Article Text

Statistics from Altmetric.com
- intravenous drug use
- right sided endocarditis
- transthoracic echocardiography
- transoesophageal echocardiography
If William Osler were alive today he would no doubt remark on the fundamental change in the nature of the disease that he originally described. Staphylococcal endocarditis in injection drug users is now the dominant form of the disease in many urban communities where there is a high incidence of injection drug use and homelessness. At our institution (a tertiary care, university affiliated hospital in inner Vancouver), 63% of 116 hospitalisations between 1994 and 2000 for infective endocarditis (IE) were in injection drug users. Right sided endocarditis accounts for 10% of all IE in population based surveys1 and a higher proportion of IE in injection drug users. Modern echocardiographic techniques have considerably augmented our ability to diagnose IE and to understand its natural history. Despite this, there are many areas in which our understanding of right sided IE remains incomplete.
Right sided IE has a significant morbidity and mortality that adds a notable economic burden to stretched inner city health care facilities. The challenges of caring for this population of patients should not be underestimated and demands a logical and coordinated approach among care providers and physicians from a variety of specialties. This article reviews aspects of the epidemiology, clinical features, diagnosis, and treatment of right sided IE in injection drug users.
EPIDEMIOLOGY AND PREDISPOSING FACTORS
Although right sided IE may occur in association with congenital heart disease and instrumentation of the right heart, it is overwhelmingly a disease of injection drug users, at least in western populations. Among injection drug users presenting with fever, 13% will have echocardiographic evidence of IE.2 If injection drug users with bacteraemia from an inner city demographic are considered, up to 41% will have evidence of IE.3
The pathogenic mechanisms that explain the increased prevalence of right sided IE in injection drug users are not fully elucidated. Damage to the right sided valves from injected particulate matter in the setting of injected bacterial loads is thought to be important, while subtle abnormalities of immune function may also have a role in pathogenesis.
In keeping with the demographic characteristics of injection drug use, this disease occurs most commonly in young males in their 20s and 30s. At our institution, which may represent a peculiar demographic, males and females are equally affected. Before infection the tricuspid valve is usually structurally normal. Reinfection of a tricuspid valve that has been damaged by previous IE accounts for a significant proportion of cases and can add to the difficulty of echocardiographic interpretation.4 It seems logical that valves previously damaged by infection are more likely than normal valves to become infected although we could find no published evidence to support this contention.
Earlier reports of IE in injection drug users emphasised the dominance of right sided involvement,3 and certainly this has been our experience. We reviewed 105 patients at our institution that met the Duke criteria for IE between April 1995 and June 1998. Of these, 86% were exclusively right sided, while 14% had left sided involvement. In some recent reports, however, the incidence of left and right sided endocarditis in this population has been similar.5 The tricuspid valve is most frequently involved followed by the mitral and then the aortic valve. Concurrent involvement of both left and right sided valves is not infrequent.5 In right sided IE it is almost always the tricuspid valve that is involved. One study of injection drug users found vegetations involving the tricuspid valve in 127 episodes, the pulmonary valve in four, and both valves in one instance.6 In our review of cases of right sided IE we found that 85 of 86 cases involved the tricuspid valve with only one involving the pulmonary valve. Involvement of other right sided structures such as the eustachian valve has been reported but is rare.
The dominant infective organism is Staphylococcus aureus, in most series accounting for around 70% of infections, with the remainder being caused mainly by streptococcal species or, less frequently, by Gram negative organisms, fungi or diphtheroids. Pseudomonal infections may have a predilection for multi-valve involvement. Infections with unusual organisms and polymicrobial infections do occur, probably as the result of the injection of contaminated diluent, but are relatively unusual. Blood cultures are positive in a high proportion of cases of right sided IE. When culture negative right sided IE occurs, it is usually as a result of antibiotic use before the drawing of blood cultures. Bartonella infection has been described as a cause of culture negative IE in a homeless inner city population, and in right sided IE.
