Article Text

Abstract
Background There is a paucity of real-world data assessing the association of operator volumes and mortality specific to primary percutaneous coronary intervention (PPCI).
Methods Demographic, clinical and outcome data for all patients undergoing PPCI in Leeds General Infirmary, UK, between 1 January 2009 and 31 December 2011, and 1 January 2013 and 31 December 2013, were obtained prospectively. Operator volumes were analysed according to annual operator PPCI volume (low volume: 1–54 PPCI per year; intermediate volume: 55–109 PPCI per year; high volume: ≥110 PPCI per year). Cox proportional hazards regression analyses were undertaken to investigate 30-day and 12-month all-cause mortality, adjusting for confounding factors.
Results During this period, 4056 patients underwent PPCI, 3703 (91.3%) of whom were followed up for a minimum of 12 months. PPCI by low-volume operators was associated with significantly higher adjusted 30-day mortality (HR 1.48 (95% CI 1.05 to 2.08); p=0.02) compared with PPCI performed by high-volume operators, with no significant difference in adjusted 12-month mortality (HR 1.26 (95% CI 0.96 to 1.65); p=0.09). Comparisons between low-volume and intermediate-volume operators, and between intermediate and high-volume operators, showed no significant differences in 30-day and 12-month mortality.
Conclusions Low operator volume is independently associated with higher probability of 30-day mortality compared with high operator volume, suggesting a volume–outcome relationship in PPCI at a threshold higher than current recommendations.
- Percutaneous Coronary Intervention
- PRIMARY PCI
- Myocardial Infarction
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Operator volumes in percutaneous coronary intervention (PCI) are inversely associated with in-hospital adverse outcomes. However, there are insufficient data examining the thresholds of volume, in addition to 30-day and 12-month outcomes in patients undergoing primary PCI (PPCI) for ST-segment elevation myocardial infarction (STEMI).
WHAT THIS STUDY ADDS
This study has demonstrated that there is an inverse association between operator-volume and 30-day mortality in patients undergoing PPCI for STEMI, at a threshold higher than the current American Heart Association (AHA) threshold of ≥11 PPCI/year. This study has also assessed for the first time, 12-month mortality in this cohort of patients.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
The current AHA recommendation of ≥11 PPCI/year may need to be re-examined, as differences in outcomes have been demonstrated at a higher threshold.
Introduction
Primary percutaneous coronary intervention (PPCI) is the guideline-recommended treatment for ST-segment elevation myocardial infarction (STEMI) due to superior efficacy compared with fibrinolysis.1–3
Numerous studies have examined the association between individual and institutional PCI volume and clinical outcome, with most but not all concluding that PCI performed by high-volume operators in high-volume centres is associated with the best outcomes.4–15 The 2011 American Heart Association (AHA) guidelines recommended that PPCI should be performed in hospitals undertaking more than 400 elective PCI procedures per year and 36 PPCI procedures per year, by operators performing more than 75 elective PCI procedures per year and at least 11 PPCI procedures per year.16 While studies analysing the association between individual PCI operator volume and clinical outcomes exist, the data specific for annual individual operator PPCI volume are limited to only in-hospital and 30-day outcomes.17–19 We hypothesised that there would be an inverse association between individual operator PPCI volume and clinical outcomes, irrespective of operator status (internal operator or visiting operator), and sought to investigate this in a large consecutive patient series from a high-volume UK surgical centre.20
Methods
The West Yorkshire PPCI Outcome Study was a prospective observational study designed to identify procedural and demographic variables associated with clinical outcomes, in patients undergoing PPCI for STEMI in Leeds General Infirmary, UK.20–22 Leeds General Infirmary is the largest single-site PPCI centre in the UK by volume, providing a regional 24/7 PPCI service to a catchment population of approximately 3.2 million people, achieving 100% population coverage.23 All patients who presented to Leeds General Infirmary for PPCI during a 4-year calendar period between 1 January 2009 and 31 December 2011, and between 1 January 2013 and 31 December 2013 were enrolled into this study. Patients who presented between 1 January 2012 and 31 December -2012 were not included in this study due to limited research staff availability at the time, which did not allow for data input and follow-up for that period.
