Article Text

Abstract
Objective Severe decompensated aortic valve stenosis is associated with noticeable reduction in survival. Until recently the options for such patients were either high-risk surgery or percutaneous balloon valvuloplasty and medical therapy which does not add any survival benefits and associated with high rate of complications. We present our experience in the use of transcatheter aortic valve implantation (TAVI) in patients with decompensated severe aortic stenosis requiring urgent intervention in the same hospital admission.
Methods In this observational study, all patients who were admitted with decompensated severe aortic stenosis were enrolled. Elective patients were excluded from the study. Perioperative records were analysed and clinical, echocardiographic and survival data were presented.
Results 76 patients with a mean age of 81±6 years were enrolled. All patients presented with New York Heart Association (NYHA) IV status. Femoral approach was performed in 86.8%. Median postoperative hospital stay was 6 days and intensive care unit admission rate was 15%. At follow-up, 61.8% of patients were in NYHA status I/II. Moderate or more paravalvular leak occurred in 5.2% of patients. Permanent pacemaker was required in 14.4% of patients. The incidence of in-hospital death was 2.6%. Kaplan-Meier analysis indicated a survival rate of 81% at 1 year.
Conclusions Urgent in-hospital TAVI is feasible as the first-line treatment in decompensated severe aortic stenosis. In our cohort, it showed to be safe and achieved satisfactory survival rates and symptom control.
- minimally invasive
- surgery-valve
- aortic valve disease
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See:http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Transcatheter aortic valve implantation (TAVI) is indicated in high-risk surgical patients with prohibitive surgical risks. It is a lab-based catheter-guided placement of aortic bioprosthetic arotic valve under general anaesthesia or sedation. Currently, this technique is also being assessed in the use in patients with moderate surgical risks.
To our knowledge, there are no reports of the use of TAVI in urgent patients who presented with decompensated heart failure due to severe aortic stenosis in the same hospital admission.
What does this study add?
This study examined the use of TAVI in patients with decompensated heart failure as a mean of urgent procedure and relieve of heart failure.
In this study, the preoperative presentation and clinical outcomes of using TAVI in urgent setting to relive decompensated heart failure with severe aortic stenosis will be discussed.
How might this impact on clinical practice?
The outcomes of this cohort study showed positive results when TAVI is used in urgent setting in relieving heart failure in patients with high risk of death otherwise with medical therapy or open heart surgery.
There was lower risk of mortality and postprocedural complications compared with medical therapy or open heart surgery when compared with the literature.
This study will encourage the specialist teams to expand the use of TAVI beyond the elective settings only to more urgent/acute use.
Introduction
Aortic valve stenosis (AS) is associated with high risk of mortality and morbidity, once the symptoms of angina, syncope or heart failure develop; over two-thirds of patients will die within 3 years.1 Until recently, the options for patients with heart failure due to severe decompensated AS has been either surgery which carried a high risk of perioperative mortality of more than 20% or percutaneous balloon aortic valvuloplasty (PBAV) which was shown to add no survival benefits and was also associated with high rate of complications and death.2–4 Transcatheter aortic valve implantation (TAVI) is an established technique in patients with high prohibitive surgical risks.5 The role of TAVI in the management of patients who require aortic valve replacement (AVR) but not fit to undergo open heart surgery is becoming more established.6 This study assessed the early outcomes of TAVI procedure in patients who presented with severe decompensated heart failure due to severe aortic stenosis necessitate urgent in-hospital intervention within the same admission.
Methods
In this observational study, all patients admitted with decompensated severe aortic stenosis between January 2015 and October 2016 to our Heart and Lung centre were enrolled. Elective patients not in failure or patients who did not receive TAVI procedure were excluded. In our unit practice, all patients including elective patients with severe left ventricular (LV) dysfunction (ejection fraction (EF) <30%) with no evidence of myocardial viability on testing received PBAV initially as a bridge to TAVI procedure if they showed symptoms improvement with PBAV. These patients were also excluded from this study.
All the patients presented as urgent with New York Heart Association (NYHA) class IV and were stabilised initially with heart failure medical therapy and aggressive diuresis to improve the cardiac failure symptoms. They were then rigorously assessed by a specialised TAVI team and relevant initial investigations acquired including blood tests, troponin levels, chest radiograph, echocardiography and coronary angiography when indicated.
