Article Text

Abstract
Objectives The risk of stroke after an acute coronary syndrome (ACS) has increased. The aim of this study was to do a comparative validation of the 6-month GRACE (Global Registry of Acute Coronary Events) risk score and CH2DS2VASc risk score to predict the risk of post-ACS ischaemic stroke.
Methods This was a retrospective study carried out in a single centre with 4229 patients with ACS discharged between 2004 and 2010 (66.9±12.8 years, 27.9% women, 64.2% underwent percutaneous coronary intervention). The primary end point is the occurrence of an ischaemic stroke during follow-up (median 4.6 years, IQR 2.7–7.1 years).
Results 184 (4.4%) patients developed an ischaemic stroke; 153 (83.2%) had sinus rhythm and 31 (16.9%) had atrial fibrillation. Patients with stroke were older, with higher rates of hypertension, diabetes, previous stroke and previous coronary artery disease. The HR for CHA2DS2VASc was 1.36 (95% CI, 1.27 to 1.48, p<0.001) and for GRACE, HR was 1.02(95% CI, 1.01 to 1.03, p<0.001). Both risk scores show adequate discriminative ability (c-index 0.63±0.02 and 0.60±0.02 for CHA2DS2VASc and GRACE, respectively). In the reclassification method there was no difference (Net Reclassification Improvement 1.98%, p=0.69). Comparing moderate-risk/high-risk patients with low-risk patients, both risk scores showed very high negative predictive value (98.5% for CHA2DS2VASc, 98.1% for GRACE). The sensitivity of CHA2DS2VASc score was higher than the GRACE risk score (95.1% vs 87.0%), whereas specificity was lower (14.4% vs 30.2%).
Conclusions The 6-month GRACE model is a clinical risk score that facilitates the identification of individual patients who are at high risk of ischaemic stroke after ACS discharge.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key questions
What is already known about this subject?
-
Patients, who survive an acute coronary syndrome (ACS), have an increased risk of stroke and therefore, a greater possibility of mortality. Most studies have assessed the incidence and predictors during admission, and during the first year of stroke post-ACS. Although there has been recently a reduction in incidence of strokes due to the advances in treatment and secondary prevention; 6-month GRACE (Global Registry of Acute Coronary Events) risk score is a useful tool to predict mortality and reinfarction. It is, however, not well defined in its ability to predict stroke after an ACS. Owing to the consequences of having an ACS, we propose this trial to assess the 6-month GRACE risk score in this setting.
What does this study add?
-
Six-month GRACE risk score estimates mortality after discharge. This proved useful to determine the long-term risk of thrombotic events and was validated in large external data sets. So far, no studies have predicted the risk of ischaemic stroke after ACS. In our study, we want to conduct a comparative validation of the 6-month GRACE risk score to predict the risk of post-ACS ischaemic stroke.
How might this impact on clinical practice?
-
Clinical practice does not have a useful tool to predict the risk of ischaemic stroke after ACS. It is important for the existence of a validated risk-standardised model to identify high-risk patients. Our study adds another utility to the 6-month GRACE risk score when it predicts thromboembolic risk. Then, 6-month GRACE risk score allows us to predict mortality, reinfarction and ischaemic stroke risk in the follow-up.
Introduction
Stroke after an acute coronary syndrome (ACS) is a rare complication. Although its incidence is higher in the first few days after ACS,1 the risk of stroke continues with the follow-up. Despite antithrombotic therapy, recent studies have shown a long-term rate of stroke after an ACS, between 1% and 4%.2–7 Also the consequences of this complication are very serious. Owing to this, it is important to identify the patients with increased risk of stroke.
To date, there are two scores that allow us to estimate the thromboembolic risk of stroke in non-valvular atrial fibrillation (AF): CHADS28 and later, CHA2DS2VASc.9 Although these two risk scores were not specifically designed to predict stroke risk after an ACS, they were recently validated in this setting.10 In addition to these, there are several scores to estimate the thrombotic risk after an ACS. The GRACE (Global Registry of Acute Coronary Events) risk score is the most extended, and it has been validated to predict death and reinfarction after an ACS.11–13
The aim of our study was to compare both risk scores, CHA2DS2VASc and 6-month GRACE risk score, to predict the long-term incidence of ischaemic stroke after an ACS.
