Article Text

Abstract
Aims Heart failure (HF) is associated with comorbidities which independently influence treatment response and outcomes. This retrospective observational study (January 2020–June 2021) analysed the impact of monthly HF multispecialty multidisciplinary team (MDT) meetings to address management of HF comorbidities and thereby on provision, cost of care and HF outcomes.
Methods Patients acted as their own controls, with outcomes compared for equal periods (for each patient) pre (HF MDT) versus post-MDT (multispecialty) meeting. The multispecialty MDT comprised HF cardiologists (primary, secondary, tertiary care), HF nurses, nephrologist, endocrinologist, palliative care, chest physician, pharmacist, clinical pharmacologist and geriatrician. Outcome measures were (1) all-cause hospitalisations, (2) outpatient clinic attendances and (3) cost.
Results 334 patients (mean age 72.5±11 years) were discussed virtually through MDT meetings and follow-up duration was 13.9±4 months. Mean age-adjusted Charlson Comorbidity Index was 7.6±2.1 and Rockwood Frailty Score 5.5±1.6. Multispecialty interventions included optimising diabetes therapy (haemoglobin A1c-HbA1c pre-MDT 68±11 mmol/mol vs post-MDT 61±9 mmol/mol; p<0.001), deprescribing to reduce anticholinergic burden (pre-MDT 1.85±0.4 vs 1.5±0.3 post-MDT; p<0.001), initiation of renin–angiotensin aldosterone system inhibitors in HF with reduced ejection fraction (HFrEF) with advanced chronic kidney disease (9% pre vs 71% post-MDT; p<0.001). Other interventions included potassium binders, treatment of anaemia, falls assessment, management of chest conditions, day-case ascitic, pleural drains and palliative support. Total cost of funding monthly multispecialty meetings was £32 400 and resultant 64 clinic appointments cost £9600. The post-MDT study period was associated with reduction in 481 clinic appointments (cost saving £72150) and reduced all-cause hospitalisations (pre-MDT 1.1±0.4 vs 0.6±0.1 post-MDT; p<0.001), reduction of 1586 hospital bed-days and cost savings of £634 400. Total cost saving to the healthcare system was £664 550.
Conclusion HF multispecialty virtual MDT model provides integrated, holistic care across all healthcare tiers for management of HF and associated comorbidities. This approach is associated with reduced clinic attendances and all-cause hospitalisations, leading to significant cost savings.
- Health Care Economics and Organizations
- Outcome Assessment, Health Care
- Quality of Health Care
- Heart Failure
- Pharmacology
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- Health Care Economics and Organizations
- Outcome Assessment, Health Care
- Quality of Health Care
- Heart Failure
- Pharmacology
What is already known on this topic
Heart failure is associated with several comorbid health conditions (multimorbidity) which independently influence outcomes as well as response to treatment.
What this study adds
This study assesses the impact of multispecialty multi-morbidity input into the management of comorbidities and thereby the effect on all-cause outcomes.
How this study might affect research. practice or policy
Results of this study illustrate that multispecialty management of comorbidities associated with heart failure, may not only improve all-cause outcomes but could also prove to be cost beneficial.
Introduction
Heart failure (HF) is a complex clinical syndrome, representing the final common pathway of many different pathological processes and associated with high mortality and frequent hospital admissions.1 There are an estimated 64.3 million cases of HF worldwide.2 This global burden is expected to increase due to an ageing population, with 80% of hospitalisations occurring in those aged >65 years.3 Significantly, hospitalisation in people with HF confers a poor prognosis with a 1-year mortality of 31%, 5-year mortality of 63% and 10-year mortality of 82% and these outcomes are worse in comparison to those who do not require hospitalisation.4
HF is frequently characterised by multimorbidity (coexistence of two or more long-term conditions) and these comorbid conditions (long-term conditions) that can influence the management of HF and adversely affect outcomes. These other conditions include other cardiovascular diseases such as ischaemic heart disease (IHD), atrial fibrillation (AF) and hypertension and non-cardiovascular comorbidities such as chronic kidney disease (CKD) (41%), anaemia (37%), diabetes mellitus (type 1 or type 2) (DM-21%), chronic obstructive pulmonary disease (COPD) (24%), a burden of polypharmacy and frailty.5 6 Most people with HF have at least one comorbidity6 7 and up to 40% of patients with HF have ≥5 comorbidities (this group contributed to >80% of the overall in-hospital stay in one study).8 The number of comorbidities is higher among patients with HF with preserved ejection fraction (HFpEF) than in patients with HF with reduced ejection fraction (HFrEF) and with a more profound impact on outcomes.9–13 In addition, non-cardiac comorbidities independently affect response to treatment, influence disease severity and HF outcomes such as hospitalisation, quality of life and mortality.7 12–19 The burden of comorbidities is also progressively increasing with time.13 20This level of multimorbidity and complexity can be most effectively managed by a multidisciplinary team (MDT), an approach endorsed by both the European Society of Cardiology (class 1A recommendation)21 and the American Heart Association (class 1B recommendation).21 However, there is little detail in the guidelines about the composition or remit of such an MDT. There is also a dearth of evidence currently regarding whether management of comorbidities by relevant specialists in consultation with HF specialists can improve HF outcomes.
The aim of this study is to assess the impact of multispecialty input on the optimisation of comorbidities, all-cause hospitalisations, outpatient clinic attendances and mortality in patients with HF.
