Article Text

Abstract
Objectives To compare the shape and strength of the associations of resting heart rate (RHR) with incident heart failure (HF) and pulmonary heart disease (PHD) in Chinese adults.
Methods The prospective China Kadoorie Biobank recruited >0.5 million adults from 10 geographically diverse regions (5 urban, 5 rural) of China during 2004–2008. After an 11-year follow-up, 6082 incident cases of HF and 5572 cases of PHD, were recorded among 491 785 participants with no prior history of heart disease or use of beta-blockers at baseline. Cox regression yielded HRs for each disease associated with usual RHR after adjustment for confounding factors.
Results The mean (SD) baseline RHR was 79 (12) (men 78 (12); women 80 (11)) bpm, and these decreased with increasing age (by about 1 bpm per 10 years). Usual RHR showed J-shaped associations with HF and log-linear associations PHD. For HF, each 10 bpm higher usual RHR was associated with an adjusted HR of 1.25 (95% CI 1.17 to 1.34) for RHR>75 bpm. For PHD, each 10 bpm higher RHR was associated with HR of 1.74 (1.67–1.81) across the full range of usual RHR. For HF at RHR>75 bpm but not PHD, the HRs per 10 bpm higher RHR were approximately halved by further adjustment for diabetes and hypertension.
Conclusions RHR was strongly positively associated with PHD throughout the range studied, but was only associated with HF at RHR>75 bpm, and the strength of the associations with HF were only one-third of those with PHD.
- heart failure
- epidemiology
- risk factors
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Resting heart rate (RHR) is a well-established therapeutic target for the treatment of heart failure (HF), but the relevance of heart rate for pulmonary heart disease (PHD) has not been widely studied.
In the Framingham Heart Study, each 10 bpm higher RHR was associated with 14% higher risk of HF at RHR greater than 80 bpm.
WHAT THIS STUDY ADDS
In an 11-year prospective study of 0.5 million Chinese adults, we examined the shape and strength of the associations of RHR with incident cases of HF and PHD.
Among those without prior history of heart diseases or use of beta-blockers, usual RHR showed a J-shaped with incident HF and log-linear associations with PHD, respectively.
Each 10 bpm higher RHR was associated with 25% higher risk of HF at RHR >75 bpm, and with 74% higher risk of PHD throughout the full range of RHR studied.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE AND/OR POLICY
Many physicians are reluctant to use beta-blockers in patients with chronic obstructive pulmonary disease (COPD), but this study provides support for more research on the use of beta-blockers for treatment of PHD and prevention of cardiac complications of COPD.
Introduction
Heart failure (HF), which affects about 25 million people worldwide, is a clinical syndrome arising from structural or functional cardiac abnormalities that result in low cardiac output and increased pressure in the relevant cardiac chambers.1–5 Left HF is characterised by the inability of the left ventricle to supply sufficient blood to the systemic circulation and right HF or pulmonary heart disease (PHD) by an inability of the right ventricle to adequately supply the pulmonary circulation. Ischaemic heart disease, hypertensive heart disease and cardiomyopathy account for most cases of left HF and chronic respiratory diseases account for most cases of PHD.2
The incidence of HF has increased steadily in recent decades, reflecting improvements in survival following acute cardiac events, longer life expectancy and an increased prevalence of hypertension, diabetes mellitus and obesity.4 6 7 HF is also associated with high risks of recurrent hospital admissions, increased healthcare expenditure and substantial in-hospital mortality depending on the healthcare setting.5 8 9 PHD has been less widely studied than HF but is believed to account for 6%–7% of all heart disease cases in the USA.10
Higher levels of resting heart rate (RHR) have been associated with higher risks of cardiovascular disease (CVD), but the relevance of RHR for both left and right HF is uncertain.11 Higher RHR is associated with higher levels of oxidative stress, endothelial dysfunction and atheromatous plaque formation.12 Previous studies conducted in mainly Western populations have reported conflicting results, both qualitatively and quantitatively, about the associations of RHR with HF,13–16 with some studies reporting J-shaped associations between RHR and HF.15 16 It is unclear the extent to which the associations of RHR with HF may be an artefact of incomplete adjustment for confounding by established risk factors, reverse causality or both. Little is known about the associations between RHR and incident HF and PHD in Chinese populations, where the distribution of major risk factors for HF and PHD differs from those in western populations.5 17 The aims of the present study were: (i) to compare the shape and strength of the associations of usual RHR with incident HF and PHD, overall and in different population subgroups and (ii) assess the extent to which the observed associations were explained by residual confounding or reverse causality bias.