The diagnosis of severe aortic stenosis was defined based on echocardiography according to the 2014 American Heart Association/American College of Cardiology guidelines with a mean pressure gradient across the aortic valve of ≥40 mm Hg, jet velocity of ≥4 m/s and aortic valve area of <1 cm2.7 A TAVI protocol CT scan which includes the aorta and distal arteries with 3D reconstruction using Phillips IntelliSpace PACS software (USA) was performed in preparation for the procedure when feasible.8 Our preferred delivery route is the peripheral femoral approach, however, based on the CT testing prior to the procedure those with contraindications to femoral approach (iliac artery calcification, distal aortic stenosis) received a different approach. Types of valve and size were discussed among the TAVI team. When aortic valve intervention is indicated, the option of TAVI procedure or open heart surgery was discussed at specialised multidisciplinary meeting including the cardiac surgeons, non-interventional cardiologists and TAVI team. Patients’ relevant investigation, diagnosis, frailty and comorbidities were assessed. TAVI was considered more suited for patients with prohibitive surgical risks.
The patients were also assessed by a TAVI anaesthetic team and the mode of anaesthesia (local anaesthetic with sedation or general anaesthesia) was discussed with the patient and finalised.
Postprocedure, the patients were managed on the coronary care unit with few patients requiring intensive care admission. All patients had serial ECGs and assessed for the need of permanent pacing. They received daily physiotherapy treatments as required.
Data collected included demographic information, other diagnosis, approach and size of the valve implanted, NYHA status, creatinine levels, LV function, intensive care unit admissions, length of hospital stay, the need for postprocedural dialysis, the need for permanent pacemaker, aortic paravalvular regurgitation and mitral valve regurgitation, cerebrovascular event, acute renal failure and survival data.
Poor LV function was defined by and EF of <30%, moderate of 30%–49% and normal of ≥50%. Acute renal impairment was defined by new raise in creatinine within the first 7 days after the procedure to ≥200 mmol/L.
Follow-up consisted of both echocardiogram test at regular intervals from second postprocedural months and every 6 months thereafter and clinical assessment in the outpatient clinic in regard to the patients’ NYHA and Canadian Cardiovascular Society status if applicable.
Statistical methods
Results are expressed in percentage for categorical variables and median (range) for non-normally distributed continuous variables. Parametric data are expressed as mean (SD).
