Article Text

Abstract
Background There is a paucity of real-world outcome data comparing clopidogrel, prasugrel and ticagrelor in primary percutaneous coronary intervention (PPCI) for ST-segment elevation myocardial infarction (STEMI). We sought to assess the association of choice of oral P2Y12-receptor inhibitor with clinical outcomes following PPCI for STEMI in a large consecutive patient series.
Methods Demographic, procedural and 12-month outcome data were prospectively collected for all patients undergoing PPCI in Leeds, UK, between 01 January 2009 and 31 December 2011, and 01 January 2013 and 31 December 2013. Clinical endpoints were 30-day and 12-month all-cause mortality, recurrent MI and 30-day HORIZONS-major bleeding. Logistic regression analyses were undertaken to adjust for confounding factors.
Results Prasugrel (n=1244) was associated with lower adjusted 30-day (OR 0.53 (0.34–0.85)) and 12-month (OR 0.55 (0.38–0.78)) mortality, and 12-month MI (OR 0.63 (0.42–0.94)) compared with clopidogrel (n=1648). Importantly, prasugrel was associated with lower adjusted 30-day mortality (OR 0.51 (0.29–0.91)) compared with ticagrelor (n=811). Lower 30-day (OR 0.40 (0.17–0.94)) and 12-month (OR 0.54 (0.32–0.93)) MI were observed in ticagrelor compared with clopidogrel, an association absent in comparison with prasugrel. Adjusted bleeding were not statistically significantly different among the P2Y12-receptor inhibitors.
Conclusion In this large consecutive real-world series, prasugrel was associated with lower adjusted 30-day mortality compared with ticagrelor and clopidogrel, and lower adjusted 12-month mortality compared with clopidogrel. Both prasugrel and ticagrelor were associated with lower recurrent MI following PPCI compared with clopidogrel, with no overall increase in adjusted bleeding.
- percutaneous coronary intervention
- ST-elevation myocardial infarction
- mortality
- prasugrel hydrochloride
- ticagrelor
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- percutaneous coronary intervention
- ST-elevation myocardial infarction
- mortality
- prasugrel hydrochloride
- ticagrelor
Key questions
What is already known about this subject?
Ticagrelor and prasugrel have both been shown to be beneficial when used in patients with acute coronary syndromes. However, there is little available data to guide clinicians in choosing between these newer agents in primary percutaneous coronary intervention (PPCI).
What does this study add?
The main finding of this study was that prasugrel was associated with lower risk-adjusted mortality compared with both clopidogrel and ticagrelor, in patients undergoing PPCI. Both prasugrel and ticagrelor were associated with lower recurrent myocardial infarction compared with clopidogrel. There were no significant differences in bleeding among the three groups.
How might this impact on clinical practice?
The findings of this study suggest that the use of prasugrel and ticagrelor in PPCI could lead to improved outcomes compared with clopidogrel. The difference in outcomes noted between prasugrel and ticagrelor may influence prescribing choice in selected patients, until further data are published from randomised controlled trials.
Introduction
Primary percutaneous coronary intervention (PPCI) is the guideline-recommended treatment strategy for patients presenting with ST-segment elevation myocardial infarction (STEMI).1 2
The addition of oral platelet P2Y12 ADP receptor inhibitors to aspirin has been shown to significantly reduce adverse events following PCI.3–6 Therefore, dual-antiplatelet therapy (DAPT) in PPCI for STEMI has been recommended for use periprocedurally and postprocedurally up to a minimum of 12 months.1 2 7 Despite evidence of significant difference in platelet reactivity in patients treated with prasugrel compared with ticagrelor, there have been only two observational studies and one meta-analysis comparing clinical outcomes of patients treated with prasugrel with clinical outcomes of patients treated with ticagrelor in STEMI, with contrasting results.8–11 In terms of randomised controlled trials (RCTs), the PRAGUE-18 study which aimed to compare prasugrel with ticagrelor was terminated early due to futility and ISAR-REACT 5 is still ongoing.12 13
The aim of this prospective outcomes study was to obtain ‘real-world’ data from a large consecutive patient series, to facilitate comparison of clinical outcomes of patients treated with clopidogrel, prasugrel and ticagrelor when undergoing PPCI.