STEMI was diagnosed according to standard criteria—chest pain consistent with myocardial ischaemia for a minimum of 20 min, with ST-segment elevation of ≥2 mm in contiguous chest leads and/or ≥1 mm in contiguous limb leads, or presumed new left-bundle branch block morphology on a 12-lead ECG. Patients who were diagnosed with STEMI at the point of first medical contact (with paramedics if out of hospital or with hospital practitioners/clinicians if in-hospital), were transferred directly to the cardiac catheterisation laboratory in Leeds General Infirmary with a telephone referral en route, for emergency coronary angiography and (if indicated), PPCI if within 12-hours of symptom onset.24 Patients were preloaded with oral aspirin (300 mg) at the point of diagnosis, prior to arrival at the cardiac catheterisation laboratory. P2Y12-receptor inhibitor loading dose was typically administered in the cardiac catheterisation laboratory on arrival, prior to angiography.
Procedural anticoagulation was achieved with either bivalirudin or unfractionated heparin (± bail out glycoprotein IIb/IIIa antagonist). Choice of stent (drug-eluting stents or bare-metal stents), arterial access site and aspiration thrombectomy were performed according to individual operator discretion, informed by guideline recommendations and experience. Preprocedure and postprocedure antegrade blood flow in the infarct-related coronary artery (IRA) was graded according to the thrombolysis in MI (TIMI) grading score of 0–3. Call for help time (call time) and time of patient arrival at Leeds General Infirmary (door time) were obtained from ambulance reports if patients were brought into the cardiac catheterisation laboratories directly by paramedics, or emergency department notes if patients self-presented to the hospital. Time of first interventional device (balloon time) was obtained from the cardiac catheterisation laboratory report.
Patients remained in hospital for a minimum of 72 hours post-PPCI, which included a minimum of 24 hours of observation on the coronary care unit. Patients were typically repatriated to the coronary care unit at their local hospital following 6–12 hours of observation post-PPCI on the coronary care unit at Leeds General Infirmary. Secondary prevention (dual antiplatelet therapy (DAPT) with aspirin and a P2Y12-receptor inhibitor, statin, beta-adrenergic receptor-blocker, ACE inhibitor or angiotensin II receptor-blocker, and (if indicated) mineralocorticoid receptor antagonists were prescribed according to guideline recommendations and clinical judgement.20
Follow-up
Written and electronic case notes were interrogated prospectively at the time of discharge to obtain demographic and procedural variables. A combination of telephone contact, access to local hospital written or electronic case notes, contact with the responsible General Practitioner, and data retrieval from the Office of National Statistics were utilised to ascertain drug therapy and mortality to a minimum of 12 months following index PPCI. Data adjudication was conducted by blinded clinicians, in consensus.
Determining annual operator PPCI volume
Operators performing PPCI in Leeds General Infirmary were either internal operators (primary employment at Leeds General Infirmary, performing both in-hours (08:00–18:00 hours, Monday–Friday) and out-of-hours (18:00–08:00 hours, Monday–Friday, all-day Saturday and Sunday) PPCI only at Leeds General Infirmary) or visiting operators (primary employment in other regional hospitals, performing mainly out-of-hours PPCI at Leeds General Infirmary).
Operator volume was derived by calculating the mean number of PPCI procedures performed by each operator over the period of time they contributed to the PPCI service, which ranged from 6 months to 4 years. Volume tertiles were then derived by calculating 33rd (55.5 PPCI per year) and 67th (110.3 PPCI per year) centiles of operator volumes, based on all PPCI procedures performed over the 4-year period. From this, relevant tertiles (low volume: 1–54 PPCI procedures per year, intermediate volume: 55–109 PPCI procedures per year and high volume: ≥110 PPCI procedures per year) were determined.