Although patterns of drug use in relation to IE have not been extensively studied, cocaine use may be a risk factor, presumably as a consequence of the much higher frequency of injections than in heroin users. The reported prevalence of HIV disease in patients with right sided IE is variable. In a Spanish series of injection drug users with IE, 76% were HIV positive.7 In our institution of 100 consecutive injection drug users with suspected endocarditis, 58 were HIV positive.8 In a cohort of injection drug users with IE, those who were HIV positive were more likely to exhibit right sided involvement.7 Advanced HIV infection is probably a risk factor for IE.9
CLINICAL MANIFESTATIONS AND COMPLICATIONS
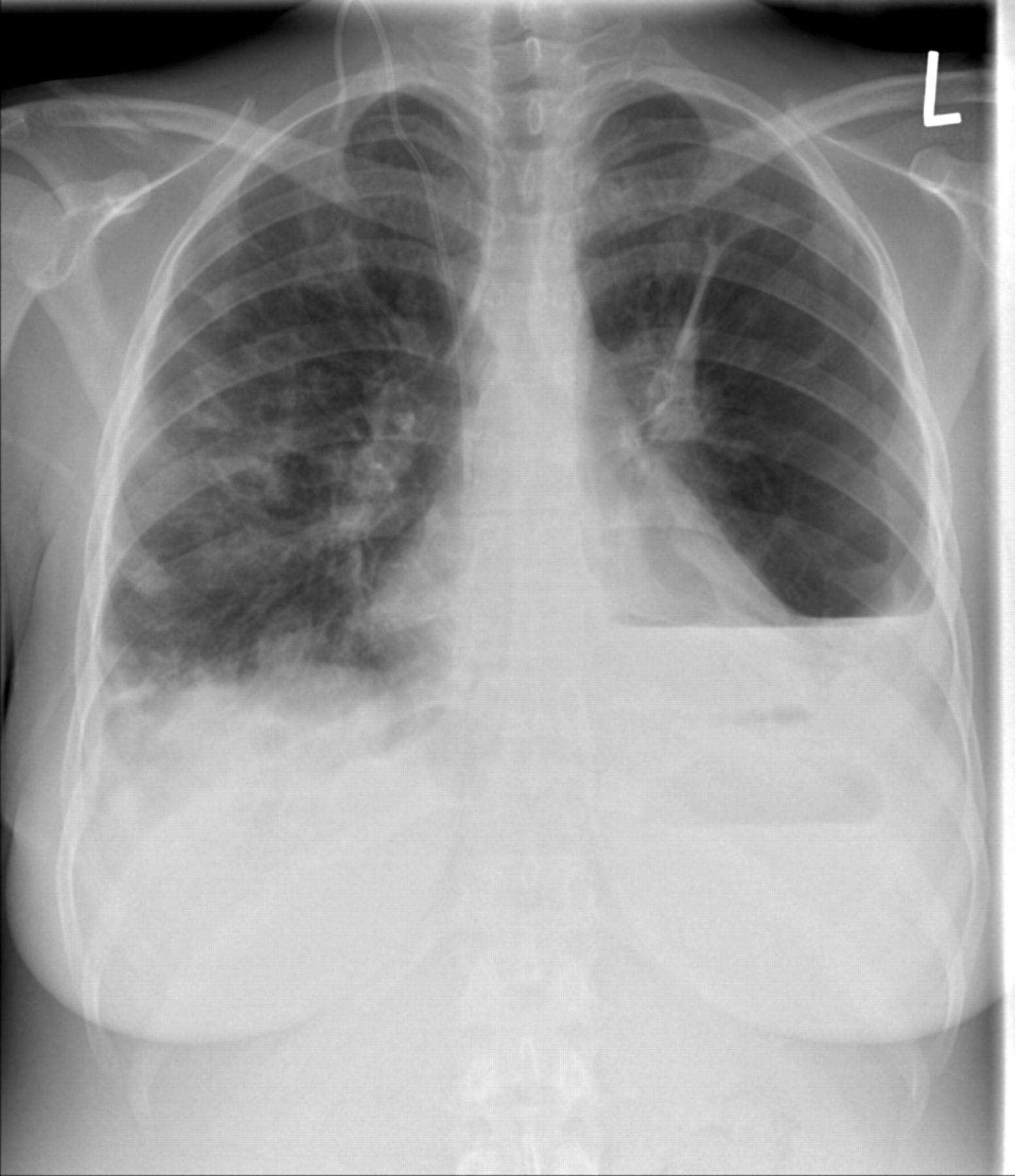
The presenting clinical features of right and left sided endocarditis are different. While most patients with right sided endocarditis will have systolic murmurs, the murmur is clearly pathologic in a minority of cases.6 Murmurs are, in fact, left sided and non-specific in most instances. The usual manifestations are persistent fever, bacteraemia, and multiple pulmonary emboli. Peripheral embolic manifestations are characteristically absent; rather, symptoms and complications arise from the involvement of the pulmonary vasculature by multiple septic pulmonary emboli. Hence chest pain, dyspnoea, cough, and haemoptysis may be presenting features. When peripheral embolic or neurologic features occur, either left sided endocarditis or paradoxical embolism should be considered. The conjunction of bacteraemia, fever, and multiple pulmonary infiltrates on chest radiography should always prompt a search for right sided endocarditis (fig 1).

Chest radiograph showing many of the features typical of right sided infective endocarditis complicated by septic pulmonary emboli. Multiple alveolar opacities are noted in the right lung. Abscess formation in the left lung has caused a broncho-pleural fistula, pneumothorax, and empyema, hence the air fluid level. The patient has had a central intravascular catheter placed for antibiotic administration.
