Article Text

Abstract
Background Coronary artery aneurysms (CAAs) are increasingly diagnosed on coronary angiography; however, controversies persist regarding their optimal management. In the present study, we analysed the long-term outcomes of patients with CAAs following three different management strategies.
Methods We performed a retrospective review of patient records with documented CAA diagnosis between 2000 and 2005. Patients were divided into three groups: medical management versus percutaneous coronary intervention (PCI) versus coronary artery bypass grafting (CABG). We analysed the rate of major cardiovascular and cerebrovascular events (MACCEs) over a period of 10 years.
Results We identified 458 patients with CAAs (mean age 78±10.5 years, 74.5% men) who received medical therapy (N=230) or underwent PCI (N=52) or CABG (N=176). The incidence of CAAs was 0.7% of the total catheterisation reports. The left anterior descending was the most common coronary artery involved (38%). The median follow-up time was 62 months. The total number of MACCE during follow-up was 155 (33.8%); 91 (39.6%) in the medical management group vs 46 (26.1%) in the CABG group vs 18 (34.6%) in the PCI group (p=0.02). Kaplan-Meier survival analysis showed that CABG was associated with better MACCE-free survival (p log-rank=0.03) than medical management. These results were confirmed on univariate Cox regression, but not multivariate regression (OR 0.773 (0.526 to 1.136); p=0.19). Both Kaplan-Meier survival and regression analyses showed that dual antiplatelet therapy (DAPT) and anticoagulation were not associated with significant improvement in MACCE rates.
Conclusion Our analysis showed similar long-term MACCE risks in patients with CAA undergoing medical, percutaneous and surgical management. Further, DAPT and anticoagulation were not associated with significant benefits in terms of MACCE rates. These results should be interpreted with caution considering the small size and potential for selection bias and should be confirmed in large, randomised trials.
- coronary artery disease
- coronary aneurysm
- coronary vessels
- percutaneous coronary intervention
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Coronary artery aneurysms (CAAs) are increasingly being diagnosed on coronary angiography. However, there is paucity of data regarding the long-term outcomes of different management strategies in patients with CAA.
What does this study add?
Our study analysed the long-term MACCE outcomes of patients with CAAs who underwent medical management versus percutaneous and surgical interventions.
How might this impact on clinical practice?
Our results will inform clinical decisions regarding the selection of management strategies for patients with CAA and the role of antiplatelet/anticoagulant therapy in this patient cohort.
Introduction
The incidence of coronary artery aneurysms (CAAs) varies from 0.3% to 5.3%.1 In most cases, CAAs are asymptomatic. However, when symptomatic, the clinical presentation varies and is typically dependent on the underlying cause, for example, atherosclerotic coronary artery disease (CAD). More than 80% of CAAs are atherosclerotic in origin.2 3 Other causative factors include Kawasaki disease, connective tissue disorders, congenital anomalies, infection, specific drug reactions, trauma or iatrogenic interventions.4 Potential complications of CAAs include thrombosis, rupture and embolism, which can precipitate ischaemia or even sudden death.5
The management strategies of CAAs include medical (conservative) therapy, percutaneous coronary intervention (PCI) and surgery. To date, there is no consensus on the optimal management of CAAs. This is because the natural history and long‐term outcomes of CAAs remain unclear. In the lack of large randomised clinical trials, current recommendations are primarily based on small studies and anecdotal evidence. Further, controversies persist regarding the benefits of anticoagulant and dual antiplatelet therapy (DAPT) in this patient population.6 7 In this retrospective cohort study, we analysed the long-term major cardiovascular and cerebrovascular event (MACCE) outcomes of patients with CAA who were managed conservatively versus those with PCI or surgical intervention over a 10-year follow-up period.