Methods
The West Yorkshire PPCI Outcome Study was established as a prospective, observational study to ascertain procedural and demographic characteristics, and clinical outcomes in all patients undergoing PPCI for STEMI at Leeds General Infirmary (LGI), UK. LGI is the largest single-centre PPCI centre by volume in the UK, providing a 24/7 PPCI service to a catchment population of 3.2 million people. The period of recruitment was from 1st of January 2009 until 31st of December 2011, and 1st of January 2013 until 31st of December 2013 (4 calendar years). Patients who presented between 01 January 2012 and 31 December 2012 were not included as follow-up, and data input were not possible due to limited staff availability at the time.
Primary endpoints were 30-day and 12-month all-cause mortality. Secondary endpoints were 30-day and 12-month MI, and 30-day major bleeding by HORIZONS criteria14 (defined as intracranial or intraocular bleeding; access site bleeding of diameter of ≥5 cm, or requiring intervention; a reduction in haemoglobin of ≥40 g/L without an overt source of bleeding, or ≥30 g/L with an overt source of bleeding; re-operation for bleeding and blood transfusion).
Patients who presented with chest pain consistent with myocardial ischaemia for a minimum of 20 min with ST-segment elevation of ≥1 mm in contiguous limb leads and/or ≥2 mm in contiguous chest leads, or with presumed new left bundle branch block on a 12-lead ECG were diagnosed with STEMI and were included in this study. Patients were transferred by paramedics directly to the cardiac catheter laboratories in LGI after first medical contact, with a telephone referral en route to minimise prehospital delays.15 Emergency diagnostic coronary angiography with (if indicated) follow-on PPCI was undertaken if patients presented within 12 hours of symptom onset. Oral aspirin 300 mg (administered at the point of diagnosis usually in the prehospital setting) and either 600 mg clopidogrel, 60 mg prasugrel or 180 mg oral ticagrelor (administered in the cardiac catheterisation laboratory prior to PPCI, with the exception of patients who were referred from surrounding emergency departments, who received their P2Y12-receptor inhibitor prior to transfer to the cardiac catheterisation laboratories) were administered preprocedure, depending on guideline recommendations at the time of index PPCI. Either bivalirudin or unfractionated heparin (±bail out glycoprotein IIb/IIIa inhibitor) were administered during PPCI. Arterial access site, choice of stent (drug-eluting stent (DES) or bare-metal stent (BMS)) and aspiration thrombectomy were at the operator’s discretion. Thrombolysis in MI (TIMI) classification was used to grade preprocedure and postprocedure flow in the infarct-related artery. Call-for-help time (call time) and time of patient arrival at LGI (door time) were obtained either from the ambulance reports or if patients self-presented from the emergency department triage notes. Time to first interventional device (balloon time) was obtained from the electronic cardiac catheter laboratory report. Patients were observed on the coronary care unit post-PPCI for a minimum of 24 hours, and remained in the hospital for a minimum of 72 hours (either at LGI if patients were local, or re-patriated to the nearest district general hospital after a minimum of 6 hours observation). DAPT, statin therapy, beta-adrenergic receptor blockers, ACE inhibitors (or angiotensin II receptor blockers) and (if indicated) mineralocorticoid receptor antagonists were prescribed according to guideline recommendation.
Follow-up
Written and electronic case notes were reviewed at the time of discharge to ascertain patient characteristics, procedural variables and in-hospital outcomes. Drug therapy and adverse events were identified up to a minimum of 12 months following index PPCI by a combination of patient telephone contact, accessing clinical information via written or electronic hospital records or from the responsible primary care physician. Mortality data up to a minimum of 12 months post-PPCI were obtained from the Office of National Statistics and central National Health Service (NHS) records. The Myocardial Infarction National Audit Project (MINAP) database (database with information pertaining to all patients admitted acutely into NHS hospitals in England and Wales with unstable angina, non-STEMI and STEMI) was used to identify MIs. Review of hospital discharge and clinic letters, and hospital electronic pathology servers (for a rise in creatine kinase and/or troponin, and drops in haemoglobin) were undertaken to verify MIs and bleeding. Event adjudication was undertaken by blinded clinicians in consensus.
Statistical analysis
Data checking and validation were undertaken to ensure the accuracy and validity of values obtained, and summary statistics were generated. All analyses were performed in IBM SPSS V.23.0.0.2. Records with incomplete data collection were excluded from the analyses. Results were analysed according to P2Y12-receptor inhibitor treatment at LGI. Continuous variables were reported as medians with their corresponding IQR. Categorical variables were reported as frequencies with their corresponding percentages (n (%)). Categorical variables were compared using χ2 tests. Continuous variables were compared using independent samples Student’s t-tests and Mann-Whitney U tests, as appropriate. A two-sided p value of ≤0.05 was considered statistically significant.