Methods
Data sources and samples
This was a retrospective study in which demographic, clinical and angiographic data, as well as data on management and in-hospital complications, had been prospectively collected and recorded in an electronic database. All patients with a diagnosis of ACS, admitted consecutively into our hospital between January 2004 and June 2010 were included in the study. ACS diagnosis was validated if the patient had new onset symptoms consistent with cardiac ischaemia and at least one of the following criteria: cardiac biomarkers above the higher normal laboratory limit, ST-segment deviation on ECG, inhospital stress testing showing ischaemia or a known history of coronary vessel disease. Patients were classified as having acute myocardial infarction (AMI) with ST-segment elevation myocardial infarction (STEMI) or non-ST-segment elevation ACS (NSTE-ACS; unstable angina and non-ST-segment elevation AMI). The initial cohort consisted of 4645 patients; 274 patients died during the inhospital phase. Of the 4371 discharged patients, we excluded those patients in whom ACS was precipitated in the context of surgery, sepsis, trauma or cocaine consumption (n=41), and those with missing data for any variable of GRACE risk score (n=67). Of the 4263 remaining patients, 1-month follow-up was completed for 99.2% (34 patients without follow-up data). Thus, the final cohort was composed of 4229 patients. The study complies with the Declaration of Helsinki and was approved by the Clinical Research Ethics Committee of our hospital.
End point
The primary end point of this study was the occurrence of an ischaemic stroke during follow-up (median 4.6 years, IQR 2.7–7.1 years), confirmed through cerebral CT when deemed necessary by the attending neurologist. Patients were followed for a mean of 4.6 years (IQR 2.7–7.1 years) after their discharge. Methods of follow-up involved one or more of the following: use of hospital records, hospital visits, phone call to the patient’s general physician and/or phone call to the patient.
GRACE risk score calculation
The 6-month GRACE risk score was calculated for each patient by assigning the appropriate number of points for each of the nine prognostic variables that enter into the calculation: age, history of heart failure, history of AMI, heart rate and systolic blood pressure at admission, ST-segment depression, serum creatinine at admission, elevated myocardial necrosis markers or enzymes and lack of percutaneous coronary revascularisation during admission (Supplemental Data). Three risk categories were established using the cut-off points set out in the GRACE study. Therefore, in the low-risk category, the GRACE score was 27–99 points for STEMI and 1–88 for NSTE-ACS; in the intermediate risk category, the score for STEMI was 100–127 and 89–118 for NSTE-ACS; and in the high risk category, the score for STEMI was 128–263 and 119–263 for NSTE-ACS.
Statistical analysis
All analyses were performed using SPSS (V.17.0, SPSS Inc, Chicago, Illinois) and STATA V.13.0. Discrete variables are expressed as frequencies and percentages, and quantitative data are presented as the mean±SD. χ2 Test was used to compare discrete variables and the Student t test to compare quantitative variables. The correlation between the risk scores was performed using Pearson test. A Cox proportional hazards model was used to estimate the HR and 95% CI of each variable in the GRACE and CHA2DS2VASc risk scores. Both stroke and death before ACS occurrence were regarded as competing risks using sub-HR (SHR).14 Cumulative stroke rates were analysed by the method of Kaplan-Meier (Log-rank test) for the different risk groups.
The c-index15 has been used as the measure for model discrimination, equivalent to the area under a receiver operating characteristic curve; this was used to determine the performance of GRACE and CHA2DS2VASc risk scores in predicting the follow-up stroke. Negative and positive predictive values for GRACE risk score were also computed for the moderate-risk/high-risk group versus low-risk group.
We also analyse the risk reclassification with Pencina’s method.16 This allowed us to calculate the Net Reclassification Improvement (NRI). It is a fraction of net reclassification based on predictions with or without a marker, and it improves the sensitivity and specificity. A p value <0.05 was considered statistically significant.
Results
Baseline characteristics and events
A total of 4229 patients were included in the analysis. The baseline characteristics are shown in table 1. The median of follow-up was 4.6 years, IQR 2.7–7.1 years. The median time for the stroke was 3.3±2.4 years since ACS. During this period 184 (4.4%) patients developed an ischaemic stroke, 153 (83.15%) had sinus rhythm and 31 (16.85%) had AF. Patients with stroke were older, with higher rates of hypertension, diabetes, a previous stroke and previous coronary artery disease.
