Article Text

Abstract
Objectives Non-ischaemic dilated cardiomyopathy (DCM) is characterised by a highly variable disease progression. Stress echocardiography and cardiopulmonary exercise testing (CPET) are beneficial in risk assessment, but are labour intensive. Repetitive squatting and standing without weights is a simple exercise (EX). The aim of this study was to investigate the prognostic role of left ventricular (LV) contractile recruitment (CR) after a simple EX of repetitive squatting through three-dimensional (3D) echocardiography.
Methods Patients with DCM (LV ejection fraction (EF)<50%, n=68) and age-matched healthy volunteers (n=25) received a 3D echocardiographic evaluation of LV EF before and after 30 repetitions of squatting-standing EX. CR was defined by the change of LV EF (Δ>4%). Patients were followed up prospectively (2 years) for cardiac death and deteriorating heart failure.
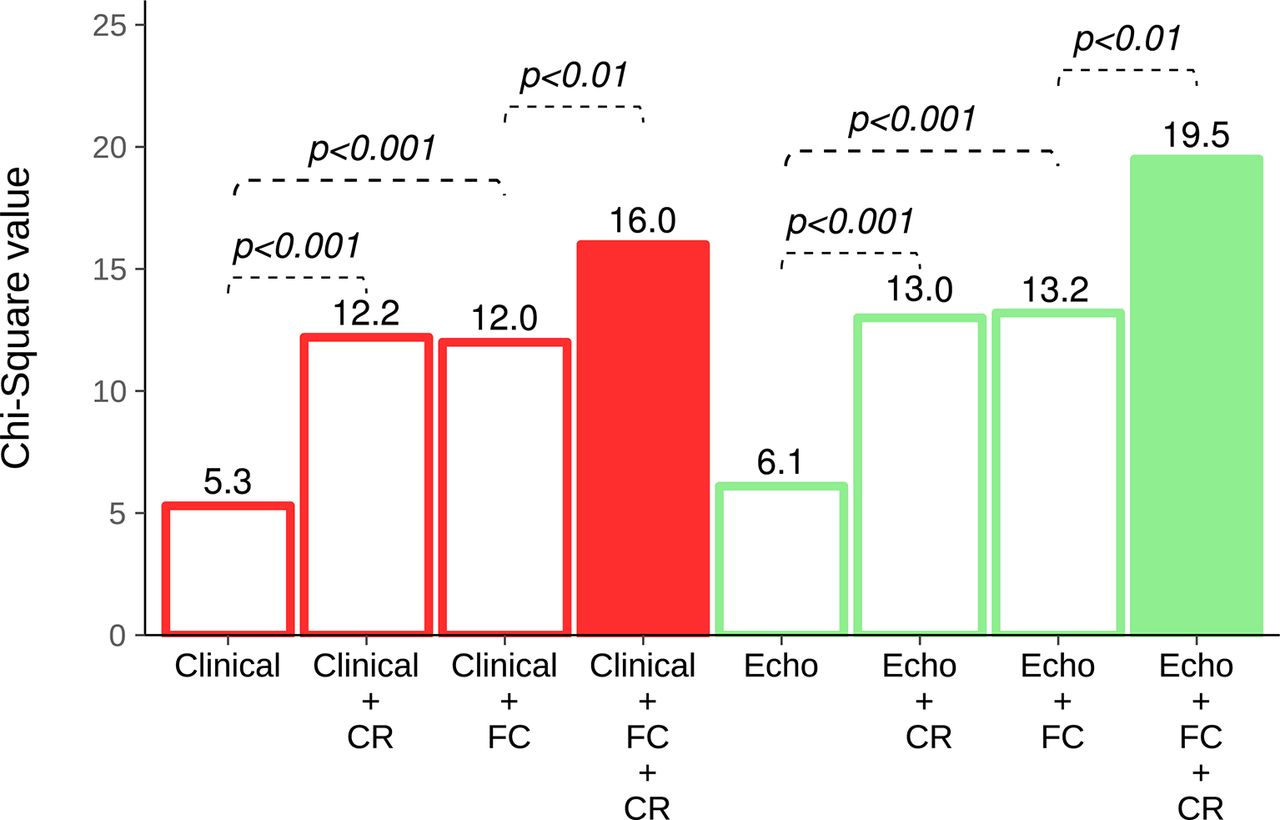
Results During follow-up, 14 cardiac events occurred (21%) with six deaths and eight severe heart failure deteriorations. A poor CR after squatting EX differentiated DCM patients with cardiac events during follow-up as accurately as a reduced peak oxygen consumption (peak VO 2<20 mL/kg/min) (sensitivity: 0.97 and 0.95). Both had a significant incremental diagnostic value over clinical (age, dyspnoea and natriuretic peptide level) or resting echocardiographic parameters (E/E’ ratio, LV EF and end-diastolic LV volume) to predict cardiac events (global χ2: 16.0 vs 5.3; 19.5 vs 6.1; P<0.01 for all).
Conclusions The presence of LV CR after EX of repetitive squatting without weights can stratify risk and predict cardiac events in patients with DCM as correct as CPET.