Methods
This study was reported in accordance with the Strengthening The Reporting Of Observational studies in Epidemiology (STROBE) guidelines for cohort studies.18
Study design, setting and population
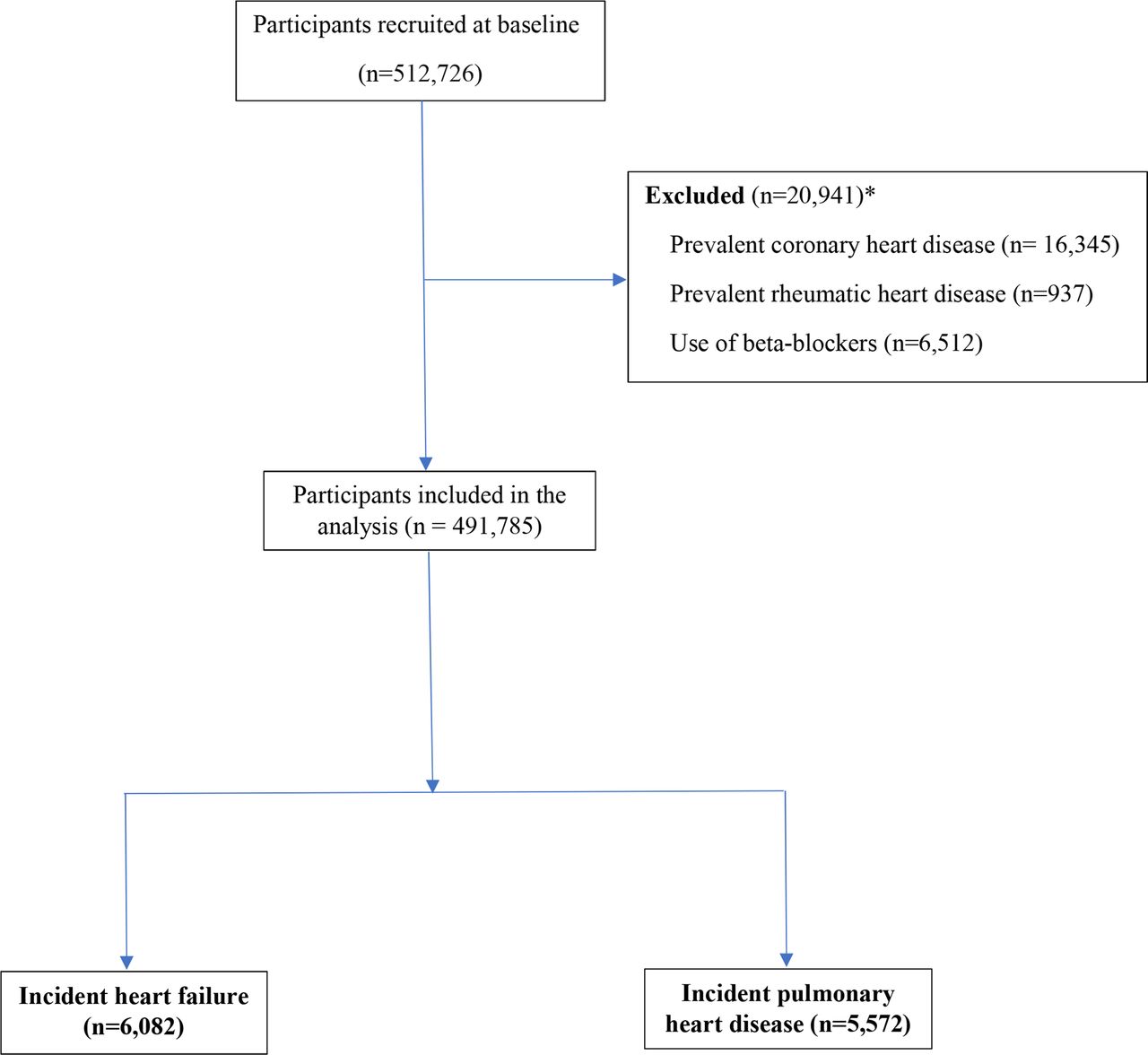
The China Kadoorie Biobank (CKB) is a prospective study of 512 726 Chinese adults who were aged 30–74 years at enrolment in 2004–2008.19 The design of the CKB study has been previously described.19–21 Briefly, participants were recruited from 10 regions in China. All permanent residents with no major disability in each of the 100–150 administrative units (comprising either urban residential areas or rural villages) were identified through official residential records and invited to participate in the study, with a response rate of about 30%.20 Less than 0.5% (n=2470) of individuals who attended the baseline survey were excluded because they withdrew their consent or had missing data. For this study, participants with a self-reported prior history of coronary heart disease (n=16 345) or rheumatic heart disease (n=937) or who reported use of beta-blockers (n=6512) at baseline were excluded. Additional analyses also excluded individuals with a prior history of chronic obstructive pulmonary disease (COPD) and other chronic diseases at baseline.
Exposures, covariates and outcomes
RHR was measured using calibrated UA-779 digital BP monitor (Omron UA-779; Live Source) to the nearest one beat per minute (bpm) after the participant had been at rest in a seated position for at least 5 min.19 RHR was measured twice, and the mean of both measurements was used for the present analyses.
Information on demographic and socioeconomic status (SES), lifestyle, medical history and self-reported health and current use of medication was collected using an interviewer-administered electronic questionnaire at local assessment clinics. All participants had mean levels of weight, height, RHR and blood pressure (BP) recorded. Repeat surveys of random samples of 5% of the CKB population (with about 80% response rates) were conducted at 4 years (2008) and 8 years (2013–2014) after baseline to assess the reproducibility of exposure variables.