Methods
Patient population
This was a single-centre, retrospective cohort study at the Cleveland Clinic. All patients whose cardiac catheterisation reports documented a diagnosis of CAA between 2000 and 2005 were included in the present study. CAA was defined as a localised dilatation of coronary vascular lumen with diameter >1.5 times compared with the reference coronary vessel. Patients reported to have ‘ectasia’ (diffuse dilatation of the coronary vessel) and those with no recorded follow-up after the initial catheterisation were excluded from the study. The study was reported according to the guidelines of the Strengthening and Reporting of Observational Studies in Epidemiology Statement checklist.8
Data collection
All patients who underwent coronary arteriography between 2000 and 2005 were eligible. A total of 74 269 consecutive cardiac catheterisation reports were searched for the word ‘aneurysm’. This strategy retrieved 3333 catheterisation reports, which were further evaluated to exclude patients with aortic, ventricular and sinus of Valsalva aneurysms. A total of 498 patients matched our inclusion criteria; however, 40 patients were further excluded due to incomplete chart information or lack of follow-up after the initial catheterisation (figure 1).

Patient selection flow diagram. Flow diagram depicting the inclusion and exclusion criteria for selection of patients with coronary artery aneurysm.
The baseline patient characteristics, aneurysm anatomical details, and outcomes were collected by a thorough review of individual medical charts and cardiac catheterisation images. Mortality data were obtained from multiple sources in an additive manner, including the Social Security Death Index, State Death Index and public record searches. For patients who did not have any date of death on record, the date of last known follow-up was used as the censor date.
Outcome definitions
The primary MACCE endpoint was a composite of all-cause death, stroke, unplanned percutaneous or surgical revascularisation, and presentation with an acute coronary event. All patients were followed for a maximum of 10 years starting from the day of CAA diagnosis.
Statistical analysis
Categorical variables were analysed using the Χ2 test and expressed as frequency and percentage. Continuous variables were analysed using one-way analysis of variance with post-hoc Tukey’s test, wherever appropriate, and reported as mean±SD. Univariate analysis was done using the OR; the multivariate analysis was done using the multivariable binary logistic regression. Kaplan-Meier curves were used for survival analysis. A p value cut-off of 0.05 was required for statistical significance. SPSS software (IBM SPSS Statistics for Windows, V.24.0, IBM Corp) was used for data analysis.
Results
Baseline characteristics
The current study included 458 patients, divided into three groups: 230 (50.2%) patients were managed medically, 176 (38.4%) underwent coronary artery bypass grafting (CABG) and 52 (11.3%) underwent PCI. The incidence of CAA was 0.7% of the total catheterisation reports. The mean age of the patient population was 78±10.5 years, with a male preponderance (N=341; 74.5%). Anginal symptoms were reported in 64% of individuals and 32% had a history of congestive heart failure. The details of patient baseline characteristics are mentioned in table 1.
Baseline characteristics of the enrolled patients with coronary artery aneurysm (N=458)
Coronary anatomy and aneurysms
Atherosclerotic CAD was the most common association with CAA, documented in 421 (91.7%) patients. Other reported causes of CAA included Kawasaki disease (n=2; 0.4%), congenital artery anomaly (n=2; 0.4%) and iatrogenic (due to stent implantation) (n=2; 0.4%). The mean aneurysm size was 6±0.3 mm and the mean reference vessel diameter was 2.8±0.8 mm. There was no difference in the mean aneurysm size in the medical (6 mm) versus PCI (6.9 mm) versus CABG (6 mm) groups. The details of the coronary vessels and aneurysms are mentioned in table 2.
Anatomical details of aneurysm
The mean SYNTAX score was 10±9; however, the SYNTAX scores for patients with medical management were lower at 6.5±8.2, compared with patients who had either CABG (15.4±8.4) or PCI (10.3±5.7) (p<0.001). The mean aneurysm diameter to reference vessel diameter ratio was 2.2. The most common artery involved was the left anterior descending (LAD) in 40.5% of cases, followed by the right (29.2%) and left circumflex coronary arteries (28.1%). In the PCI group, 20 (38.4%) patients received bare-metal stents and 24 (46.1%) patients received drug-eluting stents. Target vessel with aneurysm revascularisation was seen in 42 (80.7%) patients versus non-target vessel revascularisation in 10 (19.7%) patients.