- cardiomyopathy dilated
- three dimensional
- stress
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Measurement of left ventricular contractile reserve by stress echocardiography and functional capacity by cardiopulmonary exercise testing are superior determinants of disease progression in patients with non-ischaemic dilated cardiomyopathy than left ventricular ejection fraction at rest. However, both methods are labour intensive and not accessible in daily practice.
What does this study add?
Determination of left ventricular contractile reserve by simple exercise of repetitive squatting without weights predicts cardiac events about as functional capacity assessed by cardiopulmonary exercise testing in patients with non-ischaemic dilated cardiomyopathy.
How might this impact on clinical practice?
These findings have the potential to enrich the daily armamentarium of cardiologists revealing the crucial difference between heart failure patients with apparently similar stable clinical conditions at high risk and those at low midterm risk.
Introduction
Non-ischaemic dilated cardiomyopathy (DCM) is characterised by a progressive left ventricular (LV) chamber dilatation and global myocardial dysfunction. Its clinical course varies considerably among patients with mild symptoms and with similarly reduced cardiac function at rest. Stress echocardiography and cardiopulmonary exercise testing (CPET) have evolved as valuable tools for differentiating unfavourable prognoses in patients with systolic heart failure.1–4 Stress echocardiography assess directly LV contractile reserve (CR) measuring myocardial viability, which is achieved by an infusion of dobutamine or by physical exercise (EX).5 Peak oxygen consumption (peak VO2) during CPET relates to peak cardiac output and reflects patient’s functional capacity.6 Stress echocardiography and CPET are safe methods, but they are labour intensive, which is why patient therapy is most commonly based on two-dimensional (2D) echocardiographic measurements of resting LV ejection fraction (EF) in an ambulatory setting. In contrast, LV chamber dimensions and EFs obtained by three-dimensional (3D) echocardiography show good agreement