Article Text

Abstract
Background Early studies evaluating the performance of bioresorbable scaffold (BRS) Absorb in in-stent restenosis (ISR) lesions indicated promising short-term to mid-term outcomes.
Aims To evaluate long-term outcomes (up to 5 years) of patients with ISR treated with the Absorb BRS.
Methods We did an observational analysis of long-term outcomes of patients treated for ISR using the Absorb BRS (Abbott Vascular, Santa Clara, California, USA) between 2013 and 2016 at the Heart Centre Luzern. The main outcomes included a device-oriented composite endpoint (DOCE), defined as composite of cardiac death, target vessel (TV) myocardial infarction and TV revascularisation, target lesion revascularisation and scaffold thrombosis (ScT).
Results Overall, 118 ISR lesions were treated using totally 131 BRS among 89 patients and 31 (35%) presented with an acute coronary syndrome. The median follow-up time was 66.3 (IQR 52.3–77) months. A DOCE had occurred in 17% at 1 year, 27% at 2 years and 40% at 5 years of all patients treated for ISR using Absorb. ScTs were observed in six (8.4%) of the cohort at 5 years.
Conclusions Treatment of ISR using the everolimus-eluting BRS Absorb resulted in high rates of DOCE at 5 years. Interestingly, while event rates were low in the first year, there was a massive increase of DOCE between 1 and 5 years after scaffold implantation. With respect to its complexity, involving also a more unpredictable vascular healing process, current and future BRS should be used very restrictively for the treatment of ISR.
- cardiac catheterisation
- coronary angiography
- coronary artery disease
- percutaneous coronary intervention
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- cardiac catheterisation
- coronary angiography
- coronary artery disease
- percutaneous coronary intervention
Key questions
What is already known about this subject?
The introduction of bioresorbable scaffolds (BRSs), particularly the Absorb BRS, for treatment of coronary artery disease was received with a lot of enthusiasm and initial trial results appeared promising. Those devices were expected to provide radial strength in the early phase and dissolve over time, which results in lumen gain. However, multiple long-term follow-up studies indicated high rates of target lesion failure and scaffold thrombosis when compared with contemporary metallic stents. BRSs have also being used for treatment of in-stent restenosis (ISR). Nevertheless, long-term outcomes have not been systematically assessed yet.
What does this study add?
To the best of our knowledge, this is first study reporting long-term outcomes of patients with ISR treated with the Absorb BRS. Treatment of ISR using the everolimus-eluting Absorb resulted in high rates of adverse outcomes at 5 years, including target vessel revascularisation. Interestingly, while event rates were low in the first year, there was a remarkable increase of device related adverse outcomes between 1 and 5 years after scaffold implantation.
How might this impact on clinical practice?
Besides providing insights about long-term clinical outcomes of patients with ISR treated with the Absorb, our data also offer results additional aspects for management of patients presenting with ISR in the future, since ISR remains a clinical challenge and the optimal management is still under debate. Furthermore, our paper raises awareness on the fact that early promising results can be misleading, and the non-critical introduction of new technologies could be harmful for certain patients.
Introduction
Despite the latest advancements in percutaneous coronary interventions (PCI), including novel drug-eluting stent (DES) platforms and improved implantation techniques, in-stent restenosis (ISR) remains a commonly encountered adverse outcomes among patients with chronic coronary syndrome (CCS).1 Whereas ISR rates up to 30% had been observed with bare metal stents (BMS), more recent studies with contemporary DES still reported ISR ranging from 5% to 10%.2–4
To date, the optimal management of ISR is still under debate and represents a therapeutic challenge. Multiple approaches have been tested, including second and third-generation DES, drug-coated balloons (DCB), rotational atherectomy and brachytherapy.5 6 The latest guidelines of the European Society of Cardiology recommend either implantation of a contemporary DES (preferably an everolimus-eluting stent) or use of DCB for BMS-ISR, whereas DES-related ISR should be managed with DES. Furthermore, the use of DCB has shown favourable outcomes, especially in small-sized vessels, bifurcations, BMS-ISR and when more than two stent layers are already present in the vessel.7 8
Early after its market introduction, the everolimus-eluting bioresorbable scaffold (BRS) Absorb (Abbott Vascular, Santa Clara, California,USA) has been considered as a promising treatment option for ISR, mainly because of the fact of being integrated in the vessel wall with time, which may avoid the so called ‘onion-skin phenomenon’ (implantation of several layers of metallic stent in the same lesion), mitigating the risk for late lumen loss and improved re-endothelialisation.9 10
We published our early experience (6–12 months results) with the Absorb BRS for ISR treatment, which in fact was quite promising, including a very low incidence of target vessel revascularisation (TVR) and no scaffold thrombosis (ScT).11
Hereby, we now present the very long-term follow-up data (up to 5 years) of all patients that had been treated for clinically relevant ISR using the Absorb BRS at our institution.