Statistical analysis
Data verification was undertaken to ensure validity of data obtained. Summary statistics were then generated. Categorical variables were compared using χ2 tests, and were reported as frequencies with their corresponding percentages (n (%)). Continuous variables were compared using one-way analyses of variance for operator volume analyses. Independent samples Student’s t-test and Mann-Whitney u-test were used to compare continuous variables according to operator status (internal operator vs visiting operator). All continuous variables were reported as medians with their corresponding IQR. Results were analysed according to individual operator PPCI volume tertiles, and according to operator status. All analyses were conducted in IBM SPSS (V.23.0.0.2).
Clinical endpoints were 30-day and 12-month all-cause mortality. Survival analyses were undertaken using Cox proportional hazards (Cox PH) models. All proportional hazards assumptions were satisfied. Potential confounding factors that were adjusted for by inclusion in the Cox PH models, in addition to operator volume tertile were: patient age, previous history of MI, hypertension, hypercholesterolaemia, diabetes mellitus, peripheral or cerebral vascular disease, cigarette-smoking (ex-smoker or current smoker), left main coronary artery culprit vessel, out-of-hours PPCI and door-to-balloon (DTB) time of ≥90 min. The high-volume operator tertile was used as the reference category for the regression analyses. The Cox PH regression analyses were then repeated to compare 30-day and 12-month mortality between PPCI performed by internal operators and PPCI performed by visiting operators, by substituting operator volumes with the binary variable ‘internal operator’. For this analysis, ‘internal operator’ was used as the reference for survival analyses, with the other previously described variables remaining in the model. All HRs quoted were obtained from the Cox PH models, and reported with 95% CIs. Kaplan-Meier curves according to operator volumes were generated from the Cox models for both endpoints. A two-sided p≤0.05 was considered statistically significant.20
Results
A total of 4056 patients underwent PPCI during the study period. Baseline and procedural data were available for 3703 patients (91.3%) who were followed up, who were included in the analysis. Data for both 30-day and 12-month mortality were available for all patients included in the analysis. There were 1122 cases performed by 23 low-volume operators, 1284 cases performed by five intermediate-volume operators, and 1297 cases performed by three high-volume operators. Baseline and procedural characteristics are compared in table 1.
Baseline and procedural characteristics according to annual operator PPCI volume
There were no statistically significant differences in baseline characteristics across the tertiles. In terms of procedural characteristics, out-of-hours PPCI, radial artery access, aspiration thrombectomy, use of third-generation P2Y12-receptor inhibitors (prasugrel and ticagrelor), stent implantation, glycoprotein IIb/IIIa antagonist use, CTB and DTB times, and postprocedural TIMI 3 flow were significantly different across the tertiles (table 1).