Methods
Study setting and time period
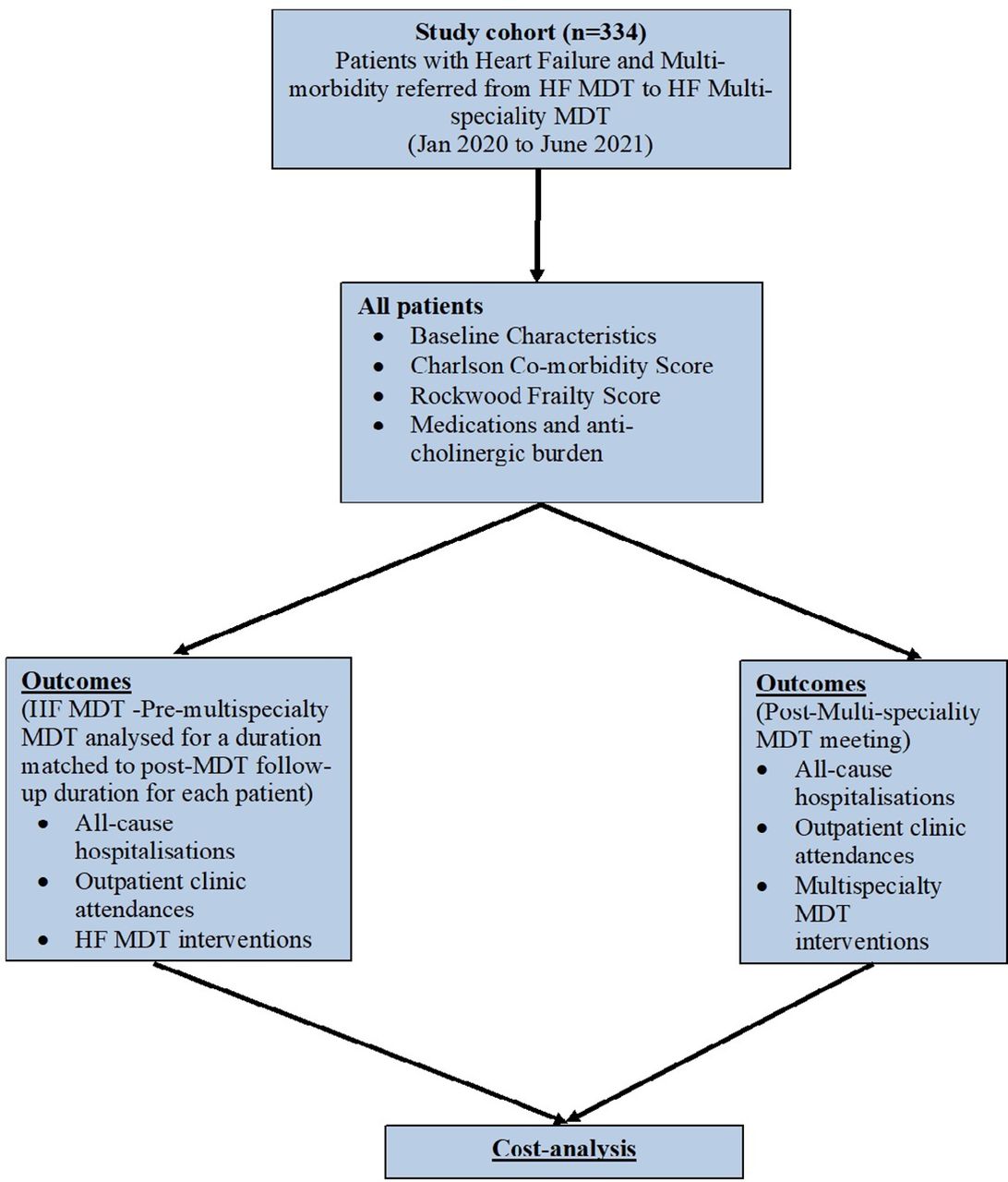
It was conducted as an observational retrospective cohort study in a British University teaching hospital, looking at the impact of a multispecialty HF MDT meeting on care models and outcomes in a HF population. We studied outcomes of patients with HF and multimorbidity referred from the HF MDT to our monthly virtual multispecialty meetings from January 2020 to June 2021 and followed up for equal amounts of time pre and post recruitment. Figure 1 illustrates the study flow chart diagram. We followed the guidelines (The Strengthening the Reporting of Observational Studies in Epidemiology) for reporting observational studies.22
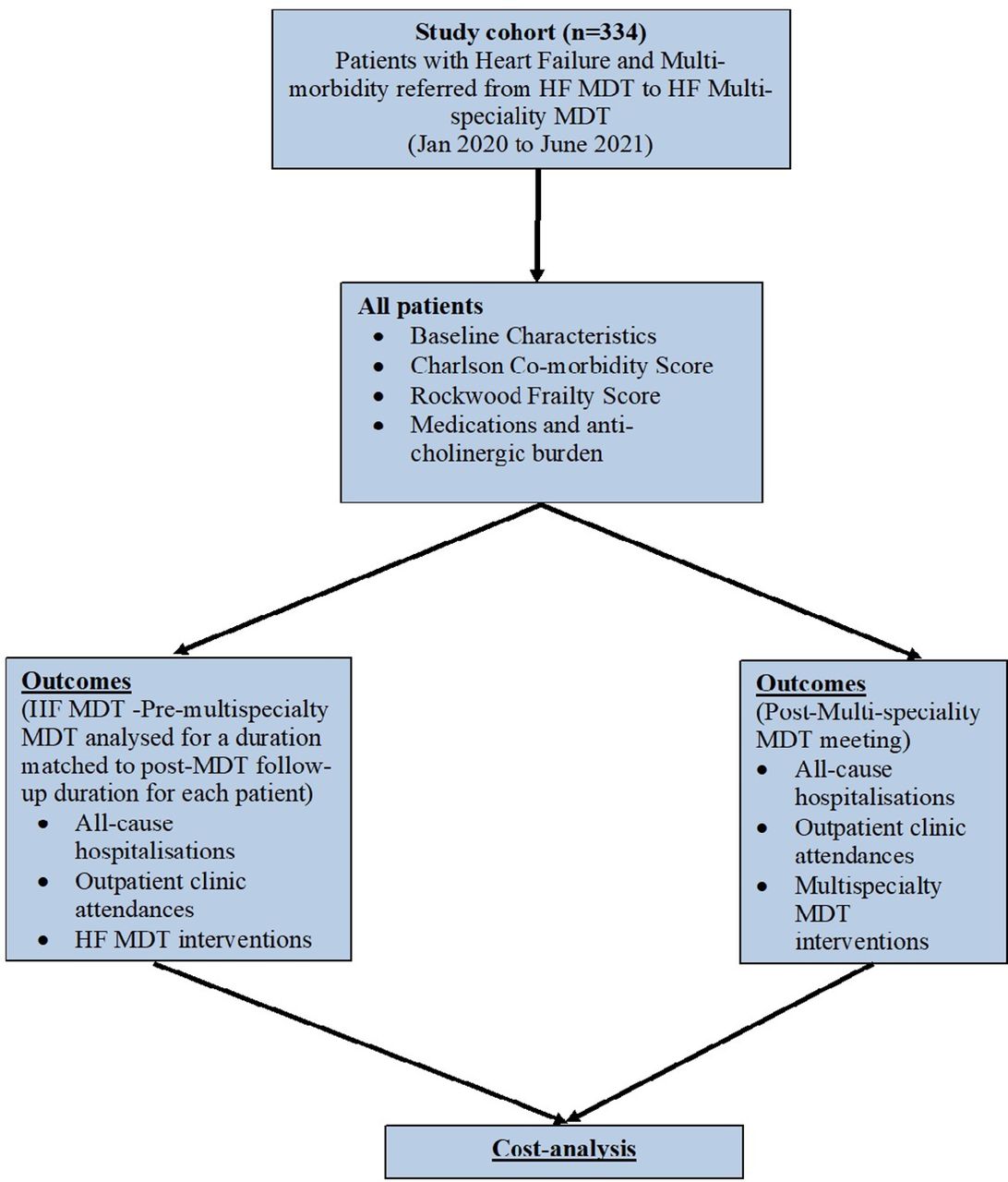
Study flow chart. HF, heart failure; MDT, heart failure.
Multispecialty MDT meeting format
Prior to prior to January 2020, our HF MDT consisted of HF cardiologists and HF specialist nurses. Since January 2020, the new model of Liverpool Multi-specialty regional HF MDT meetings has been funded by Liverpool Single Services Cardio-respiratory Group (from Liverpool Clinical Commissioning Group) and Liverpool University Hospitals NHS Foundation Trust. The multispecialty meeting is conducted monthly via videoconferencing. Sources of referral to the multispecialty MDT include community HF teams, hospital HF teams (secondary and tertiary care) and other specialty teams, using a dedicated referral form (online supplemental file 2). The multispecialty MDT consist of HF cardiologists from the community, secondary care and tertiary care, HF specialist nurses from the community and hospital, nephrologist, endocrinologist, palliative care specialist, chest physician, geriatrician, pharmacist and pharmacologist. Individualised discussions at the multispecialty MDT meeting include optimisation of HF therapies, assessment of frailty, comorbidities, cardiorenal metabolic status, specialist input into any complex chronic respiratory pathologies, need for falls risk assessment, cognitive dysfunction, rationalisation of polypharmacy burden (particularly anticholinergic burden, ACB), medication compliance and need for advanced care planning discussions or community palliative care where appropriate. Recommendations are made as consensus from the multispecialty meeting where each patient’s case is discussed once. These are then conveyed electronically or through post to the referrers, the electronic record of each discussed patient is also updated with these recommendations and the MDT consensus discussed with each patient.