Methods
All patients treated with the Absorb BRS between September 2013 and December 2016 had been included in an ongoing retrospective PCI registry (L-CAD registry, BASEC ID 2019-01067). For this study, we analysed data from all patients treated for ISR with at least one Absorb BRS. Of note, 25 patients had been included in the prospective, randomised with ABSORB-ISR study (ClinicalTrials.gov identifier: NCT02474485). The study took place at the Luzerner Kantonsspital (Lucerne, Switzerland), which represents the tertiary cardiology facility for the central part of Switzerland, with an PCI volume of approximately 1700 cases/year.
The final decision whether to use a DCB, DES or BRS for treatment of ISR remained at the discretion of the interventional cardiologist. Patients with symptomatic, stable CCS and those with acute coronary syndrome (ACS) were eligible for the study. Of note, the Absorb BRS was not used in the following settings: (1) patients with a history of a previous stent thrombosis, (2) saphenous or arterial graft lesions, (3) vessel diameters <2.5 and >4.0 mm, (4) bifurcation lesions requiring a two-stent strategy and (5) and residual stenosis >50% after predilatation.
To achieve maximum luminal gain, we routinely use non-compliant (NC) balloons for lesion preparation.12 In the context of ISR, we mainly use the ultra high-pressure NC balloons (OPN NC, SIS Medical, Winterthur, Switzerland; rated burst pressure (RBP) at 35 atm) and whenever needed intravascular imaging (optical coherence tomography, OCT, Dragonfly Abbott Vascular). All lesions were predilated using either the BEO NC (SIS Medical, Winterthur, Switzerland; RBP 24 atm) or OPN NC balloons. The Absorb BRS was implanted at 12–16 atm with gradually increasing pressure (as recommended by IFU) with the intention of completely covering the diseased segment. If necessary, postdilatation was performed using either a regular NC balloon or an OPN NC.
All angiograms were reviewed by two experienced physicians (MB and FC). The same applied for the OCT runs. The angiographic pattern of ISR was classified according to Mehran et al13 as focal (1, ISR <10 mm), diffuse (2, ISR >10 mm within the stent), proliferative (3, ISR >10 mm extending outside the stent) and occlusive (4, totally occluded ISR). Quantitative coronary angiography (QCA) analysis was performed before (if the vessel was not completely occluded) and after BRS implantation using Xcelera software, V.3.2.1 (Philips Healthcare, Best, The Netherlands). Measurements were taken on cine angiograms recorded after intracoronary nitroglycerine administration. Baseline measurements were taken with the single worst view projection and repeated in the same projection. The contrast-filled non-tapered catheter tip was used for calibration. In selected cases OCT was used to guide BRS implantation.
PCI was performed using heparin (70–100 units/kg body weight) (target activated clotting time (ACT) >230–250 s during PCI). Eptifibatide was administered only in selected patients, mainly in patients presenting with an ACS. Patients with stable CCS were discharged on aspirin and clopidogrel, while those with ACS received ticagrelor or prasugrel in addition to aspirin. Dual antiplatelet therapy was recommended for 12 months.
Follow-up was performed via telephone, clinical visits and/or chart reviewing at 6 months, 1 year, 2 years and up to 5 years after scaffold implantation. Patients with reoccurrence of angina underwent invasive coronary angiography. The patients who had been enrolled in the ABSRORB-ISR trial underwent repeat coronary angiography 9 months after scaffold implantation as per study protocol.