Long-term outcomes
The median follow-up period was 62 (11–120) months. The total number of MACCE during follow-up was 155 (33.8 %): 91 (39.6%) in the medical management group vs 46 (26.1%) in the CABG group vs 18 (34.6%) in the PCI group (p=0.02). The MACCE rate was significantly higher in the medical management group than the CABG group (p=0.005). Other comparisons (CABG vs PCI and PCI vs medical management) were statistically insignificant.
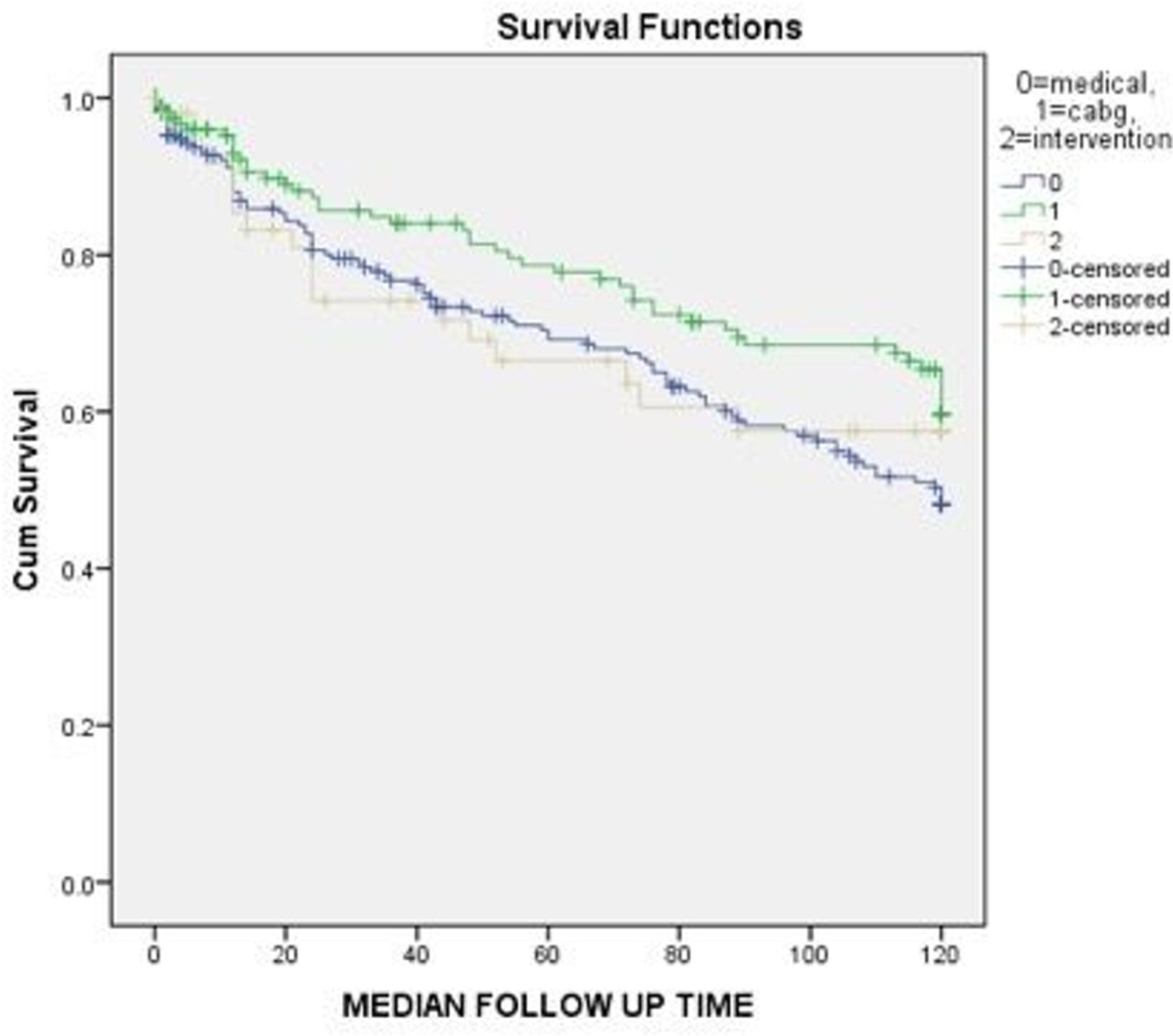