Information on vital status and causes of death was collected by linkage, through unique national identification numbers, to death registries at China’s Disease Surveillance Points system, supplemented by annual active follow-up using local residential records, and contacting participants’ family members.19 Information on hospital admissions was collected by linkage to the health insurance (HI) claims system for all hospital admissions.19 Over 97% of the CKB population reported having HI coverage, and study records are updated every 6 months.19 For the small number of uninsured participants, information on hospital admissions was identified through annual active follow-up. All incident fatal and non-fatal disease outcomes were coded, using the International Classification of Diseases tenth revision (ICD-10), by trained staff who were blinded to the baseline information of study participants. In the present report, the analyses were censored at 31 December 2017. The diagnoses of HF and PHD were obtained from HI billing records, death or disease registries that followed contemporary Chinese clinical guidelines for the diagnosis of these diseases. The current clinical guidelines for HF in China include relevant symptoms (dyspnoea on exertion, orthopnoea, fatigue and oliguria) and clinical signs (bilateral pedal oedema, S3 gallop, hepatojugular reflux and pulmonary crepitations) and use of relevant medications (diuretics and angiotensin-converting enzyme II blockers).22 The current clinical guidelines for diagnosis of PHD include relevant symptoms, clinical signs and specific findings of enlarged P waves and right ventricular hypertrophy on electrocardiography and echocardiography.23 The participants with incident HF and PHD were defined as first non-fatal hospital admission or death due to HF (ICD-10: I50) or PHD (I27).