The primary outcome was a device-oriented composite endpoint (DOCE) defined as composite of cardiac death, target vessel myocardial infarction (TV-MI) and TVR. The secondary endpoints included target lesion revascularisation (TLR) and probable or definite ScT according to the criteria of the Academic Research Consortium (ARC).14
Categorical variables are displayed as absolute numbers and percentages, and continuous variables are presented as means (±SDs) or medians (IQRs), as appropriate. Outcomes over time were plotted using Kaplan-Meier curves. Follow-up of the patients were censored at 5 years since the index procedure. A p≤0.05 was considered as statistically significant. P values were calculated using pared t-tests and Wilcoxon rank-sum test, where applicable. The analyses were conducted using STATA V.16.
Results
In total, 89 patients were included in this study and 119 lesions were treated. The baseline characteristics are summarised in table 1. The majority of patients were male (88%) with a mean age of 66.2±9.8 years. Most of the patients presented with a CCS 58 (65%) and 42 patients (47%) had a previous MI.
Baseline characteristics of the study population
Detailed procedural and angiographic information is provided in table 2. The most commonly treated vessel represented the right coronary artery (60 cases (51%)). With respect to the ISR characteristics, 47 (40%) of the lesions represented proliferative (3) or occlusive (4) ISR, 61 (52%) showed a moderate to severe calcification and 21 (18%) were chronic total occlusions. All the lesions were predilated using NC balloons at high pressure (26.8±1.3 mm Hg). A total of 131 scaffolds were implanted at mean deployment pressure of 14.7±0.4 mm Hg. Postdilatation was performed in 58 (49%) lesions at a mean pressure of 27.7±1.9 mm Hg. OCT guidance was used in 32 (27%) lesions.
Lesion characteristics of the study population
The QCA analyses are illustrated in table 3. The mean lesion length was 22.1±1.9 mm, and the minimal lumen diameter significantly increased from 1.02±0.1 mm to 2.65±0.09 mm after BRS implantation (p<0.001).
Quantitative coronary angiography (QCA) analysis of the study population
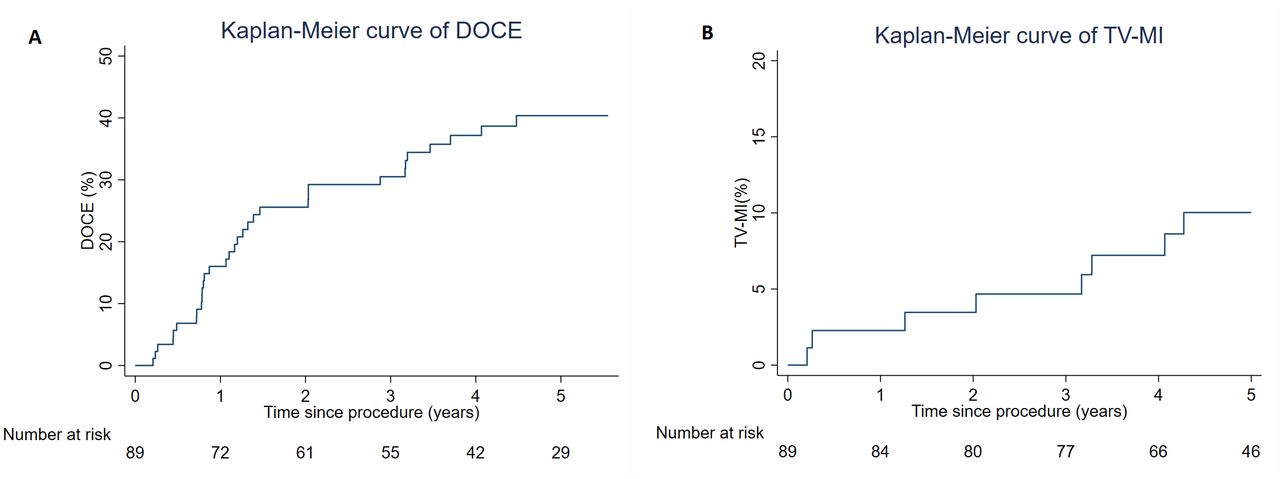
The median follow-up time was 66.3 (IQR 52.3–77) months. Overall, the primary endpoint DOCE had occurred in 17%, 27%, and 40% of all patients at 1 year, 2 years and 5 years respectively (highlighted in table 4 and figure 1A). Regarding the rate of TV-MI, this was 2.3% at 1 year, 4.7% at 2 years and of 10.0% at 5 years, as also illustrated in the figure 1B Two typical patterns of target lesion failure after BRS implantation encountered during follow-up are displayed in figure 2. The rate of ScT was low at 1 year (one case, 1.1%), but steadily increased over time (at 5 years 8.4% of all cases), whereas the majority of events occurred between the second and fifth year after scaffold implantation. Of note, a case of very late ScT was observed 41 months after implantation (case vignette, figure 3). A total of 14 (20%) patients had died at 5 years, with cardiac death accounting for 2 (3%) of the patients.