Clinical characteristics, in-hospital management and treatment at discharge
CHA2DS2VASc and GRACE risk scores
The CHA2DS2VASc and GRACE risks scores have demonstrated a strong correlation (r=0.685, p<0.001). The discrimination of both risks scores to predict primary end point was adequate (c-index, 0.63±0.02 and 0.60±0.02 for CHA2DS2VASc and GRACE risks scores, respectively).
The HR to predict follow-up post-ACS ischaemic stroke was 1.36 (95% CI 1.27 to 1.48, p<0.001) for CHA2DS2VASc score and 1.02 (95% CI, 1.01 to 1.03, p<0.001) for GRACE risk score. In table 2, the HR of each variable included in the CHA2DS2VASc and GRACE score was analysed.
HR of each variable of GRACE and CHA2DS2VASc
Both risk scores demonstrated a risk gradient to predict post-ACS stroke: 1.5%, 2.7% and 5.3% for low, moderate and high CHA2DS2VASc risk groups, respectively, and 1.9%, 4.8% and 5.8% for low, moderate and high GRACE risk groups, respectively. Figure 1 illustrates Kaplan-Meier curves for ischaemic strokes during the follow-up according to the risk stratification.
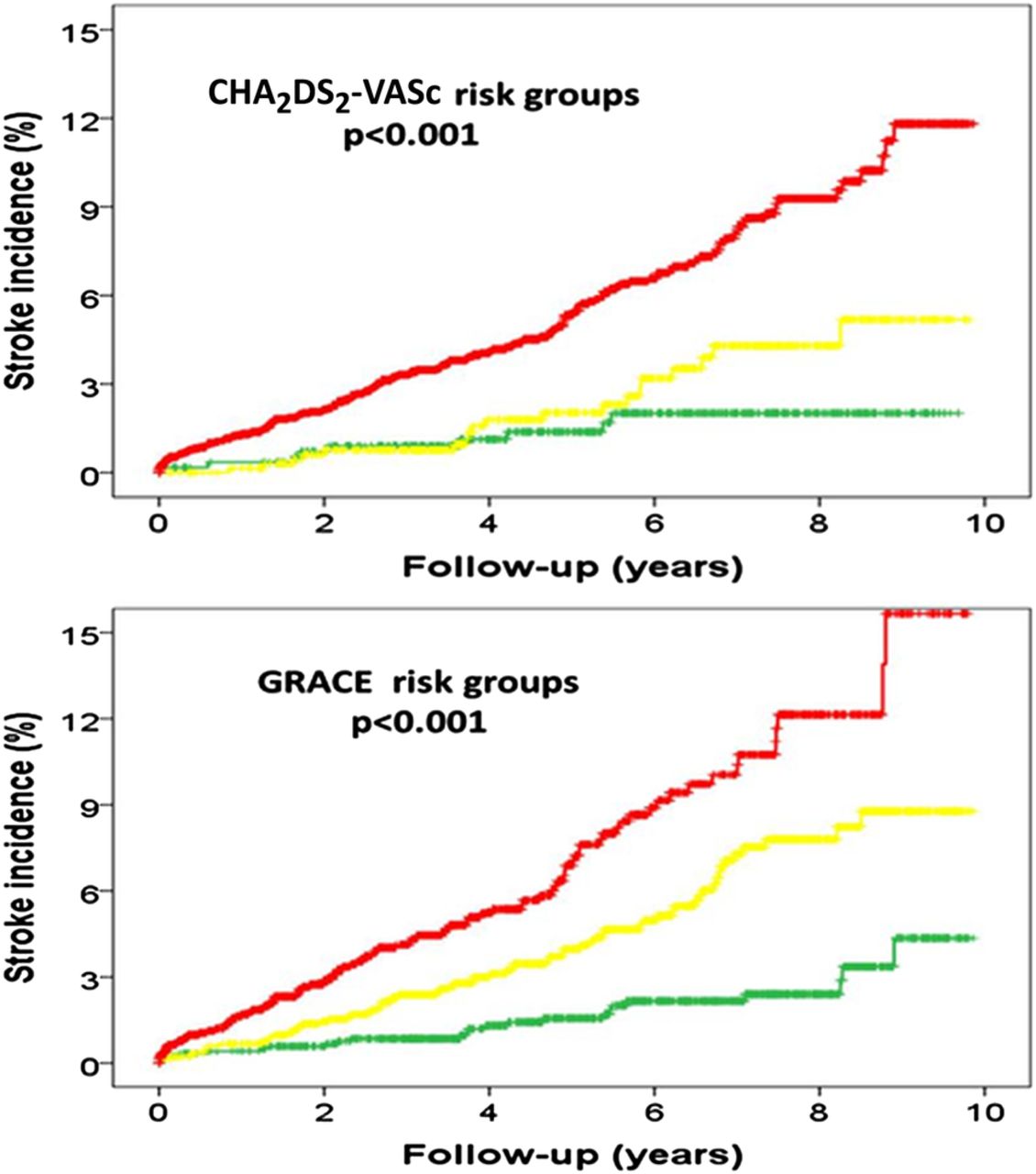
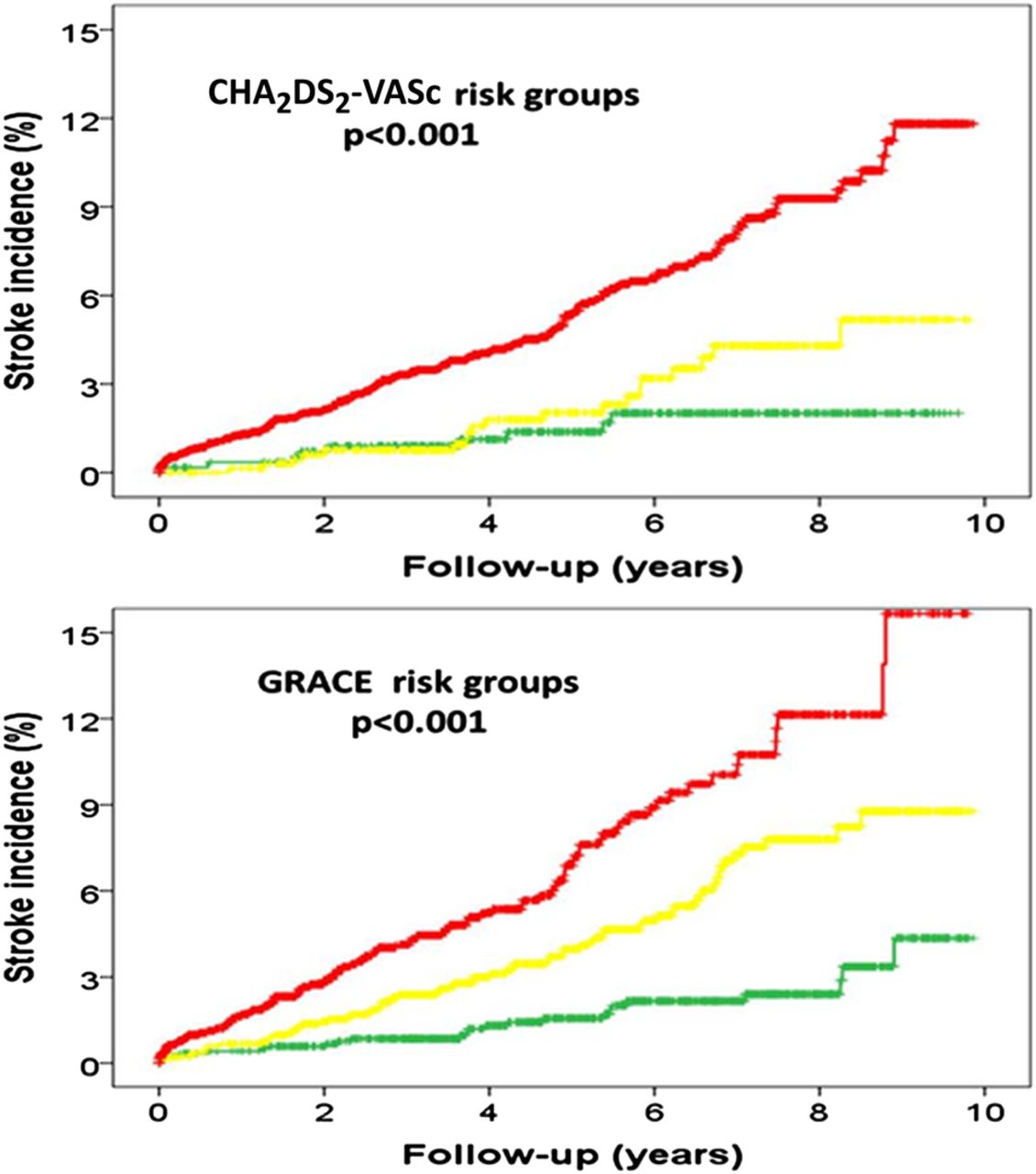{kind=link}
Kaplan-Meier curves illustrating survival according to CHA2DS2-VASc and GRACE risk scores. Green: low risk, yellow: moderate risk and red: high risk.