Supplemental material
Demographic and clinical details
We collected demographic data, comorbidities such as DM, hypertension, IHD, COPD or a pre-existing malignant condition and medication history as well as ACB (ACB which is the cumulative impact of using multiple medications with anticholinergic properties concomitantly). The ACB is calculated by identifying medications with anticholinergic properties and assigning a score between 1 and 3 according the anticholinergic activity of the medication.23 Furthermore, we computed the Charlson Comorbidity Index (CCI)24 and the Rockwood clinical frailty score.25 Patients were followed up for equal (matched) periods of time pre and post multi-specialty MDT meeting, so ‘each patient acted as their own control’ and the analysis compared outcomes during the HF MDT period vs those in the HF Multispecialty MDT period.
Outcome measures
Outcome measures assessed were all-cause hospitalisations and outpatient clinic attendances for an equal period pre and post multispecialty MDT meeting. We also assessed other measures such as advanced HF management (device therapy, transplant referrals), referrals to integrated palliative care services, burden of polypharmacy and cost analysis. Statistical comparisons were made for MDT interventions as well as outcomes, comparing the pre-multispecialty MDT (‘HF MDT’) with those of the multispecialty HF MDT time period, for matched durations.
Statistical analysis
For the descriptive statistics of our patient population, we represented continuous variables as means with SD or medians with interquartile ranges in the case of non-parametric data. Categorical variables were represented with percentages and analysed using χ2 test. Statistical comparisons were made for parametric data using paired samples Student’s t-test and for non-parametric data using Mann-Whitney test. Statistical analysis was carried out using the Statistical Package for the Social Sciences (SPSS V.23.0, IBM).
Results
Demographic details
A total of 334 patients were discussed through virtual MDT meetings from January 2020 to June 2021. We collated baseline patient characteristics as illustrated in table 1. This service model continued uninterrupted during the COVID-19 pandemic. The mean age of patients discussed was 72.5±11 years and follow-up duration was 13.9±4 months. Forty-three per cent of the patients discussed were female and 45% of patients had a diagnosis of HFpEF.