with measurements from cardiac MRI and are superior to the results of the 2D technique.7–9 Furthermore, 3D echocardiographic imaging does not rely on geometric assumptions and enables efficient image acquisition in one data set without repositioning of the ultrasound probe. These advantages of 3D echocardiography are desirable when cardiac function is expected to recuperate within minutes post EX.9
Repetitive squatting and standing without weights is a feasible EX that engages multiple muscle groups. As a dynamic EX, it would exhibit positive inotropic and chronotropic effects.10 Thus, the aim of this study was to investigate the prognostic role of LV CR after repetitive squatting EX by means of 3D echocardiography in patents with DCM.
Methods
Study population
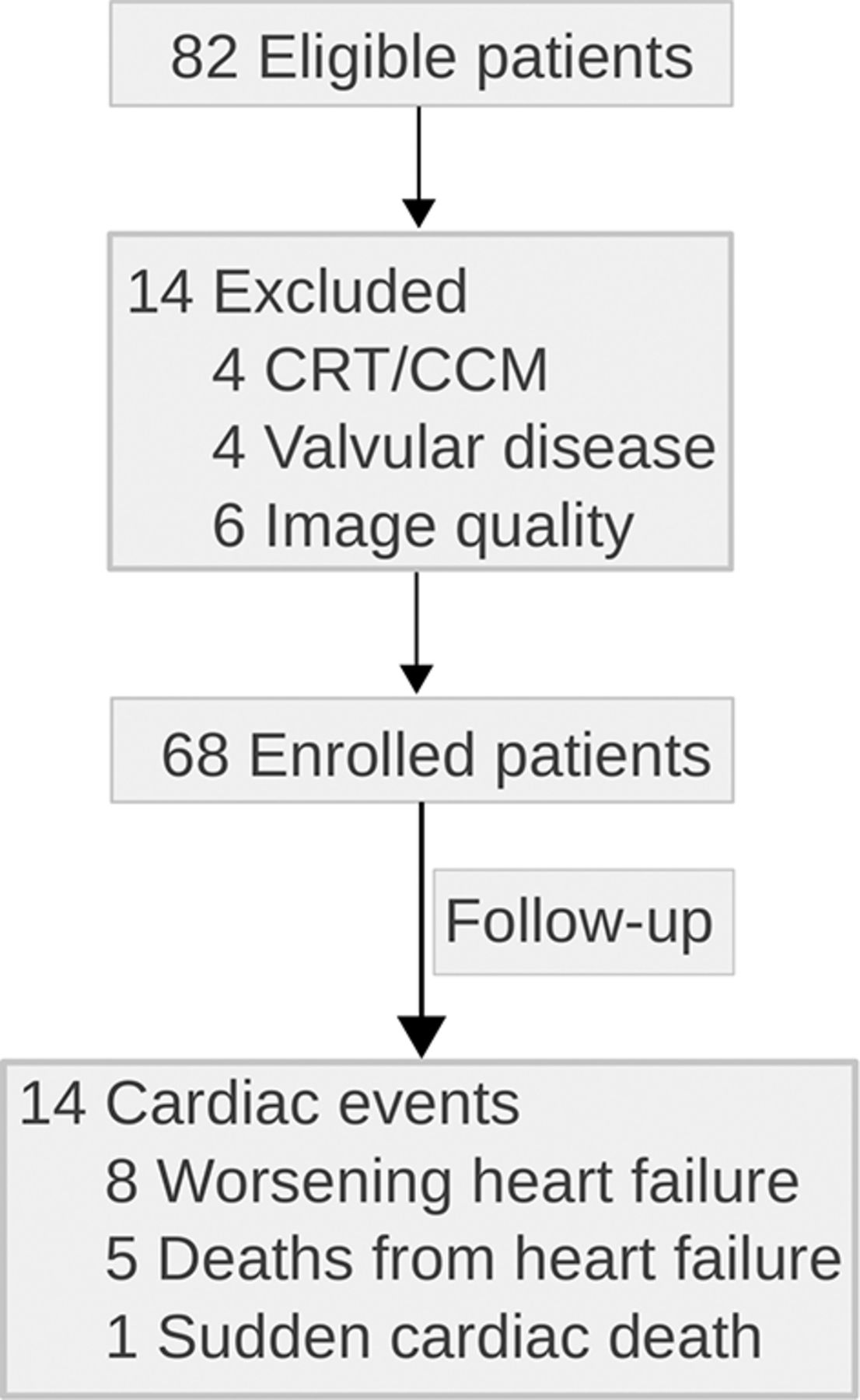
Eighty two clinically stable outpatients with a recent (<6 months) diagnosis of non-ischaemic DCM with good acoustic window but without orthopaedic disorders were screened for this prospective study. Inclusion criteria were as follows: (1) LV EF <50% in the absence of a coronary disease, (2) no clinical or magnetic-tomographic signs of myocarditis, (3) sinus rhythm without typical left bundle branch block and (4) full medical treatment according to the European heart failure guidelines.11 Right from the beginning, patients with cardiac resynchronisation/modulation therapy and with more than moderate-to-severe valve diseases were excluded (n=8) (figure 1). Twenty-five age and sex-matched healthy volunteers without a history of cardiovascular disease were included as controls. None of them reported regular training habits or had any clinical or anamnestic evidence of arterial hypertension or other cardiovascular diseases. All controls had an echocardiographic LV EF >50%, without significant valvular disease. This study was approved by the institutional review board, and written informed consent was obtained from all subjects.
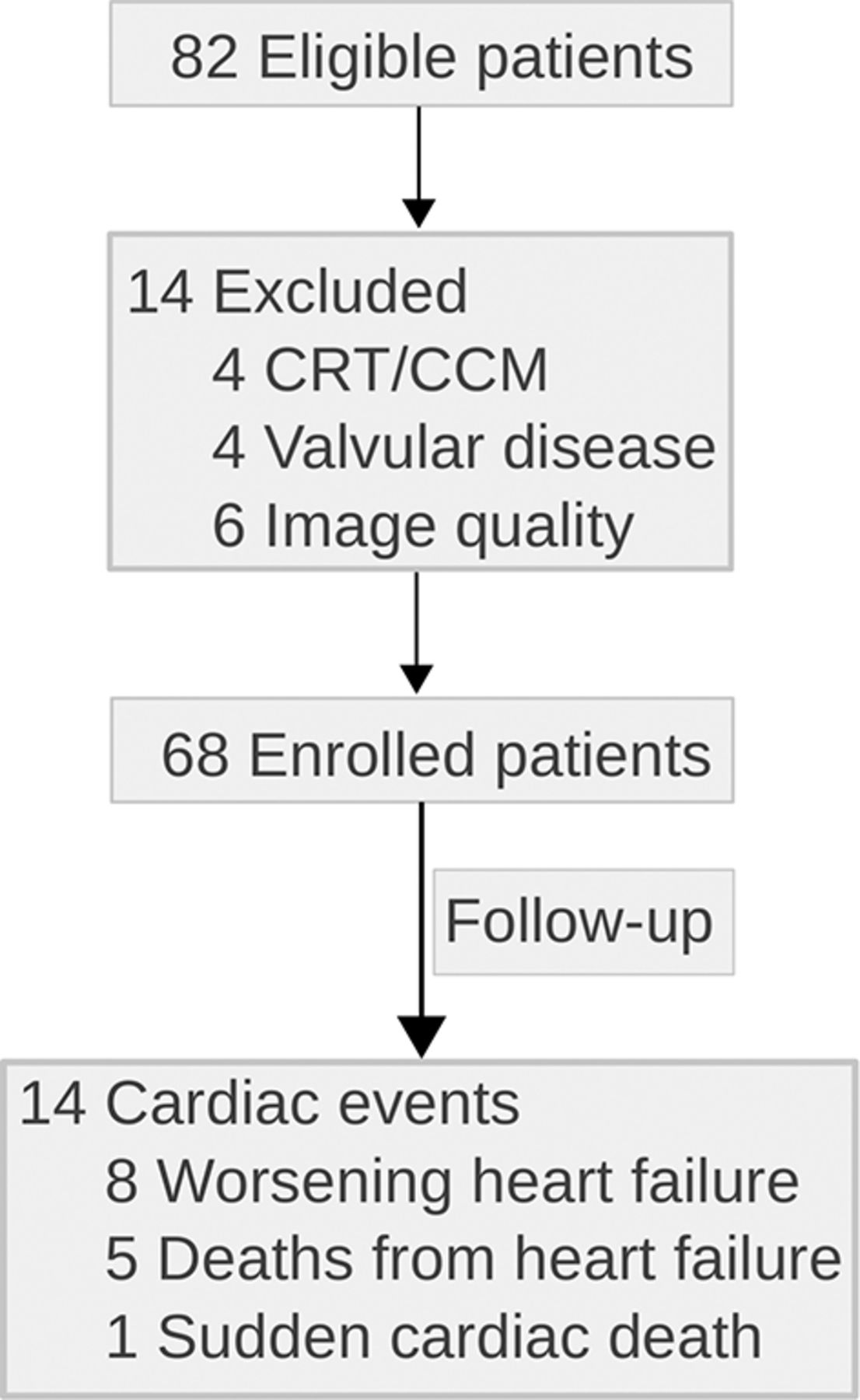
Flowchart representing the selection process of the study and the type of cardiac events occurring during follow-up period. CCM, cardiac contractility modulation; CRT, cardiac resynchronisation therapy.