The negative predictive values of CHA2DS2VASc and GRACE risks scores were 98.48% (97–99.3%) and 98.07% (97.1–98.7%), respectively. After a reclassification analysis, there was no significant improvement in the global reclassification (NRI 1.98%, p=0.69).
The analysis, controlled for competitive events (death and stroke), confirmed that CHA2DS2VASc and GRACE risk scores were powerful predictors of stroke incidence during the follow-up (SHR 1.25; 95% CI 1.16 to 1.34; p<0.001, and HR 1.01; 95% CI 1.01 to 1.02; p<0.001, respectively).
Discussion
We performed a comparative validation of GRACE and CHA2DS2VASc risk scores to predict ischaemic stroke after ACS. The main clinical finding of our study was that the discriminative ability of GRACE risk score to predict the primary end point was similar to CHA2DS2VASc, even in patients with AF.
Although the GRACE risk score was validated to quantify the risk of mortality and reinfarction in the acute phase17 or in the follow-up,11 ,12 little is known about its usefulness in predicting post-ACS stroke.18 Our study provides new evidence in this setting.
Stroke, a relatively rare complication after ACS, is associated with high mortality.5 ,18 It may occur due to a multitude of reasons, such as atherosclerotic disease and thromboembolic events. Stroke represents one of the major causes of morbidity among hospital survivors of ACS. The identification of predictors for stroke in patients with ACS may help to optimise the treatment of high-risk patients. This could prevent fatal postdischarge consequences.
The incidence of stroke post-ACS has been estimated in several trials.19 This is highest in the first 5 days,1 and subsequently it is reduced.18 ,20 Most of studies had assessed the incidence of stroke after ACS during the in-hospital phase, at 30 days or in the first year. In recent years, there have been some studies about the trends in the incidence of post-ACS stroke. Brammas et al published a reduction in the incidence of mortality in patients with post-ACS stroke, in the past few years, due to the improved treatment based on evidence.19
Clinical practice guidelines recommended risk stratification in ACS,21 ,22 in the acute phase and after hospital discharge, to improve the prognosis of these patients. To date, we have several risk scores to estimate the risk of thrombotic and thromboembolic events in ACS and AF, respectively. These risk scores have been developed and validated in the past years.
The 6-month GRACE11 risk score is a simple tool for predicting mortality in patients with ACS. It was described in 2004. This is derived from the largest multinational registry and includes the complete spectrum of patients with ACS, based on independent predictors of outcome. The 6-month GRACE risk score was developed and validated with more than 20 000 patients, between 1999 and 2003, who were included in the GRACE registry (14 countries, 94 hospitals). This score allows us to calculate the probability of mortality during the first 6 months after discharge in all ACS spectrum (c-index higher than 0.70). The application of the GRACE risk score at admission was recommended by the clinical practice guidelines for risk stratification in ACS. The 6-month GRACE risk score was validated entirely across the wide range of current patients with ACS12 and demonstrated superiority over other risk scores. Its predictive value was also further validated over 6 months (even in the 5-year follow-up).13
CHA2DS2VASc9 is a simple risk stratification schema to determine thromboembolic risk in patients with non-valvular AF. It was validated in 2009; 5333 ambulant and hospitalised patients with AF were enrolled from 2003 to 2004. The CHADS2 is commonly used to assess risk of stroke, but CHA2DS2VASc scores have better discrimination of stroke risk, particularly in low-risk patients. Clinical practice guidelines recommended calculation of CHA2DS2VASc risk scores to determine whether patients with non-valvular AF need antithrombotic therapies for the prevention of stroke and systemic embolisation.