Multivariable logistic regression was used to correct for confounding variables, and all ORs from the logistic regression models were reported with 95% CIs. Variables included in the logistic regression models were: P2Y12-receptor inhibitor, diabetes mellitus, hypertension, hypercholesterolaemia, renal dysfunction, prior MI, anterior MI, peripheral vascular disease or cerebrovascular disease, age above 65 years, radial artery access, call-to-balloon time of above 120 min, glycoprotein IIb/IIIa antagonist use, presentation with cardiogenic shock, year PPCI was performed and DES implantation. These variables were selected as known confounders, and exploratory analyses revealed that all of them had p values of ≤0.10.
Results
A total of 4056 patients underwent PPCI during the recruitment period. Baseline, clinical and follow-up data were available for 3703 (91.3%) patients who were included in the analysis. Data for 30-day and 12-month mortality, as well as 30-day and 12-month MI, were available for all included patients. Data for 30-day bleeding were available for 3449 (93.1%) of the 3703 patients, who were included in the analysis.
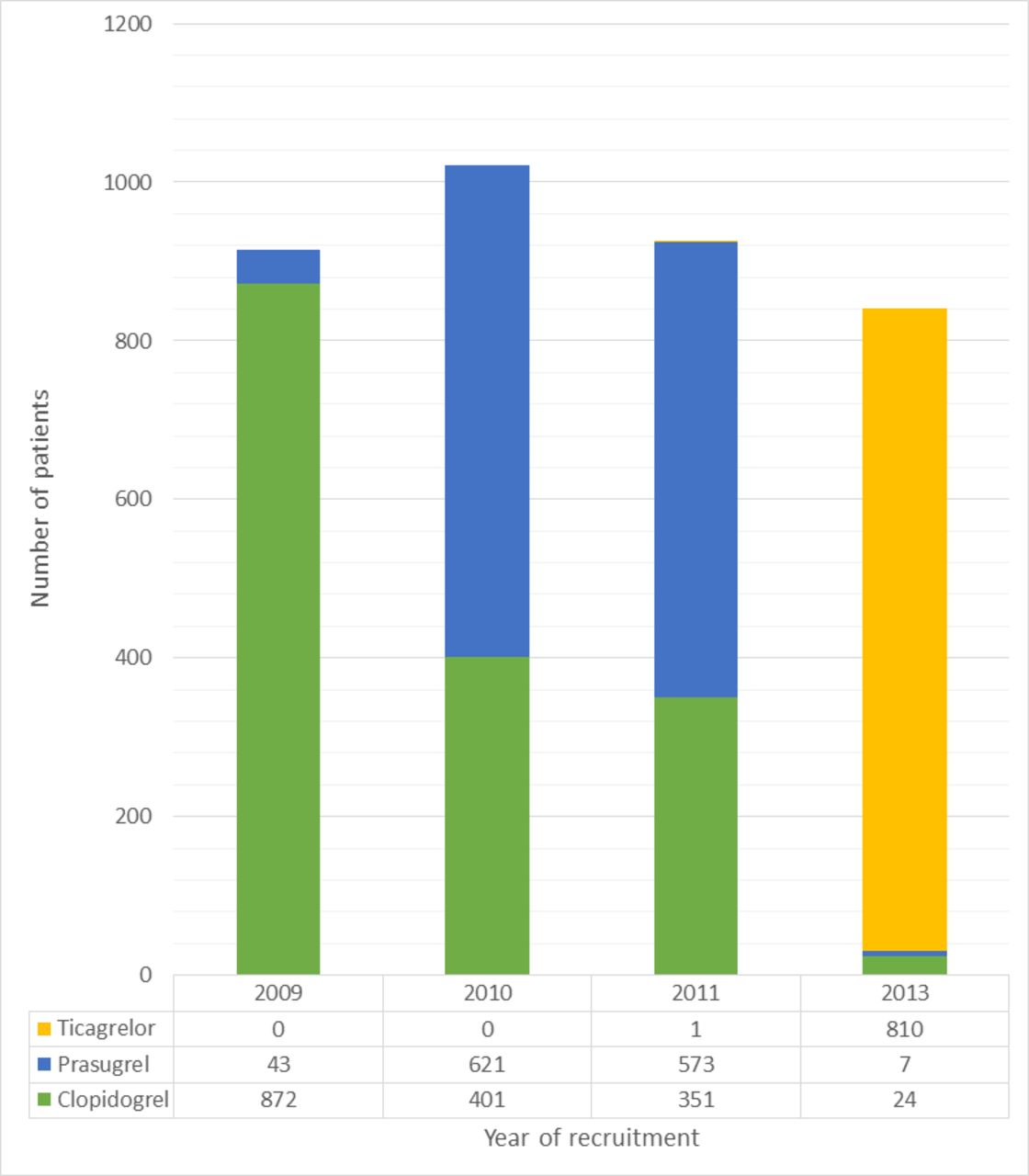
A total of 1648 (44.5%) patients received clopidogrel, 1244 (33.6%) patients received prasugrel and 811 (21.9%) patients received ticagrelor as their P2Y12-receptor inhibitor. There were multiple statistically significant differences in baseline and procedural variables (table 1). The temporal trends of use of each P2Y12-receptor inhibitor over the study period are shown in figure 1. Unadjusted and adjusted rates of 30-day and 12-month mortality, recurrent MI and 30-day bleeding are listed in table 2.