Study protocol
On study enrolment, all subjects received a full 2D echocardiographic examination at rest as described previously,12 and their N-terminal pro-B-type natriuretic peptide (NT-proBNP) plasma levels were measured. The 3D echocardiographic examinations were performed at rest and within the first 2 min after 1 set of a maximum of 30 repetitions of squatting. This number of squatting repetitions is considered a fair to good performance in healthy middle-aged subjects.13 CPET followed separately within 2 days without a change of medical regime. The primary outcome was defined as composite end point of death or hospitalisation due to deteriorating heart failure, sudden cardiac death or ventricular arrhythmias requiring hospital admission. Follow-up was performed by cardiologists blinded to the results previously obtained from repetitive squatting EX. No patient was lost during follow-up (figure 1).
Image acquisition and repetitive squatting EX
Apical 3D echocardiography of the left ventricle was obtained using a PST-25SX (1–4 MHz) phased-array matrix transducer (Toshiba Artida 4D system, Japan) in left cubital position at rest and again in left cubital position immediately within 2 min after completion of repetitive squatting EX. Blood pressure was measured at rest and immediately after repetitive squatting EX. ECG-gated subvolumes of four to six heart cycles were acquired during a breath-holding manoeuvre. Elevation tilt, lateral contrast and volume rates (mean 22±3 videos per second) were adjusted to achieve optimum imaging quality. Six patients (8%) were excluded from follow-up analysis because of poor image quality after repetitive squatting EX.
Image analysis
All data sets of 3D echocardiographic LV volumes were analysed offline semi-automatically by a dedicated wall motion tracking software (WMT, Toshiba Medical System, Japan) as described previously.7 Three independent measures were performed and represented as the individual’s mean. LV end-diastolic volume (EDV) and LV end-systolic volume (ESV) derived from 3D echocardiography were indexed to body surface area and used to calculate stroke volume (SV), cardiac index (CI) and LV EF. Intra-observer reliability of EDV, ESV and LV EF was estimated from 15 randomly selected data sets at rest and after repetitive squatting EX by the same investigator at least 1 week apart.
Cardiopulmonary exercise testing
All patients underwent a symptom-limited bicycle CPET based on three distinct stages under medical supervision until exhaustion.14 Blood pressure values and a continuous 12-lead ECG were recorded. Peak VO2 was measured, and the respiratory exchange ratio indicated the patient’s effort during CPET.
Statistical analysis
Peak VO2<20 mL/kg/min was defined as a reduced functional capacity.15 Differences in echocardiographic parameters between rest and after squatting EX were expressed as Δ values. Patients were divided into two groups, based on whether they developed a CR with Δ LV EF>4% or not.16 Continuous data were presented as mean (with SD) unless otherwise specified. Normal distribution was evaluated by the Shapiro-Wilk W test. Comparisons between groups’ mean and between rest versus after repetitive squatting EX were performed using paired/unpaired Student’s t-test or Wilcoxon signed-rank test as appropriate. Pearson’s correlation coefficient (r) was assessed. Categorical data were summarised as frequencies and percentages and were subjected to Fisher’s exact test. Univariate Cox proportional hazard analysis was applied to identify predictors of the primary end point. Effect sizes of predictors were expressed as HR with 95% CI (see table 4). Predictors from univariate regression with P<0.10 or important clinical markers were used for multivariate Cox analyses as summarised in online TableS1 of supplementary material. In detail, basal regression models with standard clinical (ie, age, New York Heart Association (NYHA) and NT-proBNP) or standard echocardiographic (ie, age, E/E' ratio and resting LV EF) parameters were constructed. These models were augmented to predict cardiac events by addition of peak VO2 from CPET or/and CR from repetitive squatting EX (ie, ΔLV EF). These Cox models were separately compared by likelihood ratio tests expressed as global χ2 values with the corresponding significance value indicating higher predictive power for events during follow-up (figure 3). Final statistical significance was defined as a two-tailed P value<0.05. All statistical analyses were performed with open-source software R (V.3.0.2, 2013, The R Foundation for Statistical Computing, Vienna).
Supplementary file 1
Results
Baseline characteristics at study enrolment
Table 1 summarises the anthropomorphic and clinical characteristics of patients with DCM and healthy controls at the time of study enrolment. Clinical characteristics did not differ significantly between DCM patients with CR and without CR, except for a trend of higher NYHA functional class and ESV in patients without CR. Both patient groups received equal medical treatment.
