVID-19, hypertension was the most prevalent cardiovascular comorbidity. We found that hypertension was associated with increased mortality on univariable but not multivariable analysis, adjusted for age, sex and comorbidities. By comparison, cardiovascular factors commonly associated with hypertension such as age, heart failure or cardiomyopathy, chronic kidney disease and COPD were significant independent predictors of mortality.
In contrast, an early study from China found that hypertension was independently associated with a composite endpoint of ICU admission, mechanical ventilation and death (HR 1.58, 95% CI 1.07 to 2.32, p=0.022).2 However, the results should be interpreted with caution since the analysis only adjusted for age and smoking status. Furthermore, decisions around ICU admission and mechanical ventilation can be subjective and may therefore differ between geographical regions and may depend on the availability of limited healthcare resources.
A further retrospective observational study based in Wuhan, China also showed that hypertension was independently associated with in-hospital mortality, even after adjusting for confounders including but not limited to age, sex, cardiovascular diseases and COPD (HR 2.12, 95% CI 1.17 to 3.82, p=0.013).14 This study, however, was based in a new emergency hospital constructed for the purpose of managing patients with COVID-19 and it is therefore unclear the extent to which these results are generalisable to the wider population treated in a non-pandemic healthcare system.
Consistent with results of our study, analysis of data from a multicentre US surveillance network for hospitalised patients with COVID-19 found that hypertension was neither associated with ICU admission (adjusted RR (aRR) 0.92, 95% CI 0.79 to 1.07) nor death (aRR 1.07, 95% CI 0.79 to 1.45) after adjustment for demographic characteristics and comorbidities including age, sex, cardiovascular disease and chronic lung disease.15 Likewise, a study of individuals in the US Department of Veterans Affairs national healthcare system found that hypertension was not associated with mortality (adjusted HR (aHR) 0.95, 95% CI 0.81 to 1.12) after adjusting for confounders including sociodemographic characteristics, comorbidities and presenting symptoms.3 Notably, however, this study was restricted to the veteran affairs system and included a high proportion of male patients, constituting 91% of the cohort. Additionally, a two-centre prospective cohort study in New York found that hypertension was associated with in-hospital mortality on univariable but not multivariable analysis (aHR 1.58, 95% CI 0.89 to 2.81) after adjusting for demographic factors and comorbidities including advanced age, sex, duration of symptoms prior to hospitalisation, cardiovascular disease and chronic lung disease.4 A further large retrospective study based in New York similarly found that hypertension was not associated with in-hospital mortality on multivariable analysis (aOR 0.84, 95% CI 0.65 to 1.10, p=0.214).16
ACE inhibitors and ARBs
There has been conjecture in the literature about the effect of ACE inhibitors and ARBs on COVID-19 prognosis. In the present study, multivariable analysis demonstrated no evidence of harm from use of ACE inhibitors or ARBs, which corresponds to much of the existing literature on this topic. One study based in France did, however, show that use of ACE inhibitors or ARBs was associated with higher risk of admission to ICU or death before ICU admission.10 This study was notably in a particularly elderly and unwell cohort of patients, with a median age of 73 years and mortality of 23.5% with 23 patients still in ICU at the time of analysis. In contrast, a study based in Hubei Province, China showed that after adjusting for age, gender, comorbidities and in-hospital medications, patients taking ACE inhibitors or ARBs had lower rates of all-cause mortality compared with those not taking these medications (HR 0.42, 95% CI 0.19 to 0.92, p=0.03).9 Similarly, in a large cohort from the French national health data system, it was found that ACE inhibitors and ARBs were each associated with lower risk of intubation or death compared with individuals using calcium channel blockers for hypertension. Furthermore, a randomised controlled trial of patients hospitalised with mild-to-moderate severity COVID-19 in Brazil showed no significant difference between continuation versus discontinuation of ACE inhibitors or ARBs on mortality.17
Other comorbidities
Consistent with our results, advanced age, COPD and chronic kidney disease have previously been shown to be robust predictors of adverse prognosis.3 4 15 However, the relationship between heart failure and mortality among patients hospitalised with COVID-19 has been less robustly characterised. The results of our study confirm the findings of a retrospective analysis of hospitalised patients in the USA which found that heart failure was an independent predictor of mortality (aOR 1.88, 95% CI 1.27 to 2.78, p=0.002).16 This emphasises the need to classify patients with pre-existing heart failure as a high-risk group and prioritise them in vaccine programmes.
Limitations
The AUS-COVID Registry does not include information about race and contains insufficient data on body mass index to include these potentially significant confounders in the multivariable model. The study also does not address questions about the interaction of poorly controlled hypertension and mortality. Furthermore, the registry reports on mortality during index hospitalisation only and no long-term outcome data are available. Despite these limitations, the AUS-COVID Registry is the first and largest multicentre Australian registry focused on cardiovascular comorbidities among patients hospitalised with COVID-19 and therefore provides important insights into the risk factors for adverse prognosis.
Conclusion
In patients hospitalised with COVID-19, a history of COPD, heart failure or cardiomyopathy, chronic kidney disease and advanced age were independent risk factors for mortality. While hypertension was the most prevalent cardiovascular comorbidity, it was not independently associated with mortality. Similarly, the baseline use of ACE inhibitors or ARBs had no independent association with in-hospital mortality.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
The AUS-COVID Registry was approved by the Northern Sydney Local Health District Human Research Ethics Committee (HREC 2020/ETH00732), which granted a waiver of consent.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors All listed authors contributed to interpretation of data as well as drafting and revision of the manuscript for this study. KB, HS, WVG, LK, CKC and RB were responsible for the study design and acted as the steering committee. Statistical analysis was conducted by KB, HS, JCiofani and JChia, KB is responsible for the overall content of this article as guarantor.
Funding This study is supported by unrestricted grants from the Paul Ramsay Foundation and the Northern Sydney Local Health District.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.