Statistical methods
Mean values and SD were used to summarise normally distributed variables, and medians and IQR were used for non-normally distributed variables. Multivariable Cox PH regression models were used to examine the associations of RHR with incident HF and PHD after stratification by region, age-at-risk, sex and season at recruitment. The multivariable regression analyses were sequentially adjusted for SES (marital status, highest level of education and household income in Yuan) and other established CVD risk factors (alcohol consumption, smoking status, physical activity in Metabolic Equivalent of Task hours per day (MET-hour/day), body mass index (BMI, in kg/m2), hypertension and diabetes mellitus). Detailed information regarding the categorisation of the covariates included in the multivariable Cox regression analysis is provided in online supplemental table. The likelihood ratio tests (LRT) for heterogeneity were used to assess departures from linearity in continuous variables or ordinal categorical variables. The LRT for heterogeneity was used to assess changes in the χ2 statistic for the associations of RHR with incident HF or PHD after sequential addition of potential confounding factors.24
Supplemental material
All associations of RHR with disease outcomes were corrected for regression dilution bias, by estimating the HRs and their corresponding 95% CI for fifths of baseline RHR and these were plotted against the mean baseline resurvey RHR in the respective baseline-defined groups. The quintile-specific HR and 95% CI were estimated using the floating absolute risk method,25 which enabled comparisons of the risks of HF or PHD between any two quintiles of RHR. Moreover, in the setting of a linear association of RHR with HF or PHD, the log HRs per 10 bpm higher baseline RHR (and their associated SEs) were divided by the regression dilution ratio (RDR) to obtain HRs per 10 bpm higher usual RHR.26 The RDR was computed using the MacMahon Peto method.26 27
Interaction terms were fitted to assess possible effect modification by age (at baseline), sex, smoking, BMI, physical activity, hypertension and diabetes and LRT were used to assess possible effect modification. Sensitivity analyses excluded first events of HF and PHD that occurred during the first 5 years of follow-up or individuals with any prior non-vascular diseases at baseline (chronic obstructive pulmonary disease, emphysema, bronchitis, pulmonary tuberculosis, asthma, any cancer, kidney disease, cirrhosis or hepatitis B or rheumatoid arthritis) or participants with poor self-reported health status at baseline. The impact of additional exclusions of participants with prior stroke or use of BP-lowering medications was also assessed. In addition, we excluded cases of PHD secondary to first HF diagnosis. Similarly, cases of HF after PHD diagnosis were also excluded. Two-tailed p values less than 0.05 were considered statistically significant. Data were analysed using Stata V.16.1 and R V.4.1.
Patient and public involvement
Local community leaders in China were consulted prior to enrolment of study participants in CKB. The findings of the CKB study are reported in peer-review publications and any relevant public health messages are disseminated using local press, television and internet to study participants.
Results
Selected baseline characteristics are shown for 491 785 eligible study participants classified by quintiles of RHR in Table 1. Figure 1 shows the flowchart for selection of the study participants. The mean (SD) age was 51.7 (10.6) years, and 60% were women (table 1). Overall, the baseline mean (SD) RHR was 79 (12) bpm (men: 78 (12); women 80 (11)), and RHR declined progressively with increasing age (by 0.76 bpm per 10-year increase). Individuals who were current smokers, less physically active or overweight or had hypertension, obesity or diabetes mellitus had higher mean RHR compared with those without such risk factors (table 1).
Baseline characteristics of all study participants by fifths of resting heart rate

Flow sheet for selection of the study participants. *Categories are not mutually exclusive and, hence, do not add up to 20 941.