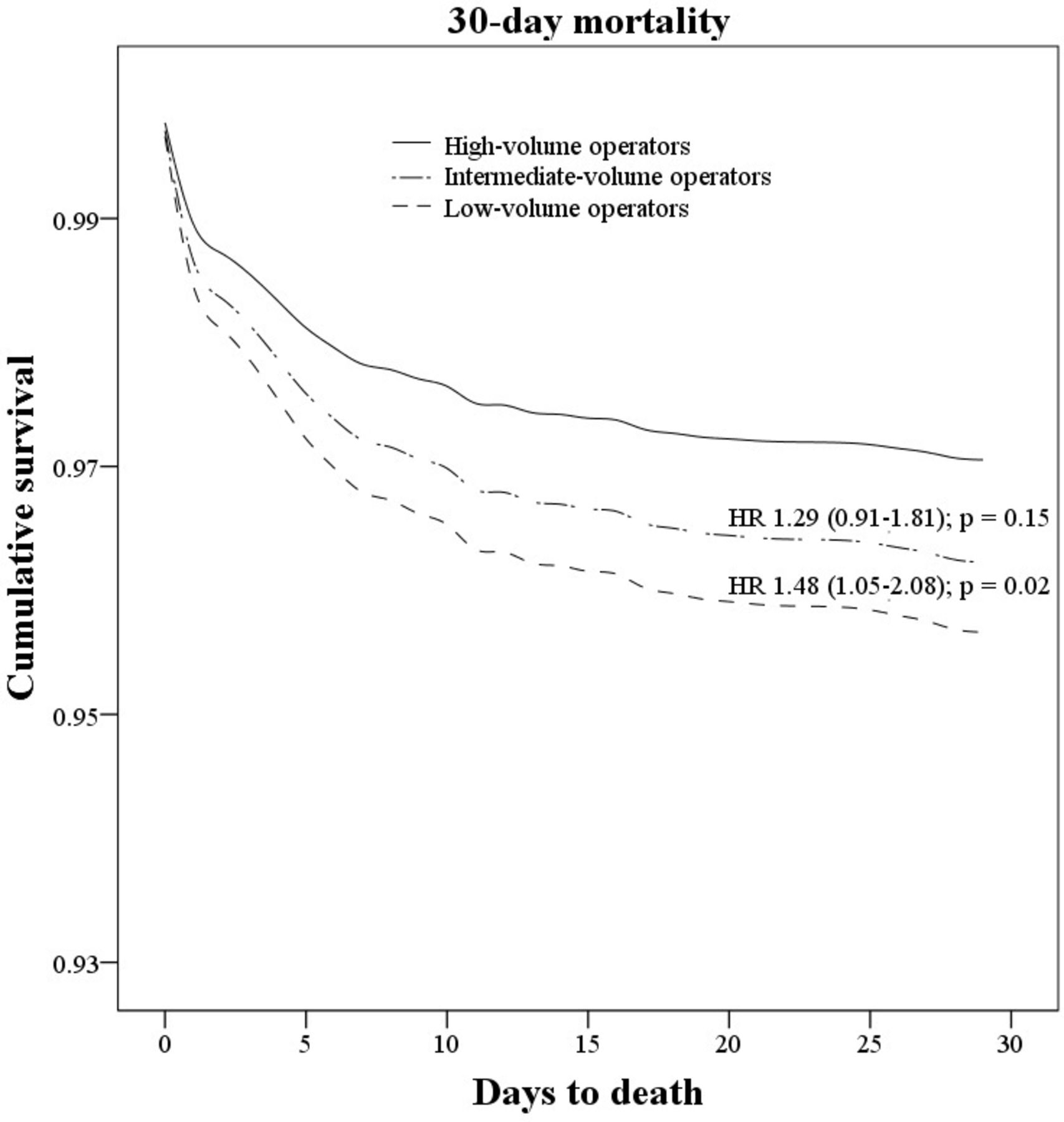
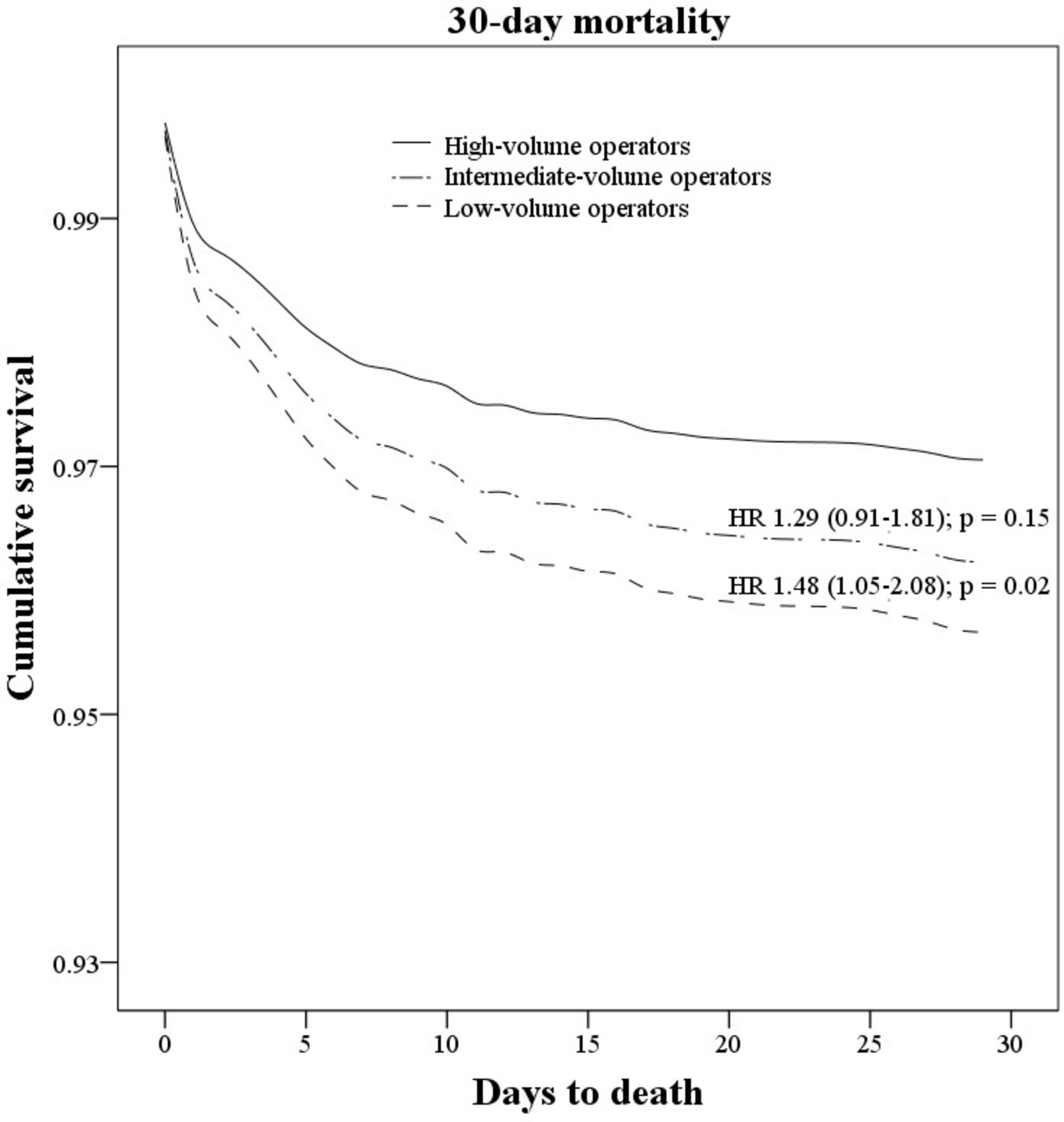
Thirty-day mortality was observed in 76 (6.8%) patients in the low-volume tertile, 71 (5.5%) patients in the intermediate-volume tertile, and 66 (5.1%) patients in the high-volume tertile (χ2 p=0.19). Twelve-month mortality was observed in 112 (10.0%) patients in the low-volume tertile, 116 (9.0%) patients in the intermediate-volume tertile, and 110 (8.5%) patients in the high-volume tertile (χ2 p=0.44). After adjusting for potential confounding variables, a statistically significant difference in 30-day mortality (HR 1.48 (95% CI 1.05 to 2.08); p=0.02) was observed in PPCI performed by low-volume operators compared with high-volume operators, with no statistically significant difference in 12-month mortality (HR 1.26 (95% CI 0.96 to 1.65); p=0.09) (table 2, figures 1 and 2). There were no significant differences in adjusted rates of 30-day (HR 1.29 (95% CI 0.91 to 1.81); p=0.15) and 12-month mortality (HR 1.21 (95% CI 0.93 to 1.58); p=0.15) in intermediate compared with high-volume operators, or in 30-day (HR 1.15 (95% CI 0.83 to 1.60); p=0.40) and 12-month (HR 1.04 (95% CI 0.80 to 1.35); p=0.78) adjusted mortality between PPCI performed by low-volume and intermediate-volume operators.