Clinical outcomes up to 5 years after implantation of the bioresorbable scaffold Absorb

Kaplan-Meier estimate of device-oriented composite outcome (DOCE) and of target vessel myocardial infarction (TV-MI): (A) graph showing the number of DOCE and (B) of TV-MI over time.

Optical coherence tomography (OCT) frames showing different scaffold failure mechanisms: (A) OCT frame of the proximal RCA showing considerable neointimal formation. The filling defects (arrowheads) indicate incomplete dissolution of the BRS scaffold 6.5 years after implantation. (B) OCT frame of the mid to distal right coronary artery (RCA) depicting overlapping scaffolds (arrows) 9 months post-treatment of a long in-stent restenosis lesion with two scaffolds. The precise positioning of the scaffolds was challenging. In this case, scaffold overlap resulted in large luminal loss. BRS, bioresorbable scaffold.
{kind=link}
{kind=link}
{kind=link}
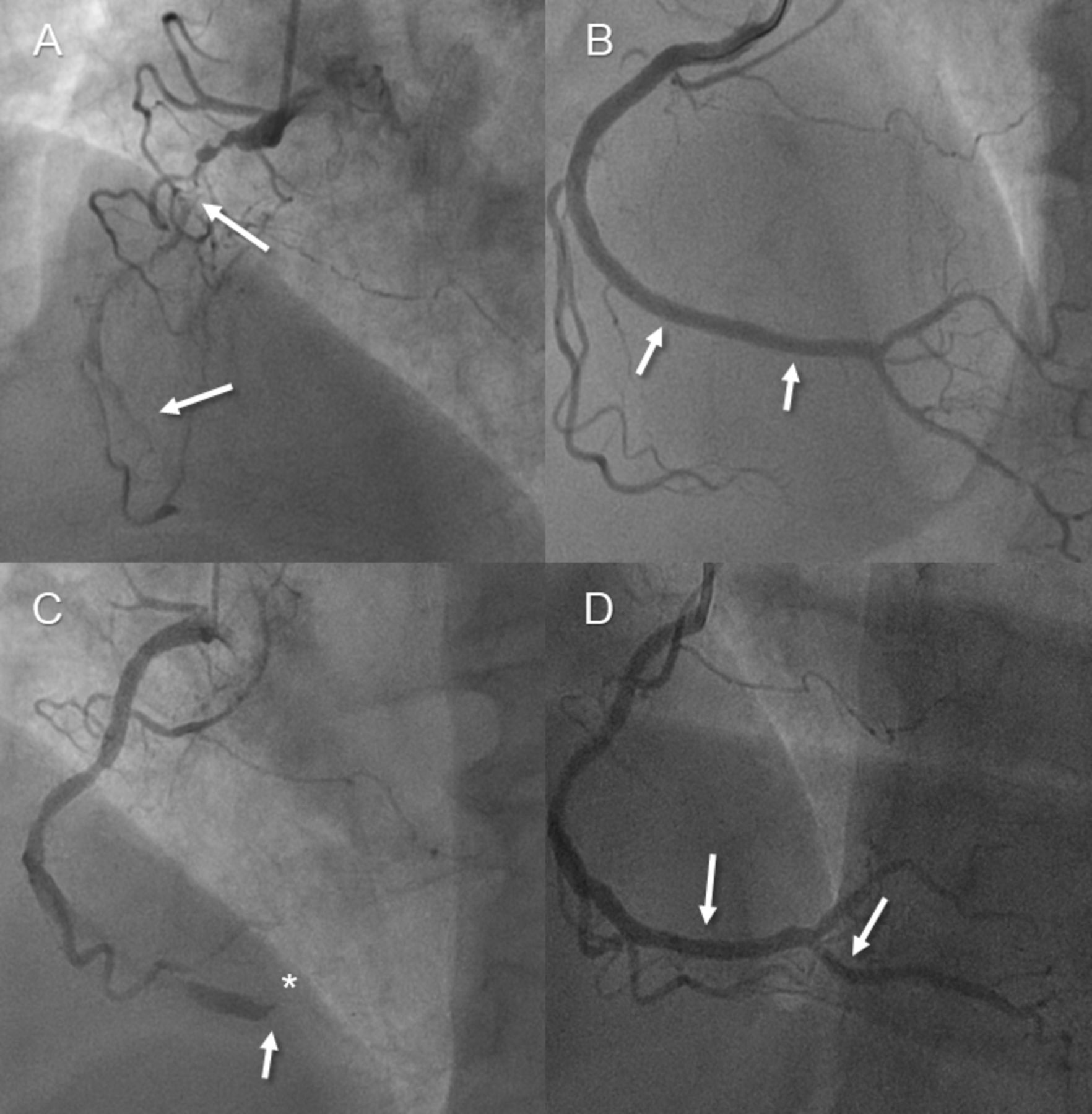
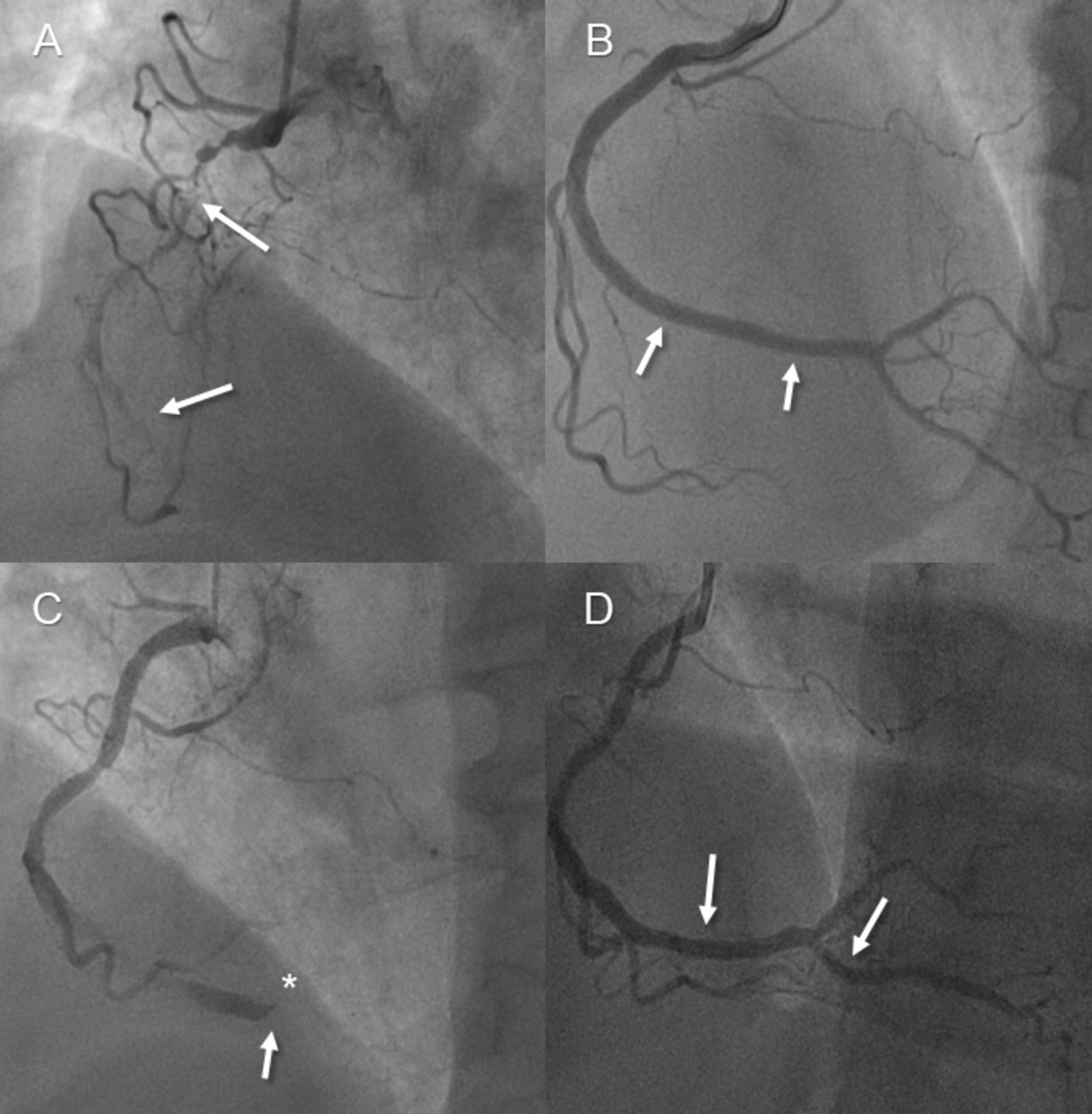