Complications of right sided endocarditis may be thought of as either cardiac or pulmonary. A variety of complications attributed to septic pulmonary emboli have been described including pulmonary infarction, pulmonary abscesses, bilateral pneumothoraces, pleural effusions, and empyema. Mycotic aneurysms of the pulmonary arteries may be complicated by potentially fatal pulmonary hemorrhage. Multiple pulmonary emboli may result in right sided chamber dilatation, right heart failure, and a worsening of tricuspid regurgitation. The embolisation of vegetations large enough to result in obstruction of a significant portion of the pulmonary arterial circulation has been described but is unusual in our experience.
Cardiac complications may arise as a consequence of tricuspid valve destruction and severe tricuspid regurgitation with right sided volume overload, chamber dilatation, and right heart failure. Chronic right atrial dilatation may be a substrate for supraventricular arrhythmias, including atrial flutter and fibrillation. In our experience, paravalvar abscess formation occurs infrequently. Vasculitis may complicate right sided IE, but is not a typical feature. Hypoxaemia has been described in right sided IE when right atrial pressure is raised sufficiently to cause right to left shunting through a patent foramen ovale. Paradoxical embolism resulting from the transit of an embolus across an acquired pulmonary arteriovenous malformation has been reported. It should be recalled that a variety of coexistent medical problems such as hepatitis or HIV disease might be present in this population as a result of complications of injection drug use and poor self care.
DIAGNOSIS OF RIGHT SIDED ENDOCARDITIS
Duke criteria
The Duke system defines a major echocardiographic criterion for IE as the finding of an oscillating intracardiac mass on the valve or supporting structures, in the path of a regurgitant jet, a paravalvar abscess or new dehiscence of a prosthetic valve.10 Although the sensitivity and specificity of the Duke criteria have not been specifically studied in right sided endocarditis, the finding of any one of these echocardiographic features involving right heart structures, in the presence of positive blood cultures with a typical organism, should be regarded as diagnostic of right sided endocarditis. In our institution all injection drug users diagnosed with endocarditis had at least one major Duke criterion.8 It should be pointed out that injection drug use is a minor Duke criterion for the diagnosis of IE.