Patientcharacteristics and comparison of 2 cohorts of patients—HFrEF/HFmrEF versus those with HFpEF
The mean age-adjusted Charlson Comorbidity Index was 7.6±2.1 and Rockwood Frailty Score was 5.5±1.6, indicating a mild to moderate degree of frailty. There was significant polypharmacy burden as indicated by the mean number of medications of 12.1±3.9 among the whole cohort.
As illustrated in table 1, we also compared baseline characteristic and comorbidities based on EF, between two groups (HFrEF and heart failure with mildly reduced ejection fraction (HFmrEF) vs HFpEF). The HFpEF group was older, consisted of more women, had a lower prevalence of IHD and higher prevalence ofhypertension and CKD. The HFpEF group also had a significantly higher Charlson Comorbidity Index and showed a trend towards greater frailty (although this was not statistically significant).
Clinical recommendations
Medicines optimisation
Consensus recommendation was made from the MDT regarding optimisation of prognostic medications. Table 2 details the medicines optimisation recommendations from the multi-specialty MDT meetings. This included initiation or continuation of prognostic HFrEF therapy such as ACE-ACE inhibitor/angiotensin receptor blocker-ARB in 32 patients with HFrEF and CKD4 up to eGFR 20 mL/min/1.73 m². A higher number of patients were prescribed potassium binders to treat hyperkalaemia due to renin-angiotensin-aldosterone system inhibitor (RAASi) therapy (2 patients pre-MDT vs 13 patients post-MDT). These interventions contributed to a significant improvement in prescription of quadruple HFrEF therapy (ACE inhibitor/ARB/ angiotensin receptor neprilysin inhibitor, beta-blocker, mineralocorticoid receptor antagonist-MRA and sodium-glucose co-transporter2 inhibitor -SGLT2i) which increased from 46% premultispecialty MDT to 71% postmultispecialty MDT; p<0.001.
Treatment optimisation and other interventions at multispecialty MDT meeting
SGLT2i addition was recommended for improved cardiorenal metabolic status in 91 patients with type 2 diabetes and HF. There was also a significant improvement in the HbA1c levels noted during the post-MDT period. As also detailed in table 2, appropriate deprescribing of polypharmacy was also recommended in order to significantly reduce the ACB (ACB 1.85±0.4 pre-MDT vs ACB 1.5±0.3 post-MDT. It is likely that this intervention contributed to the significant reduction of hospitalisations due to adverse drug reactions (12% pre-MDT to 5% post MDT; p=0.003).
Advanced HF therapies
(53/334–16%) patients underwent internal cardiovertor-defibrillator (ICD-26/53 patients) or cardiac resynchronisation therapy (CRT-14 patients) pacemaker implant (13 patients underwent CRTD) as a result of consensus recommendations from the multispecialty MDT and 11/334 (3%) patients were referred for transplant assessment. (16/334). The proportion of patients who underwent device therapy or advanced HF therapy referrals, was similar in numbers in the two study periods.
Other recommendations
Treatment of anaemia improved (24% pre-Multispecialty MDT vs  ; p<0.001) though prescription of intravenous iron instead of oral iron, erythropoietin, folic acid and vitamin B12 supplements where indicated. Five per cent of patients were referred to dialysis assessment clinics and 10 patients were instituted on dialysis. Nine per cent of patients were referred to the falls assessment clinic (7 patients referred premultispecialty MDT and 23 patients postmultispecialty MDT. As also demonstrated in table 2, the postmultispecialty MDT period was associated with a higher proportion of patients who underwent investigations and treatment optimisation for chronic obstructive airway disease, drain of pleural effusion and new diagnosis of sleep apnoea. Of 334, 37 (11%) patients required community palliative care, 9 of these patients required admission to a hospice and 11 patients required deactivation of their ICD as a part of advanced care planning palliative care. Overall mortality of this cohort during follow-up was 21% (70/334).
; p<0.001) though prescription of intravenous iron instead of oral iron, erythropoietin, folic acid and vitamin B12 supplements where indicated. Five per cent of patients were referred to dialysis assessment clinics and 10 patients were instituted on dialysis. Nine per cent of patients were referred to the falls assessment clinic (7 patients referred premultispecialty MDT and 23 patients postmultispecialty MDT. As also demonstrated in table 2, the postmultispecialty MDT period was associated with a higher proportion of patients who underwent investigations and treatment optimisation for chronic obstructive airway disease, drain of pleural effusion and new diagnosis of sleep apnoea. Of 334, 37 (11%) patients required community palliative care, 9 of these patients required admission to a hospice and 11 patients required deactivation of their ICD as a part of advanced care planning palliative care. Overall mortality of this cohort during follow-up was 21% (70/334).
Hospitalisations
As shown in figure 2, the number of all-cause hospitalisations was reduced significantly from 371 hospitalisations (4126 bed-days) pre-MDT to 205 post-MDT (2540 bed-days) (pre-MDT 1.1±0.4 vs .0.6±0.2 post MDT; p<0.001), leading to a saving of 1586 bed-days and estimated cost saving £634 400 (average cost per bed day £400.26 As also shown table 1, these significant reductions in hospitalisation were seen irrespective of ejection fraction.