Case vignette of a patient in their 60s, presenting with target lesion failure (scaffold thrombosis) 41 months after implantation of an Absorb bioresorbable vascular scaffold (BRS) for in-stent restenosis (ISR) to the right coronary artery (RCA). (A) Initial angiogram indicating severe and long ISR of the RCA (arrow); (B) final result after ISR treatment using an everolimus-eluting Xience stent and two Absorb BRS (arrows); (C) angiogram at follow-up (after 41 months)—target lesion failure due to very late scaffold/stent thrombosis (TIMI 0 flow) (*) at the level of the distal RCA bifurcation (arrow) and (D) final angiographic result after primary PCI using two everolimus-eluting Xience stents (with TIMI three flow) (arrows). PCI, percutaneous coronary interventions. TIMI, thrombolysis In myocardial infarction.
When comparing the clinical and angiographic characteristics of patients with DOCE versus no-DOCE after ISR treatment using the BRS Absorb, we found that a number of patients with diabetes and occlusive ISR were significantly higher among those presenting with an adverse outcome during the follow-up, see table 5.
Comparison of the baseline and angiographic characteristics according to the occurrence of any DOCE versus no DOCE
Discussion
Theoretically, BRS could represent an ideal solution for treatment of ISR, since they offer a prolonged release of an antiproliferative drug and the scaffolding properties provide radial strength in the acute phase resulting in more acute luminal gain. Additionally, the expected scaffold dissolution was supposed to lead to less local chronic inflammation compared with a permanent metal implant, thus reducing the risk of neointimal tissue growth, neoatherosclerosis and thrombosis15 16
However and in line with some of the major trials evaluating the BRS Absorb for treatment of native coronary lesions, our study investigating long-term outcomes after treatment of ISR using this everolimus-eluting BRS revealed a worrying increase of DOCE between 1 and 5 years after scaffold implantation, reaching 40% at 5 years follow-up. To the best of our knowledge, this is the first study reporting very long-term follow-up data after treatment of ISR with the Absorb BRS.