Baseline and procedural details according to P2Y12-receptor inhibitor
{kind=link}
P2Y12-receptor inhibitor administration over the study period.
Comparison of clinical outcomes between P2Y12-receptor inhibitors
Prasugrel versus ticagrelor
Statistically significant differences in unadjusted and adjusted 30-day mortality were observed in the comparison of prasugrel with ticagrelor, favouring patients receiving prasugrel. Although unadjusted 12-month mortality was lower in patients receiving prasugrel, multivariable analysis revealed no statistically significant difference in adjusted 12-month mortality between the two groups. Unadjusted and adjusted 30-day bleeding were not statistically significantly different between the two groups either (table 2).
Prasugrel versus clopidogrel
Comparison of prasugrel and clopidogrel revealed statistically significant differences in unadjusted and adjusted mortality, both at 30 days and 12 months, with both endpoints being statistically significantly lower in patients receiving prasugrel, compared with patients receiving clopidogrel. Unadjusted and adjusted 30-day MI, and adjusted 12-month MI were statistically significantly lower in patients receiving prasugrel compared with clopidogrel. Unadjusted and adjusted rates of 30-day bleeding were not statistically significantly different between the two groups (table 2).
Ticagrelor versus clopidogrel
Unadjusted and adjusted 30-day and 12-month mortality, and 30-day major bleeding were not statistically significantly different between the two groups. However, unadjusted and adjusted 30-day and 12-month MI were statistically significantly less likely in patients receiving ticagrelor compared with clopidogrel (table 2).
Discussion
Our analysis of real-world data from a large consecutive patient series from a UK tertiary cardiac centre has provided an important head-to-head clinical comparison between prasugrel and ticagrelor in the setting of PPCI for STEMI, with the first direct comparison of bleeding between ticagrelor and prasugrel. We have also compared prasugrel and ticagrelor individually with clopidogrel. Patients treated with prasugrel in this series were found to have a statistically significantly lower adjusted 30-day and 12-month mortality compared with those treated with clopidogrel, a finding which was not observed in the ticagrelor cohort compared with clopidogrel. Importantly, we have shown for the first time that patients receiving prasugrel had lower adjusted 30-day mortality compared with ticagrelor, a finding which approached, but did not reach statistical significance at 12 months (p=0.06). Both prasugrel and ticagrelor were associated with lower adjusted MI compared with clopidogrel, with ticagrelor being statistically significantly different at both 30 days and 12 months. We did not observe any difference in adjusted bleeding among the three P2Y12-receptor inhibitors.
Olier et al compared survival of >89 000 patients according to P2Y12-receptor inhibitor therapy, and found that in patients undergoing PPCI, treatment with prasugrel was associated with lower mortality compared with ticagrelor or clopidogrel, with no significant difference observed between ticagrelor and clopidogrel.10 The main finding in our study, that prasugrel use was associated with better outcomes compared with ticagrelor and clopidogrel, was in keeping with their results. Contrary to RCT findings, their study found that in-hospital bleeding was significantly lower with prasugrel and ticagrelor compared with clopidogrel, despite prior studies suggesting that the third-generation P2Y12-receptor inhibitors were more potent at platelet inhibition. However, in addition to mortality, our study compared rates of recurrent MI and 30-day bleeding, which are both important factors to consider in comparisons of P2Y12-receptor inhibitor therapy.