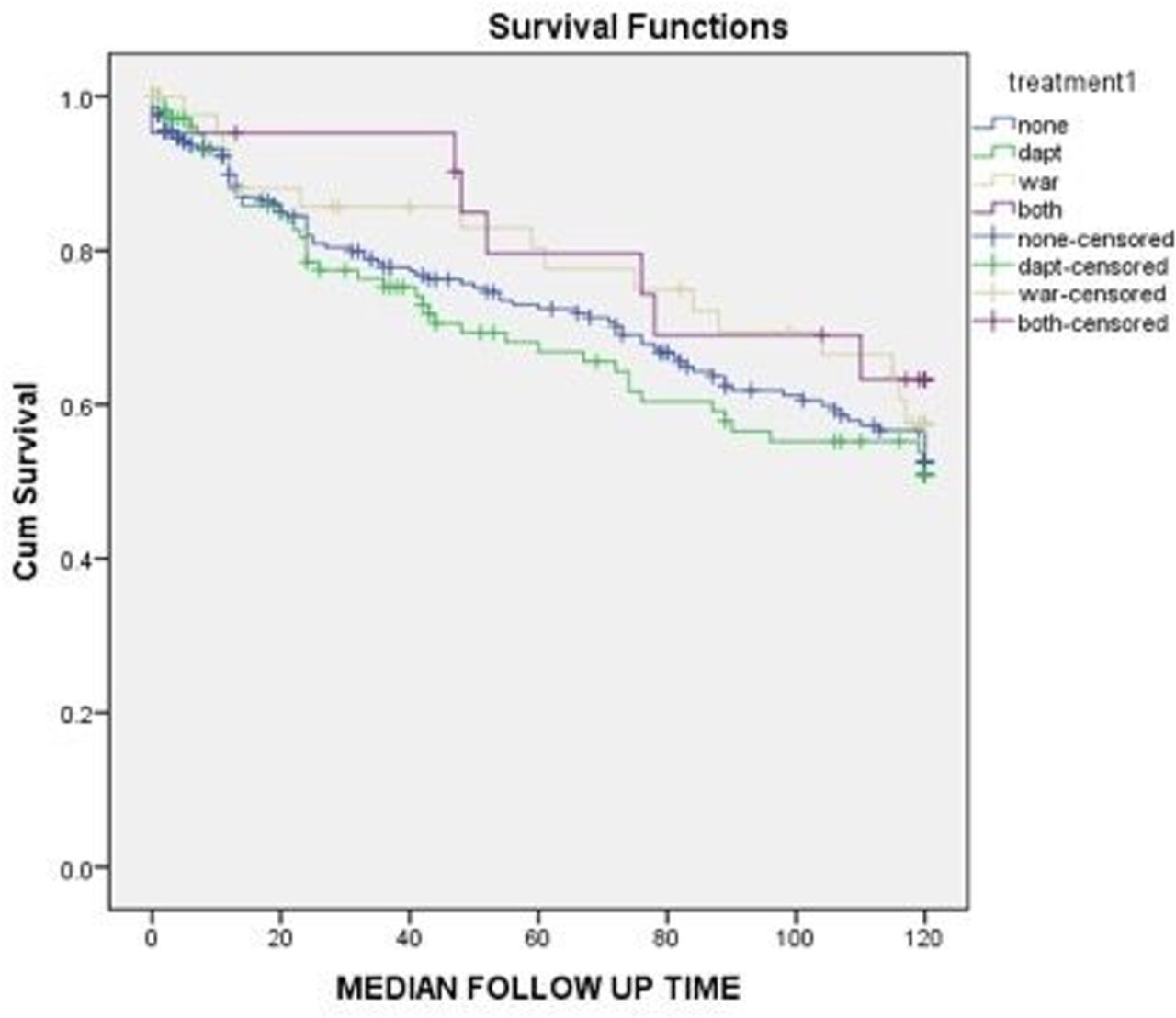
Kaplan-Meier survival analysis showed that CABG was associated with better MACCE-free survival than medical management (p log-rank=0.03); however, MACCE-free survival was similar between CABG and PCI (p log-rank=0.34), as well as between PCI and medical management (p log-rank=0.66; figure 2). In addition, there were no significant differences in MACCE-free survival between patients who received DAPT, warfarin or both (p log-rank>0.05; figure 3).