Clinical characteristics of healthy controls and patients grouped by CR at baseline
LV function after repetitive squatting EX at baseline
Comparisons of echocardiographic and haemodynamic data according to the presence or absence of CR are reported in table 2. Interestingly, there were no significant echocardiographic differences between patients with CR and without CR at rest. However, patients without a CR showed not only an inadequate increase of LV EF, SV and CI but a rise of ESV and EDV after squatting EX. In contrast, patients with a CR exhibited an overall increase of LV functional parameters with a proportional decrease of ESV, while EDV remained stable after squatting EX. These characteristics were similar to healthy controls. Of note, ∆LV EF ranged from 4% to 12% in healthy controls. ΔLV EF showed strong correlation with ΔLV ESV, ΔSV and ΔCI after repetitive squatting EX (r=−0.75, 0.79 and 0.67, P<0.001 for all), modest correlation with ΔLV EDV (r=−0.30; P=0.01) and no significant association was found with E/E' ratio, age or medication (P>0.05 for all).
Echocardiographic characteristics before and after squatting EX
CPET at baseline
At study enrolment, peak VO2 was significantly lower in patients without CR than in those with CR, although workload, EX effort and haemodynamics at peak CPET were not different as summarised in table 3. Peak VO2 correlated strongest with ESV and LV EF after squatting EX followed by E/E ratio at rest (r=−0.61, 0.56 and −0.47, P<0.001 for all). Patients without an LV CR (n=39, 57%) were more likely to exhibit a reduced functional capacity (n=24, 64%) than patients with an LV CR (n=5, 7%) (OR=7.73, P<0.001).
Cardiopulmonary test results of patients without and with a CR
Prognostic factors of clinical outcome
