Article Text

Statistics from Altmetric.com
Hellen Taussig persisted despite dyslexia, deafness and gender discrimination. In 1924, she was one of the 10 women accepted to Johns Hopkins School of Medicine and later led development of the Blalock-Taussig-Thomas shunt and founding of paediatric cardiology. In 1965, she became the first woman president of the American Heart Association (AHA), 41 years after its foundation. More than 50 years later, in 2020, a truly historic moment took place when 10 women were elected as presidents of major cardiovascular societies. The field of cardiology has been traditionally dominated by men. Despite women’s significant contributions to patient care and research in cardiology, their disproportionate under-representation compared with other fields of medicine has led to a significant gap in recruitment and promotion. This, however, appears to be slowly changing as the heightened awareness of the need to attract more women to cardiology has led to a slight increase in the number of women in cardiology (WIC). The WIC committees of AHA and the American College of Cardiology (ACC) have played critical roles in leading these efforts to address gender inequities in cardiology, aiming to create an inclusive and diverse workforce. We interviewed some women leaders in cardiology and asked them about the gaps and barriers as well as the opportunities to overcome these inequities to strengthen the representation of WIC.
What do statistics tell us about WIC?
According to the 2020 Physician Specialty Data Report, only 15% of adult cardiologists are women, and cardiology is ranked 39th of 47 specialties in the percentage of women. While there has been a significant increase in the percentage of women in internal medicine subspecialties, cardiology had one of the lowest growth rates. In 2016, only 21% of cardiology fellows were women as opposed to 60% of rheumatology fellows.1 Only 4% of interventional cardiologists in 2016 were women. A survey of ACC fellows in training found that the very low percentage of women in interventional cardiology is largely related to the culture of interventional cardiology.2 Over the last decade, there has also been a steady rise in the overall proportion of women as full-time faculty in academic medicine, department chairs and medical school deans. Cardiology, however, lags behind other internal medicine specialties with regard to women achieving leadership positions. In a 2014 analysis, women were less likely than men to be full professors after accounting for several factors known to influence faculty rank.3 While there were more women in the programme director position in 2019 as compared with 1992, only 5% of division chiefs were women, and their representation in this position has not changed since 1992.4
Barriers for women in entering cardiology
There is a general perception of incompatibility of cardiology with family life and female gender. Cardiology employment and career models have been led, designed and formulated by men with androcentric approaches, resulting in the lack of flexibility of current work models, call schedules and hours for life–work balance and family. Dr Biykem Bozkurt, immediate past president of the Heart Failure Society of America, professor and chair of internal medicine and vice chair of the department of medicine at Baylor College of Medicine, believes some barriers are the lack of women leaders as role models, mentors and sponsors; lack of equity for promotion and compensation; lack of support for women in the workforce in cardiology; and historical bias and discrimination against women. Dr Cindy Grines, immediate past president of the Society for Cardiovascular Angiography and Interventions, highlights the misperception regarding the risk of radiation exposure and lack of flexibility in schedules and calls in cardiology not allowing a work–life balance during fellowship and post-training practice. The perception that women cannot handle the challenges of the rigorous cardiology training and the demanding career that follows tops the list of barriers according to Dr Linda Gillam, chair of cardiology at Morristown Medical Centre. Dr Jennifer Mieres, past president of the American Society of Nuclear Cardiology (ASNC), professor of medicine and the associate dean of faculty affairs at the Zucker School of Medicine of Hofstra/Northwell, highlights the ACC workforce survey which identified five contributors to the negative perception of cardiology as a career for women: (1) family concerns, (2) occupational radiation, (3) discrimination, (4) disparity in compensation and (5) lack of career advancement. Dr Mieres adds bias, sexual harassment, lack of institutional support and inadequate workplace support for pregnant and nursing women cardiologists. According to Dr Sharmila Dorbala, ASNC immediate past president and professor of radiology at the Harvard Medical School, the most obvious barrier is that the male-dominated cardiology field requires a long period of training with a perception of extended work hours, at a time of life when career and reproductive biology compete. The perceived long duration of training in cardiology as well as relatively limited exposure to cardiology and, in particular, outpatient cardiology in medical school have been found to be among the main reasons for few women being attracted to the field.5 An ACC survey revealed that WIC are significantly more likely than male peers to remain single or to refrain from having children due to challenges related to child care, family leave policies, and professional and wage discrimination that impede their advancement.6 Dr Roxana Mehran, professor of medicine and director of interventional cardiovascular research at Mount Sinai School of Medicine, believes that the strongest barrier is the culture. It is often said that cardiology is an ‘old boys club’. When this is the prevailing culture, women not only feel they do not have a place but also are repelled from the specialty. Finally, Dr Toniya Singh, immediate past chair of the ACC WIC Section, adds the lack of diversity in cardiology to the list of barriers. A recent ACC global survey demonstrated a high prevalence of hostile work environments in cardiology. Hostile work environment is experienced more by women as compared with men and by Black race as compared with other races.7