Kaplan-Meier curves illustrating adjusted 30-day mortality, according to operator-volume tertiles. The reference tertile was high-volume operator status.20
{kind=link}
{kind=link}
Kaplan-Meier curves illustrating adjusted 12-month mortality, according to operator-volume tertiles. The reference tertile was high-volume operator status.20
Adjusted 30-day and 12 -month mortality for all variables included in Cox proportional hazards models analyses of operator volumes and potential confounders
There were no statistically significant differences in adjusted 30-day (HR 1.18 (95% CI 0.88 to 1.56); p=0.27) and 12-month mortality (HR 1.12 (95% CI 0.89 to 1.40); p=0.35) between visiting operators (n=20) and internal operators (n=8).
Other factors that were independently associated with mortality in our Cox PH models were advancing age, previous MI, pre-existing peripheral or cerebrovascular disease, diabetes mellitus, left-main coronary artery culprit vessel, and DTB time of ≥90 min (table 2). Left-main coronary artery as the culprit artery was most strongly associated with 30-day and 12-month mortality in this analysis.20
Discussion
We have shown that operator volume of PPCI for STEMI is independently and inversely associated with 30-day mortality, but not 12-month mortality, following the index event. In particular, PPCI performed by low-volume operators (<55 PPCI per year) was associated with significantly higher adjusted rates of mortality than those performed by high-volume operators (≥110 PPCI per year), suggesting that an operator volume–outcome relationship in PPCI exists at a threshold higher than current guideline recommendations.
Only four prior studies have specifically assessed outcomes based on operator volumes of PPCI, to a maximum of 30 days post-PPCI. Vakili et al demonstrated that in a cohort of patients who underwent PPCI in 1995, PPCI performed by high-volume operators (≥11 PPCI per operator per year) in high-volume centres (≥57 PPCI per centre per year) was associated with significantly lower in-hospital mortality (OR 0.51 (95% CI 0.26 to 0.99)) compared with low-volume operators in low-volume centres.17 However, contradictory to our findings, this difference was not observed when comparing low-volume operators with high-volume operators in high-volume centres. The difference in our findings might be explained by the advances in PPCI between 1995 and the period covered by our study in procedural techniques (radial artery access, smaller arterial sheaths), stent implantation (only 18% of patients received stents in their study, compared with 93.6% of patients in our study), pharmacotherapy (their study population predated the DAPT-era), and the acceptance of PPCI as the gold-standard reperfusion strategy in STEMI, following the landmark meta-analysis by Keeley et al.3 Importantly, we have also shown a difference in mortality at 30 days (compared with only in-hospital outcomes in their study). Although the relevance of this study in contemporary practice is unclear, this important study had informed the recommendation in the aforementioned AHA Guideline. As described in previous sections, the uptake of PPCI, advancements in techniques, technology and the evolution of secondary prevention since 1995 has been enormous.
Srinivas et al found that operator and institutional PPCI volumes were significantly associated with in-hospital mortality, reporting that in high-volume centres (>50 PPCI per year), patients who underwent PPCI by operators who performed >10 PPCI per year (in keeping with AHA recommendations of ≥11 PPCI per year) had lower in-hospital mortality compared with those who underwent PPCI by operators who performed ≤10 PPCI per year.18 They also found a statistically significant difference when the physician threshold was increased to 20 PPCI cases per year, but this difference was not observed at a threshold of 30 PPCI cases per year. However, their period of recruitment was between 2000 and 2002, which predated the routine utilisation of DAPT and transradial PPCI. The principal finding of our study is that even within a single high-volume institution, PPCI operator volume was independently associated with mortality at a higher operator volume threshold after a longer follow-up period than previously reported.