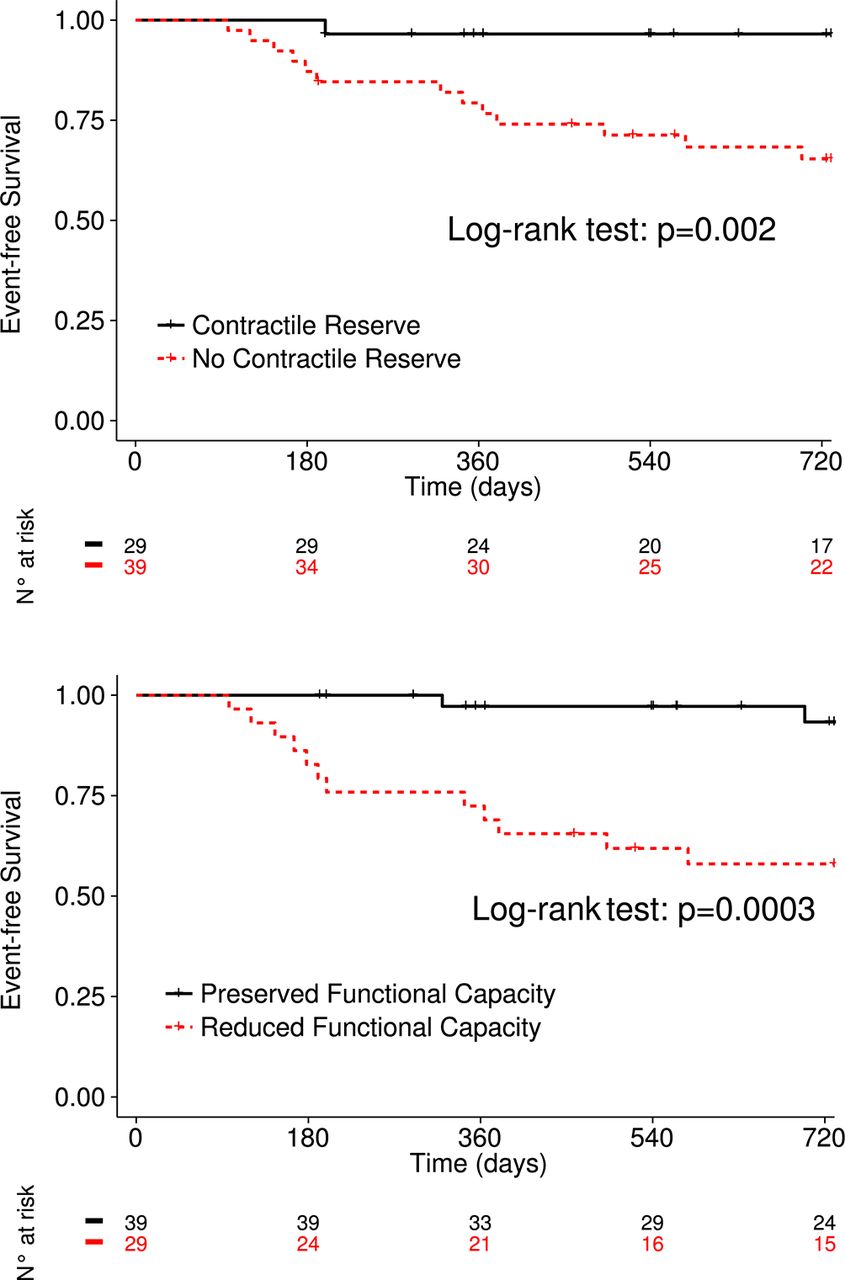
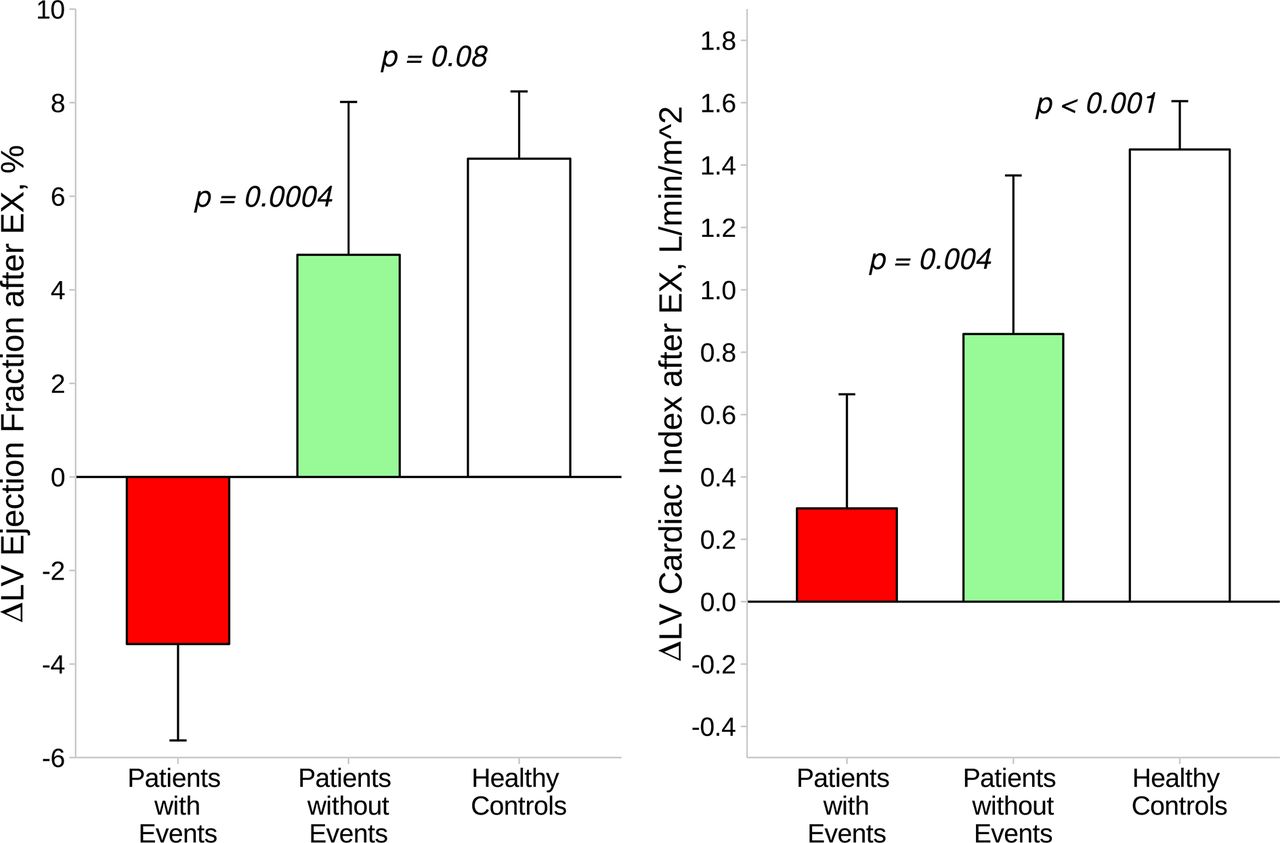
Median follow-up time of patients was 725 days. Fourteen patients (21%) developed adverse cardiac events as follows: five patients died of heart failure, one of sudden cardiac death and the remaining eight patients were hospitalised due to worsening heart failure (see figure 1). Unadjusted Kaplan-Meier curves depict event-free survival in patients with DCM stratified by functional capacity and by LV CR after repetitive squatting EX in figure 2. The presence of LV CR had similar sensitivity and specificity (0.97 and 0.51) as a preserved functional capacity (0.95 and 0.68) to detect a more favourable outcome in patients with DCM. Table 4 summarises the results of univariate Cox proportional hazard analysis of factors related to the development of cardiac events. Multivariate analysis showed that neither resting echocardiographic parameters (age, LV EF and E/E') nor clinical data (NT-pro BNP and NYHA) alone were independently associated with cardiovascular events (χ2=5.35, P=0.14 and χ2=6.07, P=0.11). Adding information about LV CR to peakVO2 and to main echocardiographic and clinical parameters yielded an incremental improvement in outcome prediction as depicted in figure 3. A summary of the multivariate analysis is found in online Table S1 of supplementary material. As expected, stratifying patients with DCM by the occurrence of cardiac events showed that these patients exhibited a deteriorating LV EF after repetitive squatting EX at baseline compared with those patients without cardiac events as depicted in figure 4. Furthermore, baseline peak VO2 was significantly lower in patients with than without events during follow-up (16±3 vs 23±6 mL/Kg/min, P<0.001).