There are nonetheless some conceptual difficulties in uncritically applying the Duke criteria to right sided endocarditis. Right sided murmurs are more difficult to detect. This is especially true of many patients who are injection drug users with their first episode of endocarditis, who will have normal or only slightly elevated right ventricular pressures and in whom a lower velocity, less turbulent tricuspid regurgitant jet might be anticipated. One should not allow the lack of a murmur, therefore, to preclude further investigation if the clinical suspicion is high. Immunologic and vascular phenomena, which feature as minor criteria in the Duke system, are also less common. Septic pulmonary emboli are listed as a minor criterion in the Duke scheme; it could be argued that this important diagnostic feature is somewhat underweighted in the present Duke criteria. On balance, however, it seems reasonable to continue to use the Duke criteria as a useful diagnostic framework.
Chest x ray
The chest x ray is a helpful laboratory aid in diagnosing right sided endocarditis (fig 1), with 55% of radiographs at presentation showing evidence of pulmonary infiltrates compatible with pulmonary emboli.6 In our institution 56% of injection drug users with definite IE have multiple pulmonary opacities.8
Transthoracic echocardiography
Modern echocardiographic techniques have significantly improved our ability to diagnose right sided endocarditis and are now the cornerstone of the diagnosis in this disease. In febrile injection drug users, standard laboratory testing and physical examination without echocardiography were ineffective in detecting the patients with endocarditis.2
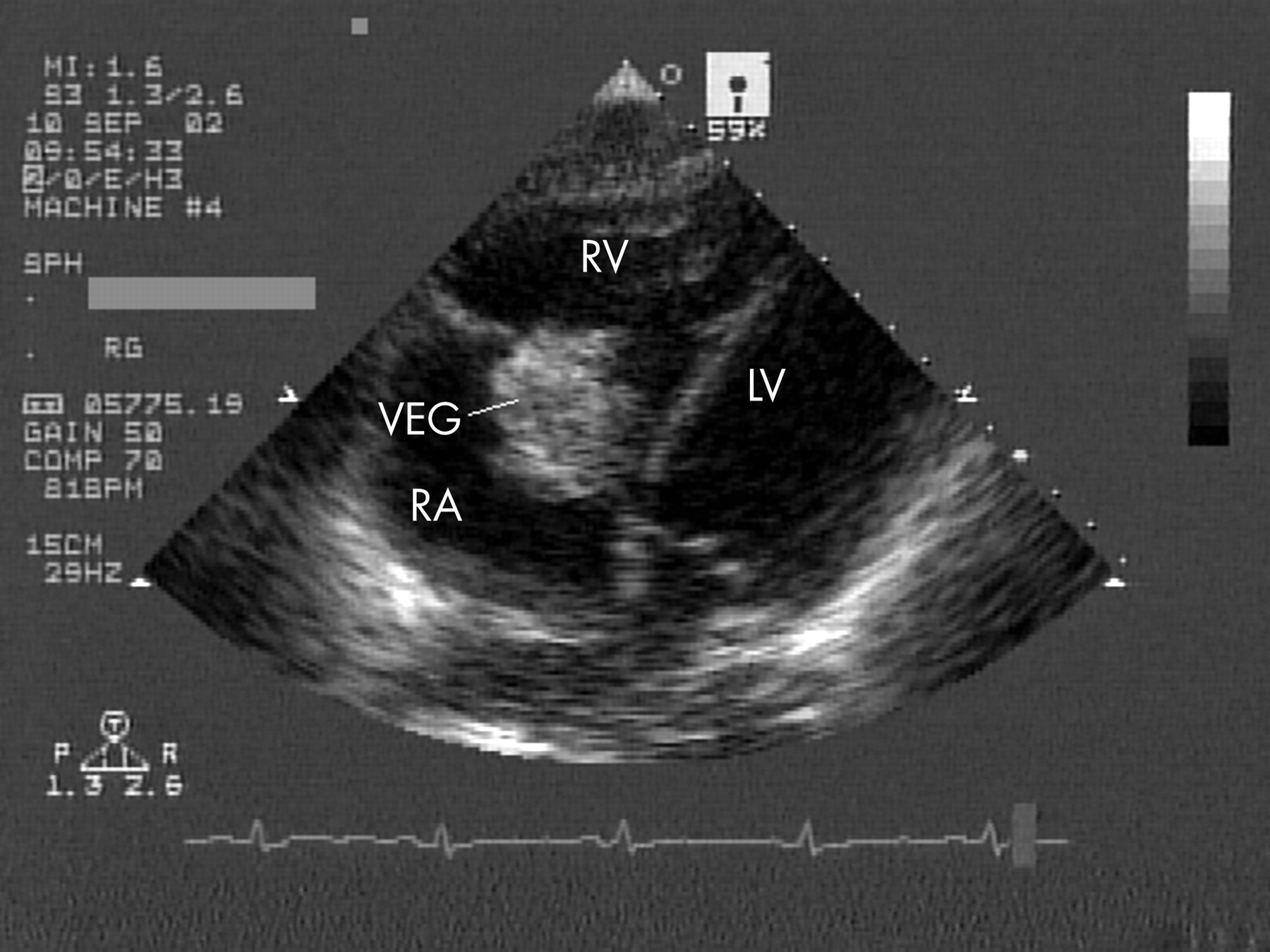