In comparison to the analysis by Gosling et al,9 we did not observe a reduction in mortality in patients treated with ticagrelor compared with clopidogrel. We found that prasugrel was associated with reduced mortality at 30 days and 12 months compared with clopidogrel, and at 30 days compared with ticagrelor, which was partly in keeping with their findings. In their study, although, 30-day outcomes were not presented, a signal towards lower 12-month mortality in patients receiving prasugrel compared with ticagrelor was observed (HR 0.81 (0.61–1.10)). Key differences in statistical analyses might account for the differences in findings. Gosling et al did not present or adjust for arterial access site, which could have been different between the groups if there was a temporal trend in the use of relevant P2Y12-receptor antagonist. Radial artery access was included in our regression models, and was found to be an independent predictor of outcomes, with lower adjusted 30-day (OR 0.28 (0.19–0.40)) and 12-month (OR 0.50 (0.38–0.66)) mortality, and 30-day bleeding (OR 0.40 (0.28–0.56)) compared with femoral artery access. Arterial access site is an important variable to correct for considering the wealth of evidence showing that transradial PPCI is independently associated with improved clinical outcomes compared with transfemoral PPCI.16–24 We had also adjusted for year of presentation, to try to correct for potential unrecorded confounders, such as progress with DES platforms and importantly, non-pharmacological secondary prevention. Our key finding, that the third-generation P2Y12-receptor inhibitors were associated with better outcomes compared with clopidogrel, was in keeping with their study.
Koshy et al 25 compared 12-month mortality in prasugrel and clopidogrel, and reported that patients receiving prasugrel had lower adjusted 12-month mortality compared with patients receiving clopidogrel. It is, however, important to note that patients who received prasugrel in their analysis were more likely to have undergone transradial PPCI compared with patients who received clopidogrel (78.0% vs 61.4%). However, in contrast to our study, choice of arterial access site was not included in their multivariable analysis. Postprocedural TIMI 3 flow was also included in their Cox model, which we did not include in our regression model, as it was plausible that P2Y12-receptor inhibitors could influence post-PPCI microvascular function.26 Patient age and door-to-balloon times also appeared different between our study and Koshy et al’s, and higher rates of glycoprotein IIb/IIIa inhibitor use was observed in both subgroups of their study compared with our study. Importantly, despite the difference in statistical analysis, along with differences in baseline and procedural characteristics, a similar association between prasugrel and survival was observed in both studies, with the additional finding of an inverse association between prasugrel and 12-month recurrent MI observed in our analysis.
There were several differences between the findings of our study and that of TRITON-TIMI 38.27 28 We observed lower 30-day and 12-month mortality in patients treated with prasugrel compared with clopidogrel. We also observed lower rates of recurrent MI within 12 months of index PPCI in patients receiving prasugrel compared with clopidogrel, which was in keeping with their findings. There were important differences in baseline and procedural characteristics between the PPCI subgroup of TRITON-TIMI 38 and our study that could explain these differences. The patients in our study appeared older (median age 62 vs 59) and had higher prevalence of tobacco use (67.5% vs 45.0%), but a lower prevalence of diabetes mellitus (14.3% vs 16.8%), hypertension (38.0% vs 48.7%) and hypercholesterolaemia (32.1% vs 37.6%). The patients included in our study were also more likely to receive DESs (60.1% vs 28.5%), were predominantly anticoagulated with bivalirudin (95.5% vs 1.0%) and were less likely to receive glycoprotein IIb/IIIa inhibitor (85.3% vs 66.2%) compared with the patients in TRITON TIMI 38. Our analysis of 30-day bleeding was in keeping with this study, which also found no statistically significant difference in bleeding at 30 days.
In a subgroup analysis from the PLATO investigators of patients with STEMI intended for management by PPCI,29 all-cause mortality reduction in patients treated with ticagrelor compared with patients treated with clopidogrel approached statistical significance (p=0.05) at 12 months, a finding that we did not observe in this study. The main statistically significant differences in outcomes were a reduction in vascular mortality, MI and stent thrombosis at 12 months for ticagrelor compared with clopidogrel. Conversely, an increased risk of stroke was noted in patients treated with ticagrelor. In our study, we found that patients treated with ticagrelor had lower rates of recurrent MI at 30 days and 12 months compared with patients treated with clopidogrel. We found that patients treated with ticagrelor did not have a higher rate of bleeding compared with patients treated with clopidogrel, in keeping with the PLATO substudy analysis. There were, however, important differences in clinical characteristics between the PLATO substudy and our study population that could account for the differences observed. In the PLATO substudy, patients who received open-label clopidogrel prerandomisation were then given an additional 600 mg loading dose of clopidogrel on randomisation (if randomised to clopidogrel). The majority of their patients received BMSs instead of DESs, and procedural anticoagulation was mainly achieved with unfractionated heparin, rather than bivalirudin, with higher use of glycoprotein IIb/IIIa inhibitor in comparison with our study population.