Filling the leaky pipeline
In order to fill the pipeline, Dr Gillam suggests that we start in high schools and colleges to advocate that cardiology provides a number of options for a rewarding and interesting career, and to identify and ensure leadership opportunities for women to serve as role models and create mentoring networks for trainees and early careers. Dr Mieres believes that recruiting and retaining WIC have to be incorporated into the mission and strategy of the cardiology community. She provides the example of the model for career advancement established in 2017 at University of Pennsylvania with the goal of promoting the recruitment, retention and advancement of WIC. Dr Singh underlines the work done by the ACC WIC Section on some of the solutions for the aforementioned issues: showing medical students and residents that there are many different ways cardiology is practiced; addressing the concerns about radiation safety through education; and working with programme directors to design better parental leave guidelines. More flexible work choices are important in allowing women to remain engaged and successful during their careers, which would allow them to advance in their career and reach leadership positions. Dr Dorbala believes that to encourage more women to enter cardiology, we need to institute flexible training policies, provide lactation and child care support for new mothers, measure objective data about wages and advancement of WIC, and educate peers about implicit bias and family members on the rigours of the field. Women cardiologists must also serve as experienced role models for residents and fellows who can demonstrate that, with the needed support structure, a career in cardiology is as feasible as any other career. In Dr Mehran’s opinion, the cardiology culture needs to shift, and this starts at the leadership level: not condoning foul language in the workplace, encouraging both men and women to take parental leave, and actively showcasing an environment where respect is paramount. A 2019 publication from the ACC WIC Section provided a roadmap and strategy to enhance recruitment, retention and career advancement for WIC.8
Improving inclusion and support of WIC
There remains a lack of diversity in the cardiology workforce both in terms of gender and ethnicity. Despite the fact that 32% of the US population is characterised by under-represented minorities including Black people and Hispanics, only about 12% of adult cardiology fellows represent these minorities. According to Dr Dorbala, the inclusion of WIC is vital to improving all aspects of cardiology, including patient care, culture of the workplace and the lives of all cardiologists. She believes that a host of workplace reforms must ensure equal opportunity for women cardiologists and trainees. In the realm of medical training, chiefs of medicine need to actively encourage women residents interested in cardiology, and cardiology programme directors need to proactively select highly qualified candidates, irrespective of gender. Chiefs of cardiology need to strongly advocate for women trainees and WIC in all aspects of work/life, including hiring practices, the implementation of family-friendly policies, as well as the inclusion and promotion of women of colour and under-represented minorities. Compensation gap is another key area that must be immediately and proactively addressed. Dr Dorbala suggests that professional organisations as well as journals must include women, specially early career women, on par with men, in committees and activities. While Dr Mehran believes that women need to see representation of WIC, women-only events should not be considered as the sole answer. To truly improve the inclusion and support of WIC, women should be given substantive opportunities to be seen, heard and resourced for success. As the cofounder of the Women as One organisation, Dr Mehran provides the Women as One organisation as an example where this is happening. Creating equal opportunities for women cardiologists and trainees requires measuring their engagement, inviting them to give lectures and grand rounds, providing them leadership roles, promoting them academically, and honouring their leadership and achievements so they can serve as role models for future generations. Finding mentors and sponsors is a very important way of introducing trainees and early career women to people in leadership who can then help them craft their path. Leaders who can advocate on their behalf as well as leaders who can work on structural issues such as lack of transparency and flexibility in their institutions are also important to foster an environment in which women can advance their careers and thrive.
Women leaders are changing the face of cardiovascular medicine, improving the male-dominant culture of cardiology, reducing the inequities in the workplace and challenging our professional entities, including academia, industry, and professional and clinical research organisations to continue Taussig’s legacy, and demonstrating that our diversity is our strength (figure 1).