To date, no risk scores specifically estimate the risk of stroke after ACS. However, GRACE and CHA2DS2VASc risk scores could be useful in this setting. Our trial demonstrated that the accuracy of GRACE risk score was similar to the CHA2DS2VASc score to predict post-ACS stroke. This is important because with only one tool, which was initially designed to assess thrombotic risk, we can predict thromboembolic risk after ACS. We can identify patients who will benefit from a more potent antithrombotic treatment at discharge. Although our results are striking, they are in line with other studies previously published, such as Barra et al.23 Also this observational retrospective single-centre cohort study, with fewer patients (n=1.711 patients and post-ACS stroke rate of 4.3%) and a shorter follow-up (median 17.4±8.7 months), shows great predictive ability of the 6-month GRACE risk score (c-index 0.782±0.019). In our cohort, we showed there was no difference between GRACE and CHA2DS2VASc risk scores to predict the risk of stroke after ACS. We have identified the GRACE risk score as a new independent predictor of stroke post-ACS.
The stroke has been considered a complication after ACS; its frequency is especially increased in the first few months.19 One of the possible reasons that the GRACE risk score could predict the risk of stroke post-ACS is because many variables were previously demonstrated as independent predictors of post-ACS stroke. Thus, in recent years, predictors of post-ACS stroke have been identified in several trials: elderly, female sex, heart failure, coronary heart disease, AF, prior stroke, diabetes mellitus, timely revascularisation therapy, secondary prevention therapies and renal function.4 ,6 ,18 ,2 ,24–29
Advanced age, a variable with great weightage in GRACE risk score, has proven to be a powerful risk factor for stroke in this population.2 ,28 Several reports have shown that impaired renal function is also an efficient predictor of stroke and systemic embolism, and inhospital mortality of these patients. This was recently validated by Piccini et al in the ROCKET AF and ATRIAL Study Cohorts.22 Both elevated heart rate (more than 100 bpm)28 ,30 as well as a high Killip class17 at admission have demonstrated increased mortality, reinfarction as well as the greater possibility of post-ACS stroke. Also, the ST-segment changes on index ECG, specially STEMI, predicts more events.31 Likewise, the value of GRACE at admission, GRACE risk score and higher markers of myocardial damage are predictors to stroke post-ACS.17 ,31 Percutaneous coronary intervention during hospitalisation predicts a decreased risk of ischaemic stroke;30 Van De Graaff et al6 showed a significant relationship between timely revascularisation therapy and risk of inhospital ischaemic stroke. The patients with previous coronary heart disease and especially anterior myocardial infarction showed an increase in post-ACS stroke.3 Heart failure and reduced left ventricular ejection fraction4 ,18 ,32 had stronger association with mortality and also have been associated with increased risk of stroke after ACS. Because of this, although the GRACE score was not designed to determine the risk of stroke, it has good discriminative ability and a good correlation with CHA2DS2VASc to predict the primary end point. GRACE risk score included some variables which have not been included in the CHA2DS2VASc score. The high-risk GRACE score patients are usually older patients with renal failure and more Killip; therefore, these patients could be at higher risk of stroke.
Clinical implications
In recent years, there has been increasing interest to show the risk of stroke after ACS, and the risk factors associated with it. The GRACE risk score could eventually contribute to a better risk stratification and help us make decisions about interventions to reduce stroke after ACS in high-risk patients. Nowadays, the estimation of cardiovascular risk and individualisation has become a priority. GRACE risk score is used in routine clinical practice for risk stratification to optimise the treatment. Our study shows a new utility to predict stroke in the follow-up post-ACS.
Limitations
These data must be interpreted in the context of this study’s limitations. It is a retrospective analysis of clinical single centre data. Our small-sized sample should be considered the main limitation of this study. In fact, the relatively low absolute number of ischaemic stroke events during follow-up reinforces the need for more studies with larger cohorts of patients to confirm the usefulness of GRACE risk score. However, irrespective of its potential future clinical validation, our study has supported the applicability of GRACE risk score in patients with ACS prior to discharge. Moreover, as many patients who died during follow-up were not autopsied or previously observed at the emergency department, it is very hard, if not impossible in some cases, to know whether stroke was the cause of death. Therefore, the true incidence of stroke was probably underestimated.
Conclusions
The GRACE model is a clinical risk score that facilitates the identification of individual patients who are at high risk of stroke after ACS discharge. New therapeutic interventions that have the potential to limit preventable post-ACS stroke may have the greatest impact on this vulnerable population.
Acknowledgments
The authors would like to thank all the staff members (physicians, nurses and auxiliary members) and fellows from the cardiology department and coronary care unit for their support.
References
Footnotes
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No additional data are available.