In our study, there were significant differences in baseline and procedural characteristics between the three groups of patients (table 1). There was a temporal change in the use of individual P2Y12-receptor inhibitors over the study period (figure 1). In 2009, the majority of patients undergoing PPCI in LGI received clopidogrel, with the remainder receiving prasugrel. In 2010 and 2011, the majority of patients received prasugrel and in 2013, the majority of patients received ticagrelor. During this period, there were changes in the rates of transradial PPCI (39.6% in 2009 vs 81.8% in 2013) and the use of DESs (41.3% in 2009 vs 82.2% in 2013). As a result of lower thresholds for accepting patients for PPCI, a higher proportion of patients in the ticagrelor cohort underwent PPCI for cardiogenic shock, which is traditionally regarded as a marker of poor prognosis.30 There were also advances in secondary prevention over the study period, including an increased rate of implantation of primary-prevention implantable cardioverter-defibrillator devices.31 These and other confounders, such as changes in clinical practice, improvements in operator proficiency and improvements in the PPCI pathway, could have all contributed to the differences in unadjusted outcomes. However, multivariable analysis, including adjustment for year of PPCI to adjust for unquantifiable time-dependent confounders, was undertaken to correct for major confounding factors.
Limitations
As this was a single-centre observational study, our findings might not reflect the broader population. However, our study demographics are comparable to those in the UK Myocardial Ischaemia National Audit Project (MINAP). Our practice and outcomes might not reflect those in other regions, as regional differences in STEMI management have been reported.32 We were unable to correct for Killip class. However, with this study being an ‘all-comers’ study, we have no reason to believe that there would be statistically significant differences in Killip class between the groups. There have been many advances in procedural techniques and technologies over the years such that we were not able to correct for the generation of DES used in each subgroup, which potentially could have affected outcomes. However, we tried to correct for these by adjusting for the year of admission. As this was an observational study, the study populations were unmatched. However, multivariable analyses were undertaken to adjust for major confounders. Perhaps most importantly we were unable to fully ascertain continuation and/or switching of P2Y12-receptor inhibitors following discharge, but this limitation was also present in the only other comparable real-world studies.9 10 25 Switching from ticagrelor was noted in PLATO due to dyspnoea, but also perhaps due to compliance with its two times per day administration. However, in our study, differences in outcomes were observed in all three comparisons of P2Y12-receptor inhibitors, which should not have been observed if switching of P2Y12-receptor inhibitor therapy influenced differences in outcomes. Event rates in this study were low compared with PLATO or TRITON-TIMI 38 that involved larger numbers of patients, as under-reporting of adverse events is more likely in observational studies compared with RCTs, and therefore play of chance could not be excluded. We were also unable to obtain details of other changes to secondary prevention (aspirin, beta-adrenergic receptor blockers, ACE-inhibitors and statins) at 30 days and 12 months. However, they were unlikely to be different across the groups as they were all part of guideline-indicated care through the period of study. Finally, the findings observed in this study should be hypothesis-generating, and an adequately powered RCT may be able to reveal differences in outcomes between P2Y12-receptor inhibitors that might inform future guidelines pertaining to optimal DAPT strategy following PPCI.
Conclusion
In PPCI, treatment with prasugrel was independently associated with lower adjusted probabilities of 30-day and 12-month mortality, and 12-month MI compared with clopidogrel. Importantly, treatment with prasugrel was independently associated with lower adjusted 30-day mortality compared with ticagrelor. Although 30-day and 12-month MI were lower in patients treated with ticagrelor compared with clopidogrel, there were no significant differences in 30-day and 12-month mortality between patients treated with ticagrelor and clopidogrel. Overall, the third-generation P2Y12-receptor inhibitors were associated with lower adverse outcomes compared with clopidogrel, with no excess bleeding.
References
Footnotes
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests Daiichi Sankyo partially contributed to the overall postgraduate degree research fellowship salary of AK. AK, SW, JB, JM and CM have received honoraria from AstraZeneca for presentations. Neither company, in any capacity, have had access to or were involved in data collection and analysis, or the preparation of this manuscript.
Patient consent for publication Not required.
Ethics approval UK National Research Ethics Service approval (0911-11311/60) and NHS approval from each hospital within the region were obtained.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement The data for this study are available from the corresponding author, upon reasonable request.