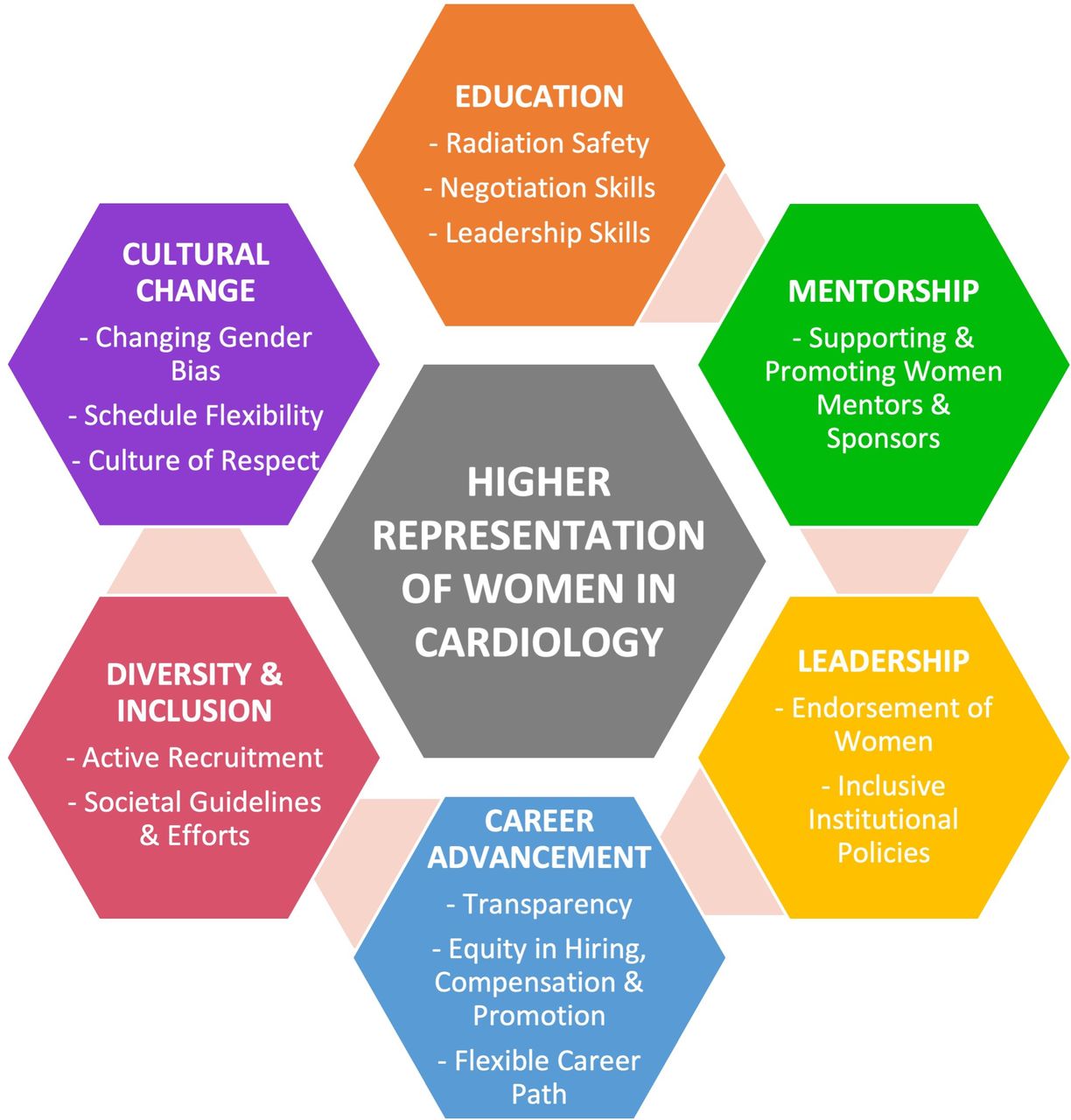
{kind=link}
Six pillars of higher representation of women in cardiology.
Ethics statements
Patient consent for publication
Footnotes
Twitter @coronarydoc, @rbp0612, @bravo__md, @BiykemB, @dorbalasharmila, @lindagillammd, @drcindygrines, @Drroxmehran, @drjmieres, @drtoniyasingh, @nanettewenger
Contributors All authors listed have contributed sufficiently to the manuscript. All authors have read and approved the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.