Association of usual resting heart rate with incident heart failure and pulmonary heart disease
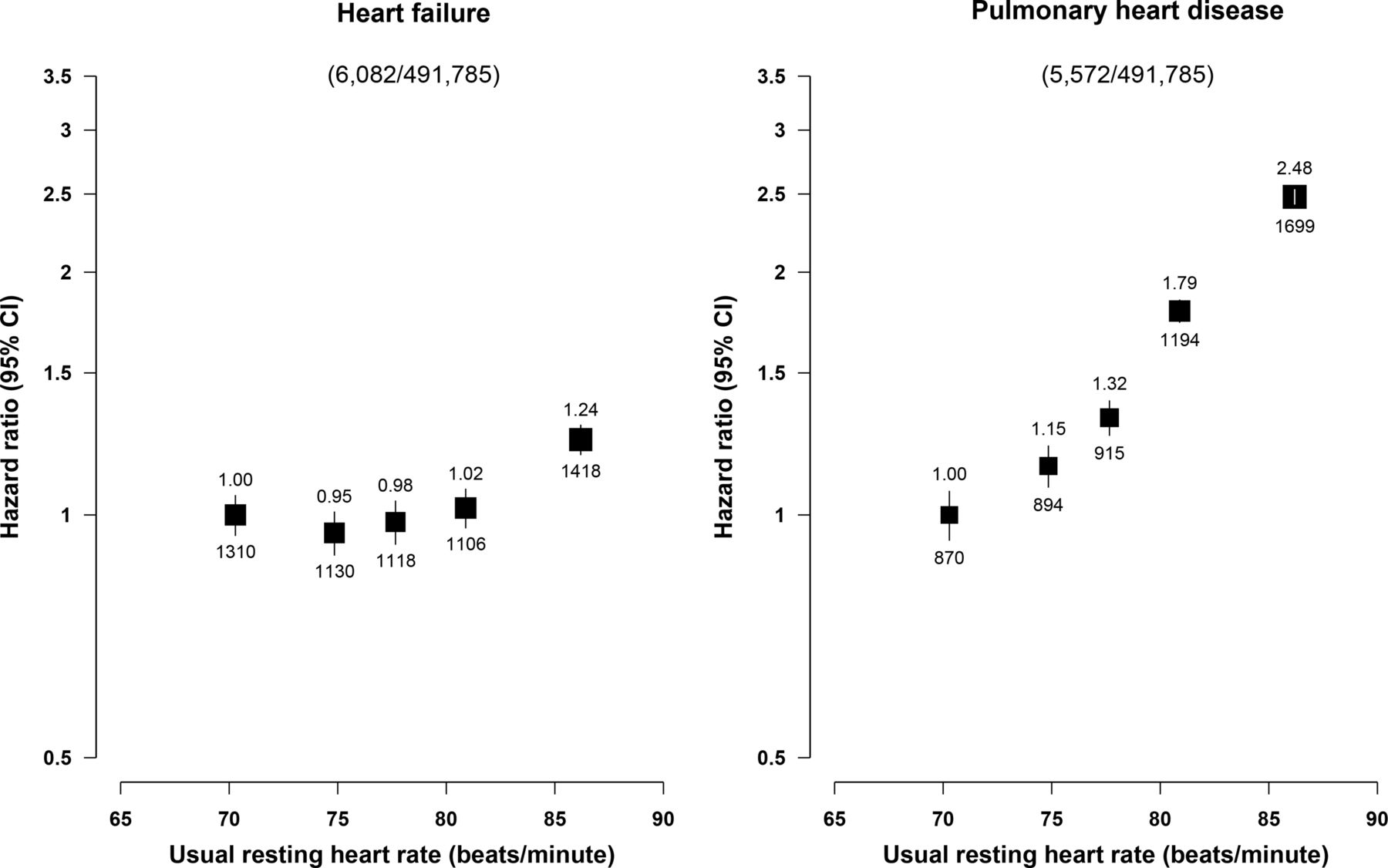
During a median follow-up of 11.1 years (IQR: 10.2–12.1) years, 6082 participants had HF and 5572 had PHD, respectively. A total of only 263 (4.7%) of the 5572 PHD occurred following a diagnosis of HF and only 325 (5.2%) of HF cases occurred after a diagnosis of PHD. There was a J-shaped association of RHR with HF, with a weak inverse association at RHR <75 bpm, but an approximately log-linear positive association at RHR ≥75 bpm (figure 2). In contrast, RHR showed strong positive and apparently log-linear association with risk of incident PHD throughout the range studied (figure 2).

Associations of fifths of RHR with heart failure and pulmonary heart disease. Models were adjusted for measured confounders (season, sex, socioeconomic status (education, household income and marital status), lifestyle (physical activity, smoking and alcohol consumption), body mass index, hypertension and diabetes mellitus) and stratified by age and region. The HR of HF or PHD for each fifth of usual RHR were compared with those in the lowest fifth. The black squares and the vertical bars are adjusted HR and 95% CI. The numbers above and below the vertical bars represent the adjusted HR and number of events in each quintile, respectively. The black squares were weighted by the number of events in each fifth. HF, heart failure; PHD, pulmonary heart disease; RHR, resting heart rate.