Hulme et al published their findings from the British Cardiovascular Interventions Society registry, assessing the operator–volume outcomes in all PCI from 2013 to 2014, including the select subgroup of patients undergoing PPCI.19 In their PPCI cohort of over 36 000 patients, they found that although unadjusted overall mortality was significantly lower with increasing operator volumes (determined according to quartiles rather than tertiles), annual operator volumes of <50 PPCI per year was not independently associated with in-hospital or 30-day mortality. Similar findings were observed in their study compared with ours. First, the rates of radial access was inversely proportional to operator volume. Second, the proportion of patients undergoing left-main PCI was higher in the high-volume group compared with the low-volume group. Third, the choice of P2Y12-receptor inhibitor differed between groups. This was an excellent study that addressed the operator–volume relationship specific to PPCI, in addition to other indications. However, although they have addressed the potential confounding factor of centre-related differences, given the multicentre nature of this registry, delays to reperfusion due to geographic variability may not have been accounted or corrected for, and could potentially confound findings in addition to intercentre variability. Nevertheless, it was an important study to suggest that in the UK, individual operator PPCI volume was not independently associated with 30-day mortality.
Most recently, Lee et al published their analysis of 8282 patients from the Korean PCI Registry, describing the association between operator volumes and in-hospital outcomes following PPCI in South Korea.15 Operator volumes were divided into three tertiles (low volume: <10 PPCI/year, moderate volume: 10–30 cases/year and high volume: >30 cases/year. No significant differences in outcomes were noted in this study, but a trend towards better outcomes was noted in the high-volume group. However, their analysis of outcomes according to operator and centre volume had demonstrated better outcomes in patients treated by high-volume operators in moderate-volume centres, but this finding was not observed in high-volume centres. There was also significant geographic variability in annual PPCI volume in this registry, which could potentially have introduced confounding factors, as per the study from Hulme et al.19 Crucially, only in-hospital outcomes were reported in this study.
Other studies that were not specific for PPCI have also shown a clear volume–outcome relationship in PCI, with low operator volume associated with significantly higher adverse events.4 7 10 25 Fanaroff et al published their analysis of 3.75 million PCI procedures between 2009 and 2015 (over 5.75 years), of which 6 27 501 cases were for STEMI, and found that in STEMI, low operator volume (<50 PCI per year) was associated with increased in-hospital mortality (OR 1.13 (95% CI 1.08 to 1.19) compared with high operator volume (>100 PCI per year).14 However, this was based on annual volume of PCI for all indications, rather than annual volume of PPCI for STEMI, which we have presented in this study. Our study is the first study showing a difference in 30-day mortality according to operator PPCI volume in a high-volume centre, in a ‘contemporary era’ of PPCI. We have also shown that differences in outcomes exist at a threshold far higher than the AHA-recommended minimum volume of ≥11 PPCI per year.
We have shown that differences in outcomes according to operator characteristics were driven by annual operator PPCI volume, rather than operator status. In our study, differences in procedural characteristics were identified that could potentially contribute to the variation in mortality observed. Lower rates of radial access for PPCI was observed in the lowest-volume tertile compared with other tertiles. There is extensive evidence showing that transradial PPCI is associated with improved clinical outcomes compared with transfemoral PPCI, including mortality, and this could have contributed to the difference in outcomes observed in the lowest volume operators compared with the highest volume operators.26–29 Higher rates of postprocedural TIMI 3 flow in the culprit artery were noted in the high-volume operator tertile compared with the low-volume operator tertile. This, in addition to radial artery access, may be a reflection of operator experience. In addition, PPCI can often involve clinical and procedural skills not usually involved in elective or urgent PCI, such as the use of thrombus aspiration, adjunct pharmacotherapy to manage large thrombus burden or slow/no-reflow, and the ability to safely perform PCI in the setting of active cardiac ischaemia, cardiogenic shock or refractory cardiac arrest. Therefore, acquisition of these skills, along with familiarity with institutional staff and equipment could also explain the volume–outcome relationship, although these factors are difficult to quantify objectively.