Our early data implicated promising results after 6 months (TVR rate 4.6%) but an increase in TVR reaching 18.4% at 12 months.11 This was initially considered acceptable given the complexity of coronary artery disease in the treated population and a prospective randomised trial comparing the Absorb BRS versus the DCB SeQuent Please NEO was initiated.17 We observed a steep increase in DOCE between 1 and 5 years, whereas the main contributor represented TVR due to recurrent ISR. Moreover, a relevant number of patients experienced ScT. Interestingly, ScT started occurring most frequently after 2 years and still occurred up to 5 years postprocedure with the cumulative rate of ScT at 5 years reaching 8.4%, which may implicate a a persistently elevated risk for acute vessel closure due thrombotic complications (very late ScT). By comparison, large, randomised studies of ISR lesions treated with DES report TLR rates ranging from 12% to 16% at 12 months and of 33% between 3 and 5 years, with most thrombotic complications occurring between 0 and 3 years.18–22
Different structural, procedural and clinical factors could explain the failure of the Absorb BRS in the context of ISR. First, the relatively thick struts (150 µm) and the material itself (polymer poly-L-lactic acid) have been associated with an enhanced medial layer injury and inflammation and consequently higher risk of neointimal hyperplasia.23–27 Of note, we encountered a case of incomplete scaffold dissolution even 6 years after implantation (figure 2A). Second, although intravascular imaging was used in almost one-third of the patients, we need to acknowledge that in the early implementation phase of the Absorb BRS, postdilatation was not a routine procedure, due to concerns on hampering the scaffold’s integrity by aggressive postdilatation. This might have left some scaffolds somewhat underexpanded. However, the relatively low event rate in the first 6 months indirectly indicate a sufficient scaffold expansion, which also argues against a mechanical reason for DOCE. In addition, the late increase of events, consistent with the steep increase between 1 and 2 years as depicted in figure 1A, is probably linked to the early scaffold dissolution, which begin around 9–12 months after implantation and ultimately lead to loss of radial strength and vessel recoil.28 This finding could also be observed in large BRS trials in native vessels, which demonstrated low event rates in the first year post-implantation but high rates thereafter.10 21 29 30 Furthermore, scaffold overlap, as seen in one-third of our patients, may have further contributed to luminal loss (figure 2B). Finally, our study population received DAPT for the maximum of 12 months, but a prolonged DAPT regimen (up to 3 years postimplantation) could have resulted in less ScT.22 31 32
We are convinced that our study and the lessons learnt from the early BRS experience have important clinical implications. Although the Absorb BRS is not used anymore in clinical practice, other devices are still being used and developed.24 BRSs do not seem to hold the theoretical promise of a efficient antiproliferative drug carrier with self-dissolving properties resulting in late luminal gain.
Whether other scaffold platforms and materials will result in better clinical outcomes remains to be proven. In our opinion, we should apply the knowledge acquired and focus on two important features when using BRS in the future. First, the meticulous use of intravascular imaging, in order to achieve maximal luminal gain, and second the avoidance of very complex lesions (including ISR and highly calcified lesions). Early promising results can be misleading, and the non-critical introduction of new technologies could be potentially harmful for certain groups of patients.
There are several limitations to our study. First, it is a single-centre study with observational nature, thus generalisability is limited. Second, it comprises a relatively small cohort. Third, the cohort is composed of two study populations with different follow-up strategies. In particular, the repeat coronary angiography after 9 months in the RCT study may have led to the detection of asymptomatic ISR and thus to a consequently higher rate of TVR. Finally, it remains unknown if routine use of intravascular imaging, namely OCT, would have influenced the outcomes of our ISR cohort and their management. Consequently, scaffold sizing may have been ‘less precise’ among parts of the study population.
In conclusion, treatment of ISR in a high-risk population using the everolimus-eluting BRS Absorb resulted in a near linear increase of DOCE between 1 year and 5 years after scaffold implantation. Considering our experience and the high rate of adverse events, with respect to the complexity of ISR involving also an unpredictable vascular healing process, current and future BRS should be used very restrictively for this indication.
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information.
Ethics statements
Patient consent for publication
References
Footnotes
MM and GMC are joint first authors.
MB and FC are joint senior authors.
MM and GMC contributed equally.
Contributors MM and GMC: conceptualisation; data curation; methodology; writing-original draft. AA-T: conceptualisation; writing-original draft. MW: writing-original draft. FM: writing-original draft. TS: writing-original draft. LV: writing-original draft. PB: writing-original draft. ST: supervision; validation. RK: supervision; validation. MB: conceptualisation; supervision; validation; visualisation. FC: conceptualisation; supervision; validation; visualisation.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests MM, GMC, AA-T, MW, FM, TS, LV, ST and RK report no conflicts of interest. MB has received consulting and speaker fees from Amgen, Astra Zeneca, Bayer and Mundipharma. FC has received consulting and speaker fees from SIS Medical and Abbott Vascular.
Provenance and peer review Not commissioned; externally peer reviewed.