Figure 3 shows the effect of sequential adjustment for potential confounding factors on the strength of the associations of RHR with HF (top panel) or PHD (bottom panel). After correction for regression dilution bias, each 10 bpm higher usual RHR was associated with a 25% (1.25; 95% CI 1.17 to 1.34) higher risk of HF for RHR for 75 bpm or greater (figure 3). The strength of the association of RHR with HF was approximately halved after adjusting for confounding due to hypertension and diabetes (as demonstrated by a 50% reduction in the χ21 from 83.4 to 41.3). For PHD, each 10 bpm higher usual RHR was associated with a 74% (1.74; 1.67–1.81) higher risk of PHD (figure 3). In contrast with HF, the strength of the association of usual RHR with PHD was largely unaltered by sequential additional adjustment for confounding factors (16.7% reduction in χ21: figure 3).
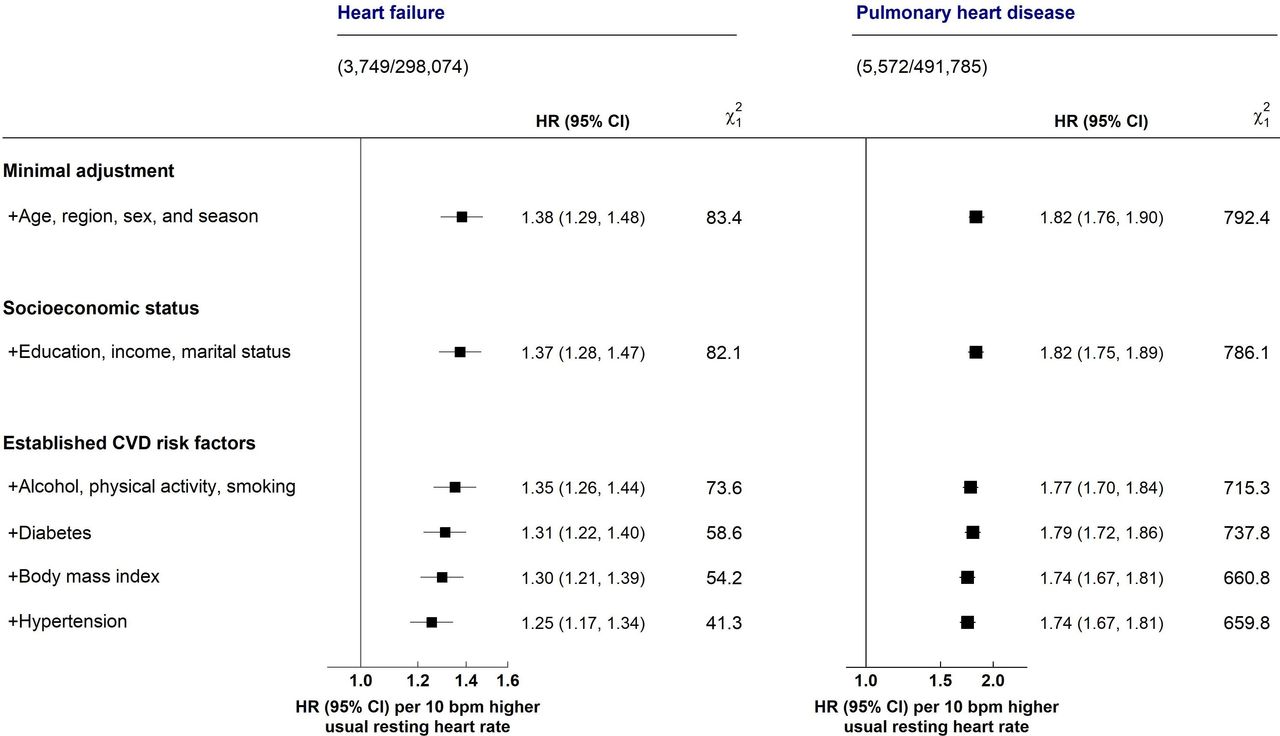
HRs (95% CI) of heart failure and pulmonary heart disease associated with 10 bpm higher RHR before and after adjusting for confounding factors. The squares represent the adjusted HR of HF or PHD per 10 beats per unit (bpm) higher usual RHR. Symbols and conventions as in figure 2. In the left panel, the analyses were restricted at a usual RHR ≥75 bpm, where the shape of the association of usual RHR with HF was approximately linear. CVD, cardiovascular disease; HF, heart failure; RHR, resting heart rate.