Cox proportional hazards analysis for cardiac events during follow-up
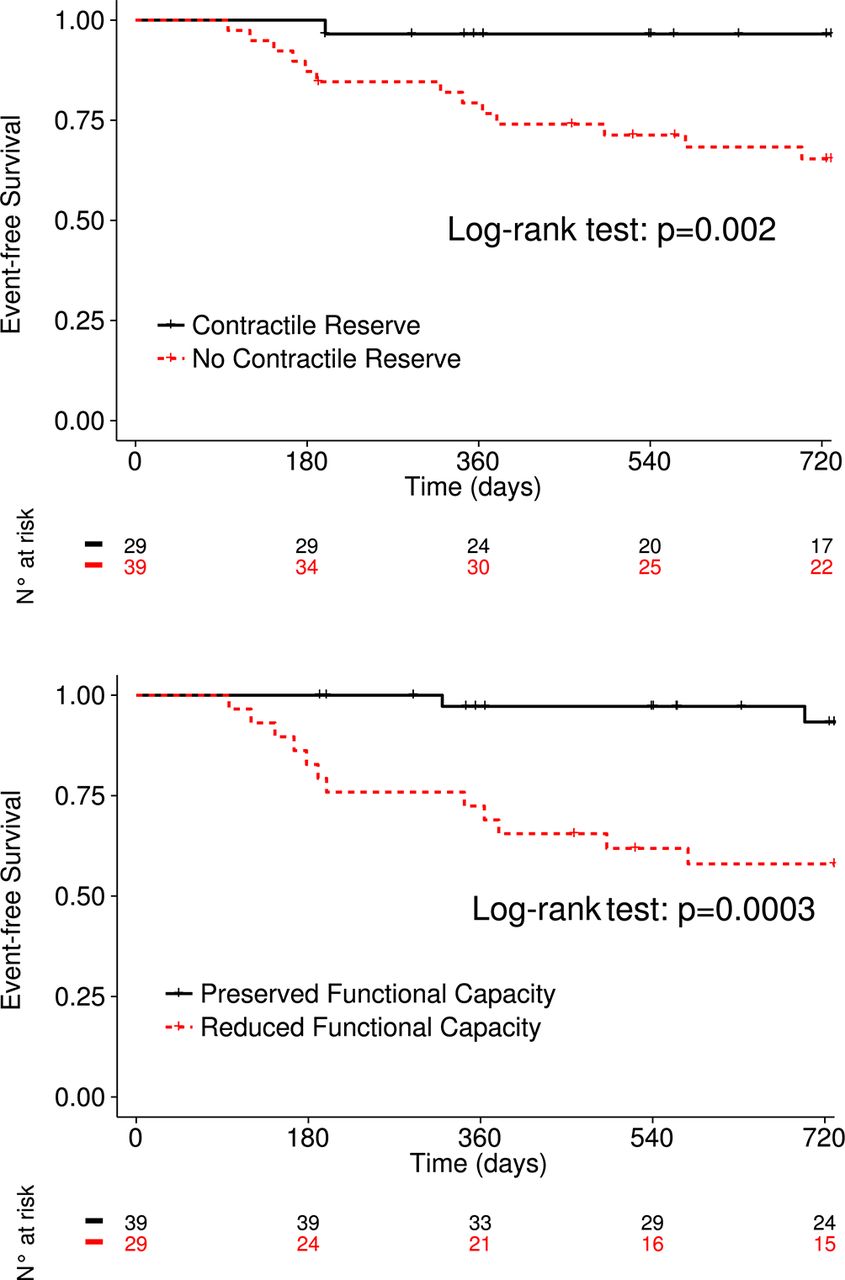
Event-free survival in patients with dilated cardiomyopathy stratified by the existence of contractile reserve (Δ left ventricula ejection fraction >4%) after repetitive squatting exercise (upper) or by the existence of preserved functional capacity (peak oxygen consumption>20 mL/Kg/min) from cardiopulmonary exercise testing (lower).

Incremental predictive value of CR after repetitive squatting exercise and FC from cardiopulmonary testing exercise results over clinical (red) and echocardiographic (green) information by likelihood ratio analysis expressed as χ 2 values (y-axis) for prediction of adverse clinical events. Basal clinical model (first red column) consisted of age, NT-proBNP levels and NYHA functional class, while basal echocardiographic model (first green column) consisted of age, E/E' ratio and LV EF obtained at rest. CR, contractile reserve; E/E', ratio of pulsed-wave Doppler-derived early diastolic transmitral flow and tissue Doppler-derived early diastolic velocity obtained from the lateral mitral annulus; EF, ejection fraction; FC, functional capacity; LV, left ventricular; NT-proBNP, N-terminal pro-B-type natriuretic peptide; NYHA, New York Heart Association.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Changes (Δ) of left ventricular (LV) ejections fraction (left) and Δ cardiac index (right) after repetitive squatting exercise in patients with (red) and without (green) events compared with healthy controls (white). Data expressed as median with IQR. P values indicate significance levels for differences between groups assessed by appropriate test. EX, exercise.
Intra-observer reliability
Intraclass correlation coefficient (ICC) in the measurement of resting LV EDV and ESV was 0.98 and 0.97, respectively, corresponding to LV EF of 0.97 (P<0.001 for all). Again after repetitive squatting EX, ICC values were as follows: 0.98, 0.98 and 0.97 (P<0.001 for all).