Kaplan-Meier survival analysis was used to assess the survivorship after the procedure. All analyses were performed using the SPSS statistical package V.21.0.9
Results
During the study period, 76 patients underwent TAVI for decompensated severe aortic stenosis. AS was newly diagnosed in 85% of patients. All patients were admitted with NYHA IV status; other patients’ characteristics are displayed in table 1. The mean age was 81±6.8 years, 50% were males. Median logistic Euroscore was 19 (range 2.7–63). Preprocedural poor LV function was present in 25% of patients. All patients had severe aortic stenosis; none had significant aortic regurgitation.
Preoperative patients’ characteristics
The majority of valves were deployed utilising the percutaneous femoral approach (84%).
The most common valve size used was 29 mm (33%) (table 2). Various valve types were used include Lotus (57%), Corevalve (11%), Evolute-R (31%) and Engalger Transapical (1%).
Distribution of valve sizes used
Postprocedural hospital length of stay was 6 (2–32) days and intensive care admission rate was 15%. Complications included acute renal failure (5.3%), permanent pacemaker (14.5%), cerebral stroke (2.6%) and vascular injury (9.2%).
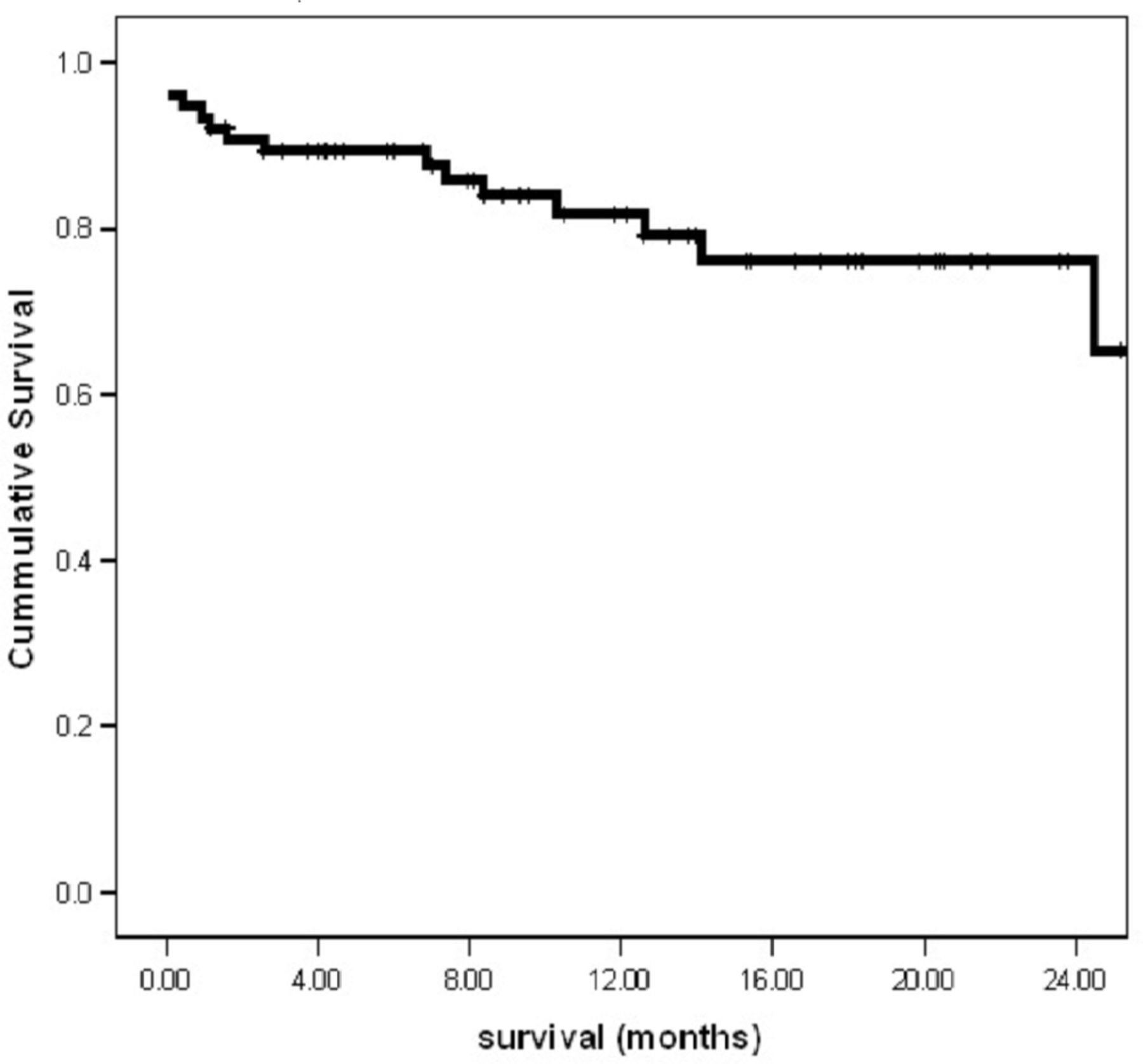
Survival data revealed in-hospital rate of death of two patients (2.6%, cause of death was pneumonia in one patient and cerebral haemorrhage on day 4 after TAVI in another), death at follow-up (9 (min 3–max 41) months) of 14 patients (18%), out of which 42% were cardiac-related deaths; median time from procedure to death was 7.8 months (table 3). Kaplan-Meier analysis indicated survival rate of 81% at 1 year (figure 1).
Time from TAVI to death (months)

{kind=link}
Kaplan-Meier survival for patients with decompensated aortic stenosis who underwent transcatheter aortic valve implantation treatment.
In this series, we achieved complete echocardiographic and clinical follow-up. A total of 94.8% of patients had mild or less degree of aortic paravalvular regurgitation. Mean gradient across the aortic valve was 9.8 mm Hg (±6.6) with area of 1.57 cm2. At follow-up, moderate or more LVEF was present in more than 80% of patients, NYHA II status or less was achieved in 61.8% and 22.3% were in class III. Seven per cent of patients who were admitted with poor LV function improved to moderate or more, and 8% who were admitted with moderate LV improved to good LV function on echocardiographic data but this was not statistically significant. Improvement was also noticed in NYHA status at follow-up (table 4). For patients group who were admitted with EF <30% perioperatively, there were no in-hospital death, had a median length stay of 5.5 days and 1-year survival rate of 70%. One patient in this group remained in NYHA stage IV.