The risks of HF and PHD for each 10 bpm higher usual RHR varied substantially in different subgroups (figure 4). The strengths of the associations of usual RHR with HF were weaker among participants with hypertension and higher BMI, whereas for PHD, they were stronger among ex-smokers, at younger age and in those without diabetes (figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
HRs (95% CI) of heart failure and pulmonary heart disease associated with 10 bpm higher resting heart in different population subgroups. Models were adjusted for measured confounders. The unshaded diamond and dashed vertical line represent the overall adjusted HR for the main model, while the solid vertical line represents the line of no effect.
Online supplemental figure 1 shows the shapes of the associations of fifths of usual RHR with HF and PHD after excluding participants with prior diseases. Table 2 shows the HR (95% CI) of HF and PHD associated with 10 bpm higher RHR after excluding participants with prior diseases. For both HF and PHD, excluding individuals with non-vascular diseases significantly attenuated the associations, while the converse was true after excluding those with prior stroke or BP-lowering medications. Exclusion of non-vascular diseases at baseline reduced the strength of the association of RHR with HF and PHD by about 50% but did not materially change the shape of the associations (online supplemental figure 1 and table 2). In addition, excluding the HF events after a diagnosis of PHD attenuated the association of RHR with HF (table 2 and online supplemental figure 1). However, excluding events occurring during the first 5 years of follow-up did not materially alter the associations.
HRs (95% CI) of heart failure and pulmonary heart disease associated with 10 bpm higher resting heart rate after excluding participants with prior diseases
Discussion
This large prospective study in China demonstrated striking differences in associations of RHR with left and right HF. For left HF, there were J-shaped associations of RHR with HF, with the modestly strong positive associations evident only at RHR >75 bpm. Moreover, further adjustment for established CVD risk factors and exclusion of prior non-vascular diseases greatly attenuated the associations towards the null. In contrast, RHR showed strong log-linear positive associations with risks of PHD throughout the range of RHR studied, which were largely unaffected by further adjustment for CVD risk factors. Among participants with RHR >75 bpm, each 10 bpm higher usual RHR was associated with a 25% higher risk of HF but was associated with a 74% higher risk of PHD throughout the range studied.
Previous studies in Western populations have reported that higher RHR was associated with a higher risk of HF in healthy adults and in patients with heart disease or hypertension in both middle-aged and older adults.16 28–32 The results of the present study are consistent with those of previous studies in Western populations that reported that higher levels of RHR were only a modest risk factor for HF but a stronger risk factor for PHD.29 30 The strength of associations of RHR with HF differed by levels of established CVD risk factors and was stronger among individuals with versus without obesity and hypertension.
The present study highlights the importance of adjusting for confounding by levels of established CVD risk factors when assessing the associations of RHR and HF. Consistent with previous reports, approximately half of the association of RHR with HF was accounted for by hypertension, adiposity and diabetes. Moreover, the present study highlights the importance of reverse causality as the strength of the associations were attenuated after excluding participants with prior non-vascular diseases and individuals with poor self-reported health at baseline. However, the strength of the associations between RHR and PHD was not attenuated after adjustment for confounding factors to the same extent as with HF after adjustment for confounding factors, suggesting that confounding factors were less important for PHD than for HF.
HF is a disease of insidious onset and has a progressive course, with an early asymptomatic stage followed by a progressive reduction in cardiac function and a corresponding increase in heart rate due to activation of the sympathetic nervous system.32 The analyses sought to minimise the effects of reverse causality by excluding participants with a prior history of coronary heart disease or rheumatic heart disease or the use of beta-blockers at baseline. Additional exclusions of participants with prior non-vascular disease and individuals with self-reported poor health substantially attenuated the strength of the associations of RHR with HF by over 50%.