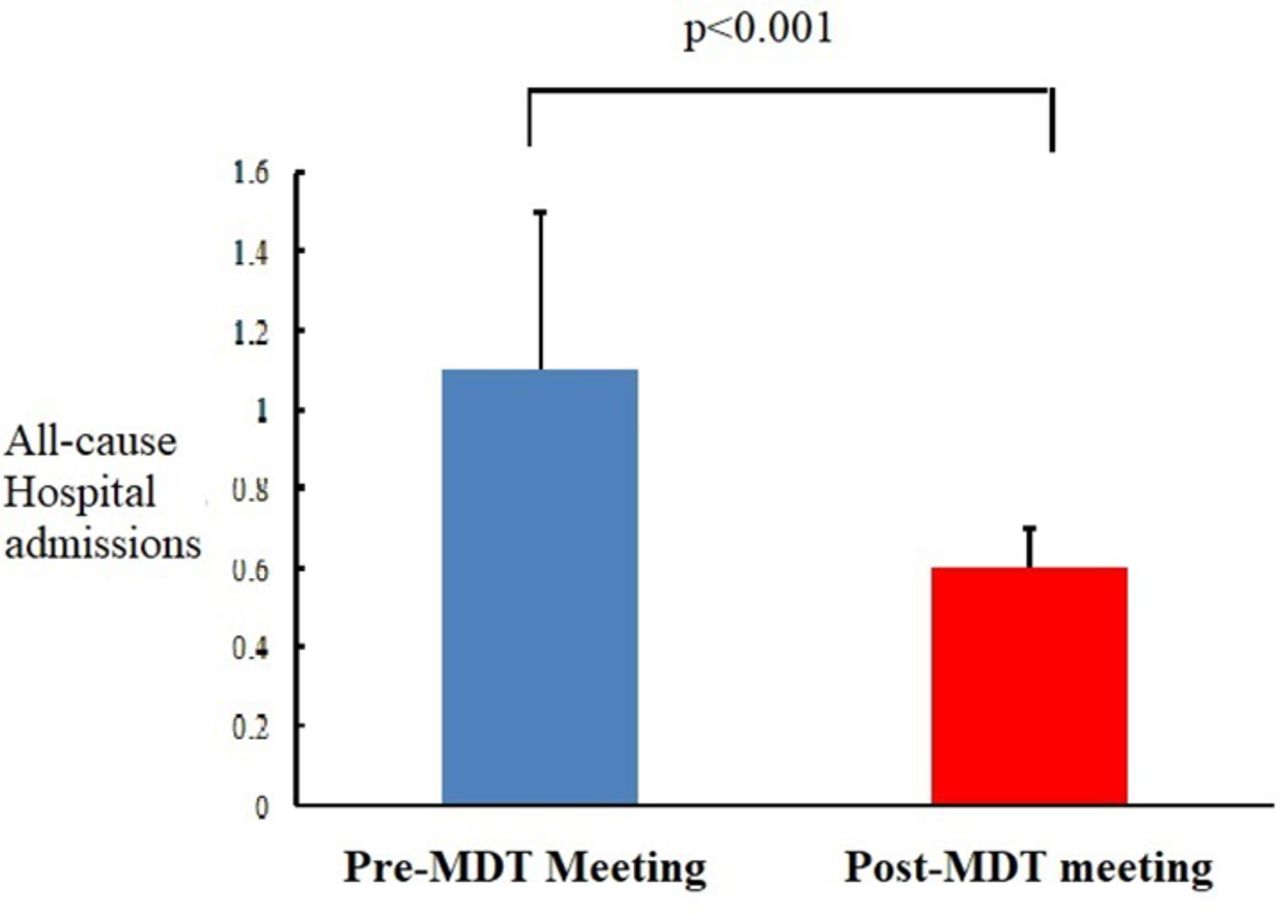
Comparison of all-cause hospitalisations premultispecialty and postmultispecialty MDT meeting. MDT, multidisciplinary team.
We performed further analysis of the cause of these hospitalisations (with regards to the aetiology of hospitalisation) as well as the effect of the multispecialty MDT based on the aetiology. In the pre-MDT period, 211 out of 371 hospitalisations (57% and 1900 bed-days) were due to HF and the remaining 160 hospitalisations (43% and2226 bed-days) due to other causes (’non-HF’).
In the post-MDT period, there were 135 hospitalisations due to HF (36% reduction; p=0.03 and contributed to 1273 bed-days. In this same period, there were 70 hospitalisations due to non-HF causes (55% reduction; p=0.04 and contributed to 1267 bed-days). Figure 3 illustrates the various non-HF causes of hospitalisation in people with HF and shows a significant reduction in hospitalisation post-MDT in these conditions. The non-HF causes of hospitalisations included cardiac (IHD, AF, valve disease), renal (acute kidney injury or electrolyte imbalances), chest (exacerbation of lung disease such as COPD/asthma, pleural effusion), diabetes (hypoglycaemia/hyperglycaemia, infected ulcer), adverse drug reactions, social reasons/need for palliative support and other reasons (eg, surgical conditions).