The key echocardiographic finding in right sided endocarditis is that of vegetation(s) in association with the tricuspid or rarely the pulmonary valve (fig 2). As with vegetations on the left sided valves, they tend to be localised to the atrial side of the valve in the path of the regurgitant jet. Tricuspid vegetations are often large and may be in excess of 2 cm, a finding that does not necessarily suggest the presence of fungal endocarditis. On rare occasions, vegetations may be sufficiently large so as to be confused with an intracardiac tumour. Entrapment of an embolised vegetation in the tricuspid chordal apparatus is sometimes seen. Similarly, embolised vegetations have been seen floating free in the right ventricle or pulmonary artery.
{kind=link}
{kind=link}
Large vegetation, approximately 4 cm in diameter, attached to the tricuspid valve. Off-axis echocardiographic views are sometimes useful in optimally demonstrating pathology in right sided infective endocarditis.
Occasionally the presence of normal anatomic variants such as Chiari network or prominent eustachian valve may cause diagnostic confusion, more particularly with transthoracic imaging; similarly venous catheters erroneously placed in the right atrium need to be identified and distinguished from vegetations. Right atrial thrombus may be distinguished from vegetation in that it is less likely to lie in the path of the jet and tends to layer on the right atrial wall. Past infection with damage to the tricuspid valve is commonly seen in this group, so the presence of vegetation does not in itself signify the presence of active infection. Extensive valve destruction with failure of leaflet co-optation and severe tricuspid regurgitation is a common sequel to tricuspid endocarditis. Although older or healed vegetations tend to be more echogenic and may even be calcified, this finding cannot reliably distinguish new from old infection. It should be clearly understood that echocardiographic findings need always to be taken in their clinical context. The finding of new or worsening tricuspid regurgitation, which is otherwise unexplained, should always prompt a diligent search for evidence of tricuspid endocarditis in the injection drug using patient.