Kaplan-Meier survival analysis for freedom from major cardiovascular and cerebrovascular events (MACCEs) in different study groups (medical management vs percutaneous coronary intervention (PCI) vs coronary artery bypass grafting (CABG)). Kaplan-Meier survival curve analysis for freedom of MACCEs in patients with medical management versus CABG versus PCI in patients with coronary artery aneurysms.

{kind=link}
{kind=link}
{kind=link}
Kaplan-Meier survival analysis for freedom from MACCE in patients who received warfarin, DAPT or both. DAPT, dual antiplatelet therapy; MACCE, major cardiovascular and cerebrovascular event.
Univariate regression analysis showed that older age (OR 1.051 (1.014 to 1.056), p=0.01), acute coronary syndrome (ACS) on initial presentation (OR 1.601 (1.051 to 2.441), p=0.03), chronic heart failure (OR 2.021 (1.471 to 2.775), p<0.001) and chronic kidney disease (OR 1.685 (1.156 to 2.456), p=0.007), and aneurysm location in the left main artery (OR 1.584 (1.283 to 1.868), p<0.001) were significantly associated with increased MACCE rates in patients with CAA. In contrast, CABG treatment was associated with less MACCE on long-term follow-up (OR 0.684 (0.480 to 0.975), p=0.03). However, the association was not significant for PCI, DAPT and anticoagulation (table 3). Multivariate regression showed that only chronic heart failure was significantly associated with worse MACCE outcome (OR 1.934 (1.343 to 2.785), p<0.001). The significant MACCE difference between CABG and medical treatment was not stable on multivariate regression (OR 0.773 (0.526 to 1.136); p=0.19).
Univariate regression analysis of the factors associated with MACCE outcomes in patients with coronary artery aneurysm
Other than MACCE, aneurysm-related complications were seen in seven patients; five patients presented with thrombus formation in the aneurysmal area, one patient with type B aortic dissection after stent placement in the aneurysm and one patient with LAD to pulmonary artery aneurysm (likely secondary to congenital artery fistula).
Discussion
We report the long-term outcomes of patients with CAA from a high-volume health system. The key findings of our study were (a) the incidence of CAA diagnosis was 0.7% of all-comers for invasive coronary arteriograms; (b) atherosclerosis remained the most common cause of CAA and LAD was the most commonly involved coronary artery; (c) CABG was associated with better MACCE-free survival than medical management, but no significant difference was recorded between CABG and PCI; and (d) no significant difference in MACCE-free survival was noted between patients managed on DAPT versus warfarin.
Consistent with prior studies,6 9–11 atherosclerosis was the most common causal association of CAA, present in more than 90% of our patients. This could be due to the natural history of CAA formation with the presence of focal areas of calcification and fibrosis, as well as large cholesterol crystals. Such features weaken the vessel wall and decrease its elasticity, ultimately reducing the vessel’s tolerance to intraluminal pressure with subsequent dilatation and aneurysm formation. Long-term transmural inflammation, which is characteristic of atherosclerotic disease, further contributes to this process of vessel-wall weakening.
Because most patients with CAA in our study had associated CAD, their management was directed towards CAD revascularisation. This provided us with an opportunity to compare the long-term outcomes of patients undergoing different modes of revascularisation or medical management. Patients who underwent either CABG or PCI had higher SYNTAX scores compared with the medically managed patients, signifying the increased severity of CAD in this subset of patients. Interestingly, CABG was associated with better MACCE-free survival than medical management, but no significant difference was noted between PCI and CABG in terms of MACCE-free survival. The latter finding should be interpreted with caution because of the limited number of patients in the PCI arm of our study. Although the significant difference between CABG and medical treatment was confirmed in univariate regression, it disappeared in multivariate regression. This may be because patients selected for CABG are usually less sick than those selected for conservative therapy. Therefore, the implications of this finding are prognostic rather than to recommend CABG as a management strategy for CAA.