The association of RHR with PHD could possibly reflect some dysfunction of the sympathetic nervous system and related peripheral chemoreceptors in response to the vasodilatory effects of hypoxaemia. Increased sympathetic nerve activity could result in elevated RHR, increased stroke volume and systemic vasoconstriction.2 33 Prolonged chronic vasoconstriction of the pulmonary arteries and increased cardiac output could result in right ventricular remodelling and failure.
While the study, involving a large number of cases, demonstrated precision in the strength of the associations with both right and left HF, it also had some important limitations. Participants were not advised to avoid smoking or consumption of tea and coffee before examination. Even though the associations between RHR with HF and PHD were corrected for regression dilution bias, it was not possible to correct for within-person variability in covariates.34 Moreover, due to the large size of the study, it was not feasible to collect data on heart rhythm at baseline in the CKB. Furthermore, it was not possible to classify HF and PHD by major subtypes as medical records providing details of the diagnostic criteria for major subtypes were not available in CKB. Consequently, we cannot exclude the possibility of some misclassification, as cases of HF and PHD in the CKB were not validated at the time of this analysis. Moreover, we were unable to refute the possibility of some misclassification of COPD as PHD, as both diagnoses are difficult to distinguish in clinical practice. In addition, it is possible that there was some misclassification from failure to diagnose mild cases of HF and PHD. Likewise, it was not possible to fully exclude the possibility of residual confounding (eg, systematic inflammatory markers and use of beta-adrenergic stimulators) and unknown confounders on the associations of RHR with HF and PHD. Finally, the findings of this study cannot be generalised to the Chinese population, as the CKB is not representative of the Chinese population.
Conclusion
Higher levels of RHR (above 75 bpm) were only modestly and positively associated with higher risks of HF, but were much more strongly associated with higher risks of PHD (across the full range of RHR). This study suggests that RHR may be more strongly associated with right rather than with left HF. RHR is a potentially important modifiable risk factor for HF, since measurements of RHR are readily accessible for both patients and healthcare workers. While use of medication to control heart rate has been shown to reduce hospitalisation and death among selected patients with HF, the relevance of medication or other strategies to control heart rate for prevention of incident HF or PHD is uncertain. The findings of the present study imply that reducing high levels of RHR could significantly reduce morbidity and mortality associated with HF and PHD at a population level. However, further research is needed to assess the causal relevance of the observed associations between RHR with HF and PHD and clinical relevance of using RHR to predict individuals at high risk of HF or PHD based on their RHR.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Ethical Review Committees of the Chinese Centre for Disease Control and Prevention and the Oxford Tropical Research Ethics Committee. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors acknowledge the participants, CKB project staff, staff of the China CDC and its regional offices for access to death and disease registries. The Chinese National Health Insurance scheme provided electronic linkage to all hospital admissions. The China Kadoorie Biobank study is jointly coordinated by the University of Oxford and the Chinese Academy of Medical Sciences.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
YC and RC contributed equally.
ZC and DB contributed equally.
Collaborators Members of the China Kadoorie Biobank Collaborative Group are shown in the online supplemental appendix.
Contributors VNA, YC, RC and DB designed the study. VNA performed the data analyses and wrote the first draft of the manuscript. YC, RC, ZC and DB provided critical comments on the manuscript. RC, LL and ZC, as members of the CKB Steering Committee, designed and supervised the conduct of the study. YC, YG, JL, CY and ZC coordinated the data acquisition. All authors provided comments on the final version of the manuscript. RC, YC and DB are guarantors for this report.
Funding The funding body for the baseline survey was the Kadoorie Charitable Foundation, Hong Kong, China and the funding sources for the long-term continuation of the study include UK Wellcome Trust (202922/Z/16/Z, 104085/Z/14/Z, 088158/Z/09/Z), Chinese National Natural Science Foundation (81390540, 81390541, 81390544) and the National Key Research and Development Program of China (2016YFC0900500, 2016YFC0900501, 2016YFC0900504, 2016YFC1303904). Core funding was provided to the CTSU, University of Oxford, by the British Heart Foundation, the UK Medical Research Council and Cancer Research UK. VNA’s graduate study was supported by a Nuffield Department of Population Health studentship (Reference number: Ref. MSD1920_ 1140683).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.