Preprocedural and postprocedural left ventricular (LV) function and New York Heart Association (NYHA) status
Discussion
In our cohort, urgent inpatient TAVI for decompensated severe AS showed good outcome and symptom relief. Aortic stenosis is a malignant disease with dreadful outcomes if not addressed. In their landmark paper, Ross and Brauwald examined the natural history of symptomatic aortic stenosis. They illustrated a dramatic increase in mortality with mean survival of 5 years at best and up to two-thirds of patients with symptoms die within 3 years.1 In severe symptomatic aortic stenosis, the 1-year and 2-year survival rates for patients who did not have AVR because the physicians deferred the procedure or the patients declined was 57% and 37%, respectively.10 Survival rates of patients with severe AS and low LVEF if the valve was not addressed at 1 and 4 years has been reported to be as low as 41% and 15%, respectively. AVR shown to be the main significant factor of improvement of survival in this group.11
Until recently, the option for patients with decompensated severe aortic stenosis who have prohibitively high risk of surgery has been the use of PBAV as a palliative measure. Leiberman and his colleagues examined the results of PBAV in 165 patients and showed a median 1-year and 2-year survival of only 64% and 48%, respectively. Their rate of major events including repeat PBAV, aortic valve surgery or death was 58% and 81% at 1 and 2 years, respectively. In a subgroup of their patient population, class IV congestive heart failure, similar to our patient cohort, was associated with increased risks of major cardiac event. When the authors compared the group of patients who eventually went on to have aortic surgery, 1-year survival improved to 83% (AVR group) compared with 48% in the PBAV group alone.3 Significant risk of mortality with PBAV was also similar in various reports reaching up to 87% at 2 years after PBAV with short median survival period of 6.6 months.12–14 When these figures are examined closely, the rate of survival among patients who received PBAV for severe decompensated AS is not notably different from those who received medical therapy alone.3 10 15 In their prospective registry study comparing surgical AVR, TAVI and PBAV in high-risk patients, the authors concluded that the use of PBAV is not different to medical therapy alone and this group was associated with higher risk of mortality compared with AVR or TAVI groups. In their cohort, 10% and 4.8% received PBAV as a bridge therapy in the TAVI and AVR groups, respectively. The authors also concluded that the use of PBAV is associated with high risk of complications and the use of this procedure as a bridge to surgical AVR/TAVI added no benefits.4
TAVI is becoming more recognised worldwide, especially in the high-risk groups. In their randomised trial, Kapadia and colleagues compared the use of TAVI with medical therapy in high-risk operative group and showed significant benefit in survival and symptoms in favour for the TAVI group. Their median survival rate was also significantly longer (31 vs 11.7 month).5 Similar results were highlighted when surgical AVR was compared with PBAV.3 In high-risk patients, TAVI can offer a real solution to the patients’ illness with much less risks to life compared with open heart surgery.
The patients in this study represent those who were unwell, have multiple comorbidities and presented acutely with congestive heart failure. Given the evidence of PBAV and medical treatment alone on survival and symptom control, TAVI was an obvious option we applied in our unit to treat such group who would otherwise have poor chance of survival. This cohort of patients presented with NYHA IV status as an emergency and having the opportunity to undergo TAVI has given them the benefit of survival and relive of their symptoms with the majority having NYHA II status or less at follow-up. Kapadia and colleagues also demonstrated significant symptomatic benefit when compared their TAVI group with standard best medical therapy alone in those at high risk of open heart surgery. This is also true for hospital readmissions due to cardiac disease.5
TAVI is a fast-growing technology with increasing safety and technique of valve implantation offering similar results and rate of complications for patients undergoing the procedure urgently or electively.6 TAVI thus can offer a real solution and benefit in survival and symptoms for critical patients who present with acute decompensated aortic stenosis and deemed unfit to undergo open heart surgery giving them the best and arguably the safest option of managing their illness. Given the availability of an effective and safe technique as TAVI, PBAV should be left as a secondary alternative option and last resort.
Limitations
In this article, we presented a full data at follow-up with robust echocardiographic data; however, several limitations still exist. This is a non-randomised study with short follow-up period. The types of TAVI valves used were not preselected and hence a bias in favour to any specific type of valve particularly in regard to haemodynamic performance cannot be ruled out. Although in this article we showed that the improvement of patients’ symptoms is of utmost importance for these patients who present with this debilitating disease and the results are promising, but postprocedural symptoms and exercise limitations were assessed during outpatients’ clinic consultations based on patients reports and feedback and no formal objectives testing were undertaken to determine the patients’ accurate exercise status.
Conclusion
TAVI is a useful and feasible treatment strategy in patients presenting with heart failure resulting from decompensated severe aortic stenosis. When compared with historical data on medical therapy alone, surgical AVR or PBAV in similar group of patients, TAVI seems to be associated with less risk of death and complications. Further studies with longer follow-up and direct comparison between groups are needed to accurately examine the degree of survival benefit that can be achieved.
Acknowledgments
We would like to express our gratitude to all staff (nurses, perfusionists, para-medical staff, junior doctors, anaesthetists and surgeons) of the cardiothoracic surgical and cardiology unit of the Heart and Lung Centre, Wolverhampton, UK, for their help and support with our TAVI program.
References
Footnotes
Contributors MA contributed to planning, data collection, statistical analysis and writing up of the manuscript. HL contributed to planning, reporting of the work and writing the manuscript as well as review of the manuscript. SK, JMC, AM and MM contributed to planning, review of the article and perioperative data. MA and HL were responsible for the overall content of the article.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.