Former studies have reported good short-term and long-term outcomes for CABG in patients with CAA12 13 ; however, data comparing CABG outcomes to those of PCI or medical management alone are rare. Szalat et al reviewed the short-term outcomes of 18 patients with CAA who underwent CABG and 24 patients who underwent PCI. No mortality was recorded in either group. In patients with follow-up data at 4 months, 12 (92%) and 15 (79%) patients were asymptomatic in the CABG and PCI groups, respectively, while 5 patients in the PCI group developed restenosis.14 Our findings are in line with recent results from the International Coronary Artery Aneurysm Registry (CAAR). Data analysis of 1565 patients with CAA showed that CABG and PCI had similar rates of mortality (15.6% vs 15.9%, p=0.92) and MACCE (31.6% vs 31.4%; p=0.96) at short-term follow-up.15 To our knowledge, the current study offers the longest follow-up data of patients with CAA in the literature.
The role of DAPT and warfarin in patients with CAA is a topic of debate. Recent studies16–18 have shown that patients with CAA are at higher risk of MACCE compared with patients with control CAD. In our study, about 12% of patients presented with ACS (during the initial coronary arteriography), which is a high-risk group for future thrombotic events (as confirmed by univariate regression), especially in the infarct-related artery. Previous authors suggested that patients with stent placement and CAA should be considered for long-term DAPT therapy.19 20 Similarly, chronic anticoagulation to prevent downstream thromboembolism has been suggested by some studies, given the decreased coronary flow velocities in the aneurysmal artery. Anticoagulation seems to be of benefit in patients with Kawasaki disease and giant aneurysms to prevent myocardial infarction and sudden death.10 21 In atherosclerotic aneurysms, however, the benefit of anticoagulation has not been evaluated. Some authors have suggested that given the natural history of atherosclerotic aneurysms, there is no convincing evidence to justify the risk of anticoagulation.22 However, recent studies have suggested an efficacious role of anticoagulation, especially in patients with aneurysm presenting with ST-elevation myocardial infarction and coronary aneurysms with multivessel disease.23 24
In the CAAR registry, 90.2%, 64.8% and 13.4% of patients were prescribed aspirin, DAPT and anticoagulation at discharge, which we believe reflects contemporary practice.15 In our study, both Kaplan-Meier survival and Cox regression analyses showed no significant MACCE benefits for DAPT and warfarin alone or combined on long-term follow-up. Large-scale randomised trials are needed to validate our results in this high-risk population.
Limitations
Our study has the inherent limitations of a retrospective cohort study with regard to selection bias and immortal time bias. During the reading of coronary catheterisation reports, there might have been some interobserver variability in the measurement of the aneurysm size. Aiming at long-term follow-up, we retrieved the data for patients who were managed ≥15 years ago; therefore, the management strategies in this study may not reflect contemporary practice. Further, we may not have captured all deaths. In addition, our study population consisted mainly of patients with CAD; therefore, the results regarding DAPT and oral anticoagulation may not be applicable to other causes of CAA such as Kawasaki disease and connective tissue disorders.
Conclusion
CAA is often associated with CAD. Medical management, PCI and CABG are performed depending on the associated coronary anatomy with the aneurysmal lesion. In the present study, data analysis showed similar long-term MACCE risks in patients with CAA undergoing medical, percutaneous and surgical management. These findings should be interpreted with caution considering the relatively small size and the potential for selection bias in this retrospective study. In addition, we found that neither DAPT nor warfarin offers significant MACCE benefits on long-term follow-up. Large, comparative trials are needed to confirm our findings and optimise the management of these high-risk patients.
References
Footnotes
Contributors Data collection, analysis and writing of the manuscript: SK, RC, CM and AK. Review of the angiogram images: RT. Editing and writing of the manuscript: RP, FGB, CS, SE, DJ, GP and SK. Statistical analysis: MZK, MSK and SK. Data collection: KD, MG, MK, KB, BRV, YS, JR and KA. SK is responsible for the overall content of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study protocol was approved by the institutional review board at the Cleveland Clinic.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. All patient data were de-identified.