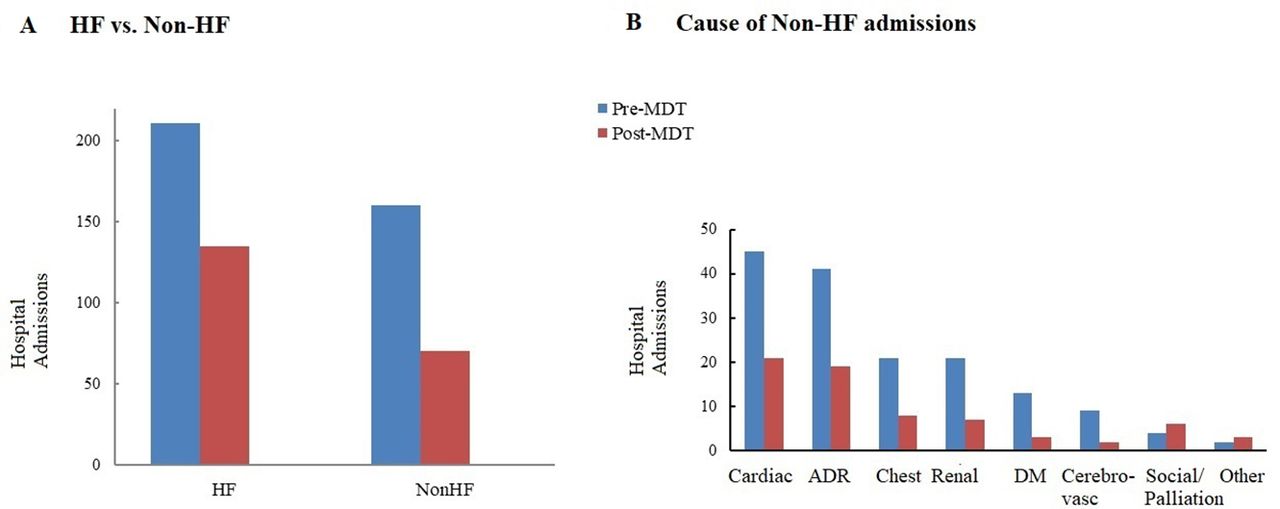
Comparison of hospitalisation premultispecialty and postmultispecialty MDT based on causes. DM, diabetes mellitus; HF, heart failure; MDT, multidisciplinary team; ADR, Adverse Drug Reaction
Outpatient attendances
The number of outpatient clinic attendances reduced in the post-MDT meeting was 534. There were 946 outpatient appointments pre-MDT meeting and 465 appointments post-MDT. There was a 51% reduction in HF appointments (481 pre vs 242) post and 55% reduction in non-HF appointments (465 vs 223). Further analysis of the non-HF appointments (shown in table 3) revealed that there were reductions in the majority of causes of outpatients clinic appointments (cardiac, renal, diabetes, chest, geriatric, cerebrovascular and other causes but an increase in clinical appointments for falls clinic and palliative clinic. This reduced inconvenience to patients and also potentially saved patients money. This includes avoidance of need for travel as well as waiting time in clinic (average 51.3 minutes),27 transport and parking costs (average saving of £5.52 per patient per appointment by car and £4.60 by bus).28 There was also the added positive environmental impact through carbon footprint reduction (in this study 554 kgCO2).
Comparison of OPD appointments premultispecialty and postmultispecialty MDT meeting
Economic analysis
We also performed an economic analysis of the impact of the virtual multispecialty MDT. This is also illustrated in table 4. The total cost of funding the multispecialty MDT meeting was 0.5 programmed activity NHS rates29 per specialty (£1800 per meeting and £32 400 for the duration of the study (January 2020–June 2021). The 64 clinic appointments that generated as a result of recommendations from the multispecialty MDT meetings cost an estimated £9600 (£150 per outpatient clinic.26 However, the MDT meetings were also associated with a reduction in 534 clinic appointments (cost saving £80 100). As detailed above, a reduction in all-cause hospitalisations in the post-MDT period was associated with a saving of 1586 bed-days and estimated cost saving £634 400. As shown in table 4, the total saving to the healthcare system was £664 550.
Economic analysis—healthcare savings
Discussion
Several previous studies have shown the coexistence and adverse impact of multimorbidity in patients with HF. However, this is the first study to demonstrate that multispecialty, multidisciplinary management of comorbidities with integration of community, secondary and tertiary care HF specialists, is associated with reduced all-cause hospitalisations and outpatient clinic attendances (HF and non-HF) in people with HF irrespective of the ejection fraction. The multispecialty MDT also optimised the care of multiple comorbidities and facilitated timely involvement of relevant specialties.
It is important to focus on the management of multimorbidity along with the management of HF itself. Other studies have demonstrated that HF contributes to a smaller proportion of the burden of hospitalisation (less than 20%), non-cardiovascular causes contribute to more than 60% of the burden of hospitalisations.5 30 Small studies (randomised and observational) have shown that treatment of individual comorbidities such as sleep apnoea,31 anaemia,32 AF33 and obesity,34 can reduce hospitalisation and mortality in HF patients. Our study has also shown that multispecialty input into comorbidities and treatment optimisation can lead to a significant reduction in hospitalisations due to non-HF causes. A focus on management of comorbidities is relevant for all types of HF, but particularly for HFpEF in which there is a higher burden of comorbidities as shown by the significantly higher Charlson Comorbidity Index in this cohort of patients. In patients with HFpEF, only SGLT2 inhibitors have recently been demonstrated to lead to a reduction in the composite outcome of cardiovascular death or hospitalisation.35Additionally, while quadruple therapy and devices can significantly improve outcomes in people with HFrEF, coexistence of multimorbidity such as CKD may deter clinicians from prescribing prognostic RAASi therapy and a multispecialty MDT can help improve prescription of this class of medications which are evidence based for improved cardiorenal outcomes. Previous data from our centre have also demonstrated that a joint cardiorenal MDT meeting can reduce the need for further cardiology or renal outpatient follow-up in nearly 50% of patients.36 However, there is significant variation and disparity in the management of HF and associated comorbidities depending on the geographical location of the patient and healthcare professional.37 Specialists frequently focus on a single disease entity, potentially with a deleterious effect on other organ/systems (one such example is the occurrence of worsening renal function in patients with HFrEF during decompensated HF, prompting cessation of RAASi therapy and in turn leading to worsening HF outcomes).