Transoesophageal echocardiography
Many injection drug users have good thoracic ultrasound windows meaning that high resolution images can be obtained with transthoracic echocardiographic examination in many patients. This, combined with the relative proximity of the tricuspid valve to the ultrasound transducer, means that this valve is often well imaged by the transthoracic technique. We find the right ventricular inflow view and the subcostal views often give useful information when the question is one of tricuspid endocarditis. Careful attention to the adjustment of sector width, depth, and focus settings will help in accurate identification of vegetations. Under some circumstances higher frequency transducers—for example, 4 MHz or broadband transducers switched to a “resolution setting”—may be used to improve spatial resolution. Alternatively use of the “zoom function” (on some machines) may assist with lesion identification. The need for routine transoesophageal echocardiography (TOE) in right sided endocarditis is therefore questionable.11 TOE may be useful in detecting paravalvar abscess formation and for diagnosing unusual forms of right sided endocarditis such as pulmonary valve involvement or infection on the eustachian valve. For patients with suspected IE who are injection drug users, the practice in our laboratory is to perform transthoracic echocardiography (TTE) as the first echo study in almost all cases. The rationale for this approach is the simplicity and reduced cost of TTE and the importance of having the TTE information to direct and target a subsequent TOE examination appropriately. If there is a moderate or high suspicion of IE, and the initial TTE is negative, the TTE is repeated after an interval of about one week. TOE is then used in those patients in whom diagnostic quality images are not obtained with transthoracic imaging, and those who have negative TTE examinations where the suspicion of endocarditis is moderate or high (especially in the setting of staphylococcal bacteraemia). Occasionally pacing wires or right sided prosthetic valves are encountered; where there is a suspicion of endocarditis TOE is usually indicated. We often obtain our best views of the tricuspid valve via the transgastric window, while the pulmonary valve is usually best seen in the 60° mid oesophageal view. Rotation of the crystal array and angulation of the probe tip in order to visualise the valves in a number of orientations is mandatory during TOE.
HIV and right sided endocarditis
Significant immunosuppression (CD4 count < 200/mm3) is associated with a higher mortality rate in right sided IE in HIV infected injection drug users, though it is not clear that this increased mortality is as a consequence of the IE.12 As in non-HIV infected patients with right sided endocarditis, the involvement of the left sided valves is predictive of an increased risk of death.12
TREATMENT OF RIGHT SIDED ENDOCARDITIS
Short course antibiotic treatment for right sided endocarditis and management of addiction
The successful management of a complicated case often requires the close cooperation of a cardiologist, an infectious disease physician, and occasionally a cardiac surgeon. The role of addiction physicians in managing intercurrent drug withdrawal and maintaining the patient in hospital has been understated in the past. Methadone and/or other agents may be needed to control withdrawal symptoms. These patients may be difficult and disruptive and often engender negative attitudes in health care professionals. Their lack of adherence to in-hospital treatment is a major practical hurdle and has stimulated interest in developing shorter duration antibiotic regimens. There is reasonable evidence that short course antibiotic treatment for uncomplicated right sided endocarditis is effective.13 In our institution we use intravenous cloxacillin 2 g every four hours for two weeks together with gentamicin 1 mg/kg every eight hours for tricuspid endocarditis caused by methicillin sensitive staphylococcal species. The benefit of gentamicin in native valve endocarditis lies in earlier defervescence of fever and the sterilisation of blood cultures; there is no proven survival advantage. In the presence of a relative or absolute contraindication to gentamicin, therefore, a two week course of cloxacillin alone may be adequate. In the event that the patient cannot be persuaded to stay in hospital for the full two weeks, a 28 day course of oral treatment with ciprofloxacin and rifampin is prescribed, ideally with administration in a supervised setting such as a drug treatment facility.14 We consider intravenous drug use to be a contraindication for home treatment with intravenous antibiotics.
Circumstances where short course antibiotic treatment for infective endocarditis is not appropriate
-
▸ Confirmed or suspected left sided endocarditis
-
▸ Metastatic sites of infection or empyema
-
▸ Cardiac or extracardiac complications
-
▸ Methicillin resistant Staphylococcus aureus (MRSA)
-
▸ Presence of any prosthetic valve
-
▸ Vegetation size > 10 mm
-
▸ Incomplete response to treatment
-
▸ HIV positive and CD4 count < 200/mm3
There are some situations in which short course antibiotic treatment is not appropriate (see box).
In general non-staphylococcal right sided endocarditis is treated in a similar fashion to left sided endocarditis. A full discussion of antibiotic regimens to cover all contingencies is beyond the scope of this review.