Discussion
This study evaluated the prognostic role of LV CR after repetitive squatting EX by means of 3D echocardiography in patients with DCM. The major findings of this study are as follows: (1) repetitive squatting EX has the ability to disclose LV CR in patients with DCM and in healthy persons (figure 4); (2) absence of LV CR after repetitive squatting EX predicts future cardiac events (figure 2) similarly as a reduced functional capacity by CPET (figure 3); (3) it is superior than resting LV EF or clinical baseline characteristics and (4) LV CR assessed by repetitive squatting-standing EX is an additional diagnostic tool to CPET in order to discriminate patients at higher risk (figure 3).
Both, determination of functional capacity by CPET and assessment of LV CR by stress echocardiography are indispensable tools for differentiating adverse prognoses in patients with heart failure.3–4 17–19 CPET is regarded the clinical gold standard in the evaluation of patient’s EX ability with peak VO2 as one of the main markers of functional performance.15 Traditionally stress echocardiography is performed with bicycle EX or with inotropic drugs in order to determine LV CR,5 but it is labour intensive or not everywhere accessible in daily practice. Both peak VO2 and LV CR rely on increasing cardiac output due to an augmented LV SV6 which is dependent on the decrease of LV ESV.20 Indeed, we could demonstrate that improving peak VO2 was strongly related to a concomitant decrease of LV ESV and increase of LV EF after squatting EX. Furthermore, LV CI adapted after EX with augmentation of LV SV and heart rate in order to fulfil blood/oxygen demand which is in line with the definition of CR.21 Patients with a decrease of LV SV and EF exhibited for instance a reduced functional capacity disclosing an insufficient rise of CR (figure 4). Repetitive squatting performed as a dynamic EX engages multiple muscle groups and provides positive inotropic and chronotropic effects on the healthy heart.10 22 In this study, we clearly demonstrated that repetitive squatting EX has the ability to disclose an LV CR in patients with DCM and in healthy persons.
The determination of LV EF at rest remains routine practice to guide patient’s therapy, although over the last decade the scientific community has given up on the idea that it could be the exclusive marker of functional capacity14 23 or of clinical prognosis.24 25 Therefore, it should be important to evaluate LV functional response under dynamic conditions by use of EX or pharmacological stress that otherwise would be missed at rest. An all-accessible method of stress echocardiography in order to determine LV CR could enrich the daily armamentarium of cardiologists identifying patients with heart failure at higher risk for cardiac events. Indeed, as to our knowledge for the first time, our study demonstrates that the presence of LV CR after simple squatting EX is similarly predictive of a favourable clinical outcome in patients with DCM as the presence of a preserved functional capacity determined by CPET (figure 2). Both patients with and without a LV CR showed similar clinical and echocardiographic baseline characteristics at rest (tables 1 and 2). However, patients without LV CR developed a concomitant dilation of LV EDV and impairment of peak VO2 after EX which is indicative of a more progressive disease stage in these subjects.2 23 26 Increase of preload after EX would induce myocardial prestretch with augmentation of myocardial contraction, for instance improving LV emptying in healthy hearts. However, in the context of per se reduced cardiac contractility27 with loss of contractile units augmented preload may induce elevated systolic wall stress and decrease lusitropy which in turn causes a drop in cardiac output due to a afterload/preload mismatch via a dysfunctional Frank-Starling mechanism in systolic heart failure.28 Indeed, our results underpin that LV CR after squatting EX is a superior predictor of outcome than resting echocardiographic parameters or other clinical characteristics (figure 3). These findings are in agreement with previous stress echocardiography studies1 2 19 20 in which the absence of CR was a strong determinant of adverse outcome in patients with systolic heart failure. Our study clearly shows that a repetitive squatting-standing performed as a stress EX is an additional diagnostic tool to CPET in order to discriminate patients at higher risk.
Limitations
There are certain limitations to this prospective observational pilot study. First, this single-centre study was performed within a mid-term follow-up time and the diagnosis of heart failure was made <6 months. Second, the number of events in our study group was limited. Our patients with DCM exhibited concomitant elevated LV filling pressures at rest (ie, E/E' and NT-proBNP), but are considered as compensated and of lower risk for cardiac events.29 30 This circumstance did not allow us to adjust the variables in a full multivariable model. Further studies with a broader collective of patients with systolic heart failure are needed to validate the present findings. Third, 3D echocardiography is limited by its relative low temporal resolution. However, we demonstrated good reproducibility of LV dimensions and EF at rest as well as after repetitive squatting EX. Furthermore, we are confident that the ongoing development in echocardiographic imaging will augment the usability of this method in order to facilitate further studies.
Conclusion
The results of this study demonstrate that a fast stress test by repetitive squatting EX reveals the crucial difference between heart failure patients with apparently similar stable clinical conditions at high risk and those at low midterm risk. LV CR assessed with 3D echocardiography and with repetitive squatting predicts cardiac events about as functional capacity assessed by CPET enriching the daily armamentarium of cardiologists.
References
Footnotes
KMS and SU contributed equally.
Contributors All authors have contributed to this investigation as follows: study concept and proposal (KMS and SU: both authors contributed equally), data acquisition (KMS, SU, MR, CP, SQ, SK, KI), data analysis (KMS, SU, MR), drafting of manuscript (KMS, SU,RHS, SJ) and critical revisions of the manuscript (all authors).
Funding This research received no grant from any funding agency in the public or commercial sectors.
Competing interests None declared.
Ethics approval Institutional Review Board of Techinical University Dresden, Medical Faculty.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.