Disease management programmes incorporating MDT input from dietician, social worker, physical therapist and pharmacist have shown a significant reduction in 30-day readmissions rates,38 however, we note the variable definition of the constitution of a HF MDT and the variable effects of MDT input into HF outcomes.39 Members of the MDT have included HF specialist nurses, HF consultants, pharmacists, dieticians, social care workers, physiotherapists, palliative care specialists and psychologists. The largest study of MDT intervention (Co-ordinating study evaluating Outcomes of Advising and Counselling in Heart failure (COACH) study) showed neutral outcomes in terms of HF hospitalisations or mortality.40 It is possible that the lack of specialist input into intensive management of comorbidities may have diluted the wide-ranging beneficial effects of MDT input. The strategy of incorporation of other specialists (nephrologist, diabetologist, geriatrician, chest physician, pharmacologist, palliative care) to address comorbidities simultaneously along with HF specialists, is novel and timely, particularly considering the cardiac, renal and metabolic impact of HF therapies such as the SGLT2 inhibitors. Our study has also shown that incorporation of a pharmacist as well as clinical pharmacologist in the MDT, can help with reduction in ACB due to polypharmacy and the associated deleterious effects. This intervention was associated with a significant reduction in hospitalisations due to adverse drug reactions.
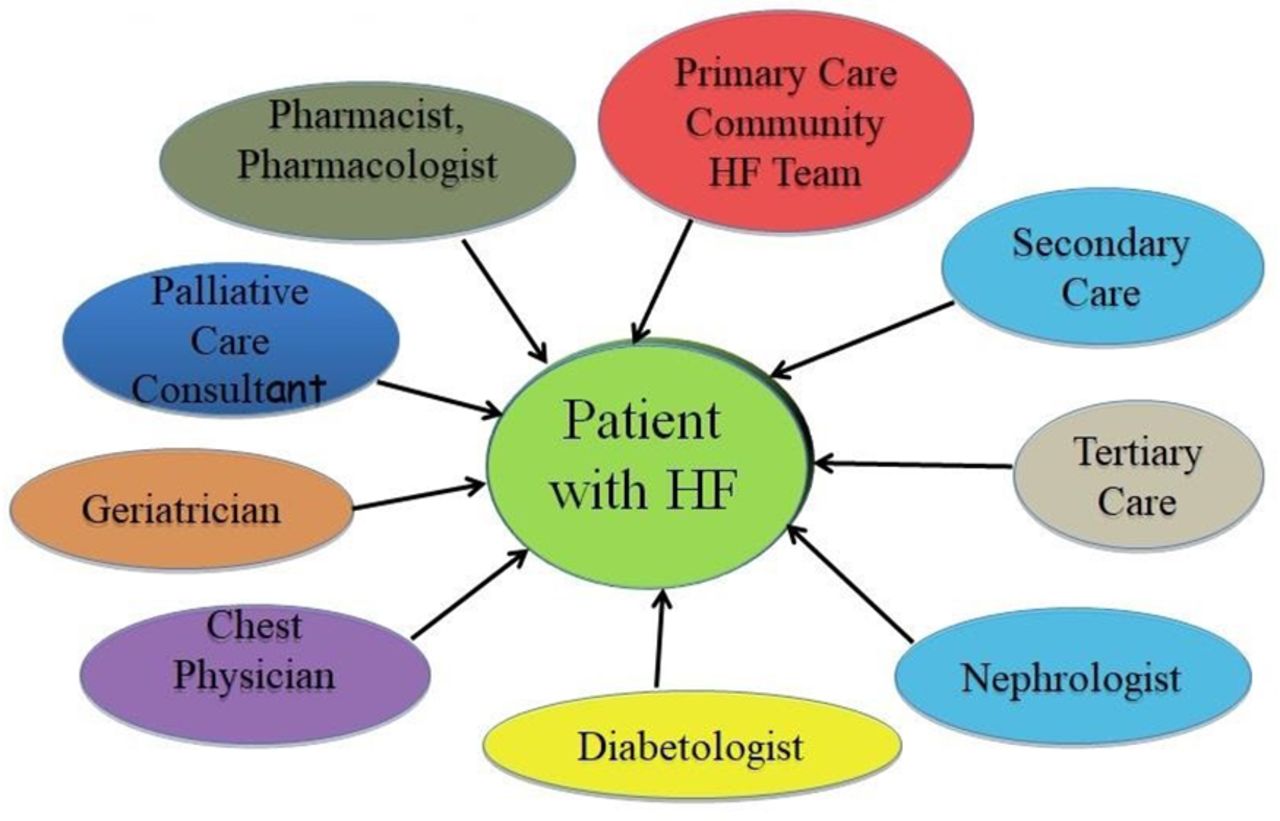
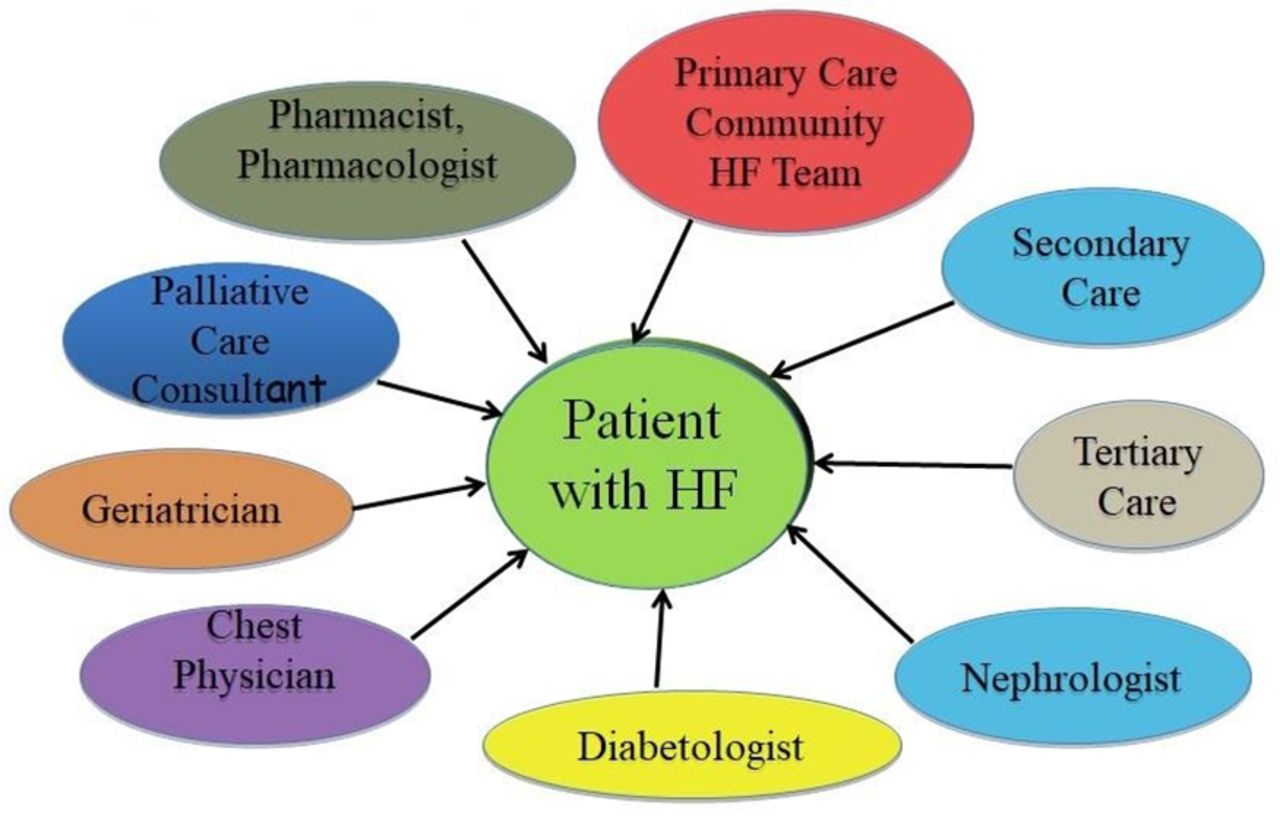
Our service model (figure 4) exemplifies individualised, patient-centric, holistic care using a consensus multispecialty approach targeted to the management of HF and comorbidities jointly. The need to address and manage comorbidities frequently prompts referral to other specialty outpatient clinics. Repeated outpatient clinic attendances are inconvenient to otherwise frail and often less mobile patients. Frailty in people with HF is an important determinant of outcomes41 and our study has shown that people with HF can have associated mild to moderate degree of frailty. We have demonstrated that a virtual multispecialty MDT is associated with savings of time, travel and cost and a significant reduction in interspecialty referrals/outpatient clinic attendances, thereby of particular benefit for people with frailty and HF.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Integrated multispecialty MDT model illustrating the team members involved in the MDT meetings. HF, heart failure; MDT, multidisciplinary team.
Virtual MDT clinics have been particularly relevant during the COVID-19 pandemic when this particularly vulnerable cohort prefer to avoid travel and minimise the risk of hospital-acquired infection (findings supported by our national HF patient survey regarding the impact of the COVID-19 pandemic on HF services).42 Our virtual multispecialty MDT model importantly ensured that the management of patients with HF continued uninterrupted throughout the COVID-19 pandemic, while minimising the need for patients to attend face-to-face outpatient clinic appointments.