Prognosis and surgical treatment of right sided endocarditis
Right sided endocarditis is generally regarded as having a relatively benign prognosis and in-hospital mortality is less than 10%. Our in-hospital mortality for right sided IE in injection drug users is 5%. Most will survive even if they leave hospital before the full course of treatment has been completed. As follow up in the injection drug using population is notoriously difficult, few data are available on their long term outlook. It is clear that there will be a significant late mortality from causes other than IE and right heart failure, such as non-cardiac infections, drug overdose, and AIDS related complications. Mortality is higher where there is left sided involvement.
Fortunately most patients can be treated medically, with surgery being necessary in only a small minority of cases.6 Indications for surgical treatment are better defined for left than for right sided endocarditis. Sepsis, which is uncontrolled despite adequate antibiotic treatment, and intractable right heart failure despite appropriate medical treatment, are the most important indications for surgical intervention. The finding of a paravalvar abscess or fungal endocarditis are usually indications for surgery. Recurrent pulmonary embolism following the initiation of antibiotic treatment may occur and does not in itself represent an indication for surgery.6 Some authors have felt that large vegetation size (diameter > 10 mm) in the context of persisting fever identifies a set of patients who are likely to benefit from surgery.15 Others have felt that many of these patients will eventually recover with medical treatment.16 Very large vegetations (> 20 mm), however, are associated with a poor outcome.6 Patients may also require an operation to treat concomitant left sided endocarditis.
Injection drug use and right sided endocarditis: key points
-
▸ In inner city communities most cases of infective endocarditis (IE) occur in injection drug users; many of these will have right sided IE caused by staphylococci
-
▸ If injection drug users with bacteraemia from an inner city demographic are considered, up to 41% will have evidence of endocarditis
-
▸ The conjunction of bacteraemia, fever, and multiple pulmonary infiltrates on chest radiography should always prompt a search for right sided IE
-
▸ A transoesophageal echocardiographic examination is not necessary in many cases of right sided IE
-
▸ Coexistent medical problems such as hepatitis or HIV disease may be present
-
▸ Successful treatment of right sided IE in injection drug users requires a multidisciplinary approach
-
▸ Most patients will recover with medical treatment; short course or rarely oral antibiotic treatment may be useful in certain situations
Enthusiasm for surgery is tempered by the knowledge that the majority of patients will resume injection drug use following hospital discharge. Surgical approaches vary, with valve removal or replacement being the historical, commonly recommended approaches. Both approaches are controversial and there is a lack of controlled trials in the literature upon which to base decision making. Valvectomy may result in permanent damage to the right ventricle and ultimately intractable right heart failure and death. Significant early mortality (11%) was reported in one group where this approach was used.17 We have seen large pericardial effusions and tamponade following valvectomy caused by refractory right heart failure. More recent attention has focused on tricuspid valve vegetectomy or repair.18 Repair has the advantage of avoiding or minimising the implantation of foreign material in the infected area while preserving the function of the valve. Several different techniques have been used, including cusp resection (rendering the valve bicuspid), commissural plication, the use of artificial chordae, and pericardial patch repair of the tricuspid leaflet (sometimes in conjunction with mobilisation of the secondary chordae and tricuspid annuloplasty). Where extensive valvar destruction has occurred, replacement of the tricuspid valve may be necessary. When valve replacement is unavoidable our current approach is to use cryopreserved mitral homografts in the tricuspid position, which usually requires the addition of a tricuspid ring to provide annular stability.19 Reinfection of the valve can be anticipated in some cases; when this occurs, antibiotic treatment may result in a cure of the prosthetic valve endocarditis.20
PREVENTION
A discussion of the issues involved in the prevention of injection drug use is beyond the scope of this review. It is possible that harm reduction strategies aimed at reducing injection frequency (such as methadone availability) or clean injection strategies (clean injection education, injection rooms, needle exchange programmes or legal heroin) may have a beneficial effect.
REFERENCES
Supplementary materials
. Web-only References
Available as PDF (printer friendly file)Files in this Data Supplement:
Linked Articles
- Miscellanea