Although evidence suggests institutional PCI volumes are not associated with clinical outcomes,30 our finding that PPCI performed by operators performing <55 PPCI per year is associated with significantly higher probability of 30-day mortality compared with high-volume operators, should prompt re-examination of the AHA recommendation that ≥11 PPCI per year per operator is an acceptable operator volume for the provision of PPCI.20
Limitations
This is a single-centre study, therefore, our findings might not be generalisable to other regions or countries, as differences in the management of STEMI on a regional/national basis have been reported.20 23 However, as the management pathway adopted in our centre is in accordance with international practice guidelines, we are satisfied that our findings are broadly generalisable. Furthermore, differences in operator volumes in our study are not confounded by potential differences in performance between centres that theoretically can confound findings observed in multi-centre registry studies, but we recognise that in a smaller cohort of operators, differences observed may be due to other unidentified operator or systemic factors, rather than annual operator PPCI volumes. Our analyses were performed on observational registry data, and despite being prospectively collected, it was not possible to account for all potential confounders and unknown sources of bias. However, this is typical of prior analyses of operator volumes and outcomes in PCI, and is a robust methodological approach. The exclusion of patients undergoing PPCI in 2012 could have introduced bias into this study. However, this should not influence the overall result, as all other patients were obtained from an ‘unselected’ sample, and there were no significant changes in local protocol between 2011 and 2013. The difference between median case volumes between intermediate and high-volume operators was not numerically large, and clinically, it may not be relevant to divide these two groups. However, this was expected as the distribution of operator volume was right skewed. The difference in mean operator volumes in these two groups was strongly statistically significant (p<0.01). Therefore, division into tertiles based on institutional operator volumes was statistically justified. It is possible that some visiting operators may have performed in-hours PPCI in their base hospitals. However, according to the British Cardiovascular Intervention Society database, between 2012 and 2014, only a total of 25 PPCI were undertaken in this three calendar-year period in the four PCI-capable regional hospitals by 13 of the 21 visiting operators, which adds approximately 0.6 PPCI per year per operator. Therefore, the number of PPCI undertaken by visiting cardiologists in Leeds General Infirmary is likely to be representative of their true annual PPCI volume. Our event rates were relatively low compared with analyses of national databases, and therefore, play of chance could not be excluded. However, we are confident that our findings are objectively plausible considering the differences observed in transradial PPCI and postprocedural TIMI 3 flow in IRA, both of which are associated with improved outcomes following PPCI, and were observed to be more likely in PPCI undertaken by high-volume operators. In addition, the 8% lost to follow-up at 12 months that was observed is a potential source of bias. However, these patients were randomly distributed across the three tertiles such that the analysed population should be representative of the total population. Although a significant difference in 30-day mortality was demonstrated in this study, this difference no longer met statistical significance at 12 months. This could be due to individual patient factors. However, the possibility of the 8% of patients lost to follow-up at 12 months, or play of chance contributing to this difference could not be excluded. Although PPCI by low-volume operators was associated with higher risk-adjusted mortality compared with high-volume operators, it is important to recognise that PPCI operators, regardless of annual volume, provide an important life-saving service to any population. The benefit of this has to be weighed against that of thrombolysis, which has been shown to be less efficacious compared with PPCI. Finally, the results of this study should be considered hypothesis generating, prompting examination of larger national/international datasets for confirmation of findings.20
Conclusions
Low operator volume in PPCI for STEMI is independently associated with higher 30-day mortality compared with high operator volume. This suggests an operator volume–outcome relationship exists at a threshold higher than the current guideline recommendations. If this is confirmed, minimum operator volumes for PPCI may need to be adjusted to ensure optimal patient outcomes in the treatment of STEMI.20
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
National Health Service (NHS) approval from each regional hospital, and UK National Research Ethics Service approval (0911-11311/60) were obtained.
Acknowledgments
Analyses undertaken in this study were described in the 2017 MD Thesis by A. Krishnamurthy titled Determinants of clinical outcomes following primary percutaneous coronary intervention: the West Yorkshire Primary Percutaneous Coronary Intervention Outcome Study.
References
Footnotes
Contributors AK is the first author; undertaking primary analysis of data and preparation, revision of the manuscript, subsequent submission for peer-review, and is responsible for the overall content as he guarantor. AK accepts full responsibility for the work, conduct of the study, had access to the data, and controlled the decision to publish. All coauthors contributed to the production of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.