We acknowledge limitations of this study including the observational nature; the efficacy of this service model maybe be best evaluated through a randomised controlled trial. Limitations of the virtual MDT approach also include the potential for miscommunication in view of lack of patient presence during the meeting. This was minimised by spoken and written discussions with the patient prior to and subsequent to the meeting. The model requires robust service planning to ensure attendance of multiple specialists and members of the MDT.
In conclusion, we demonstrate that an integrated and virtual multidisciplinary input is associated with improved HF outcomes through a reduction in all-cause hospitalisations and clinic attendances and is not only patient-centred but also cost-effective. Application of this model could be considered the gold-standard approach in addressing multimorbidity in patients with HF, however, this will need to be validated through assessment in a randomised study comparing outcomes from a HF MDT versus multispecialty MDT in addition to HF MDT.
Supplemental material
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Acknowledgments
Heart Failure Specialist Nurses (Aintree University Hospital, Community Heart Failure Team and LHCH)
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @cardiologyMCR, @DrRajivsankar
Contributors HE: data collection, data analysis and interpretation, drafting the article, critical revision of the article, final approval of the version to be published. LW; critical revision of the article, final approval of the version to be published. KM: data collection, data analysis and interpretation, critical revision of the article, final approval of the version to be published. EO: critical revision of the article, final approval of the version to be published. HD: critical revision of the article, final approval of the version to be published. MK: critical revision of the article, final approval of the version to be published. AR: critical revision of the article, final approval of the version to be published. JB: critical revision of the article, final approval of the version to be published. JH: critical revision of the article, final approval of the version to be published. NH-E: critical revision of the article, final approval of the version to be published. JB: critical revision of the article, final approval of the version to be published. AA: critical revision of the article, final approval of the version to be published. CW: critical revision of the article, final approval of the version to be published. DC: critical revision of the article, final approval of the version to be published. RS: conception or design of the work, data collection, data analysis and interpretation, drafting the article, critical revision of the article, final approval of the version to be published, and responsible for the overall content as guarantor.
Funding The MDT meetings are funded by the Liverpool Single Services Cardio-Respiratory Operation Group, Liverpool Clinical Commissioning Group and Liverpool University Hospitals NHS Foundation Trust.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.