Article Text

Statistics from Altmetric.com
Drug eluting stents (DES) permit controlled release of antiproliferative agents from durable polymer coatings and are recognised as a major innovation in the treatment of coronary artery disease.1 DES use has significantly improved clinical outcomes as compared with bare metal stents (BMS), primarily through a notable reduction in the risk of repeat revascularisation. However, the potent anti-restenotic effect of early generation DES—namely Cypher sirolimus eluting stents (SES) and Taxus paclitaxel eluting stents (PES)—came at the expense of delayed arterial healing of the stented coronary segment, characterised by chronic inflammation at the stented site with uncovered stent struts, coronary evaginations and positive vessel remodelling, fibrin deposition, and neoatherosclerosis.2 ,3 This pathological process has been proposed as a mechanism of the higher risk of late thrombotic events—specifically very late stent thrombosis—after implantation of early generation Cypher SES and Taxus PES.2
The introduction of newer generation DES with thinner stent struts, novel durable or biodegradable polymer coatings, and new limus antiproliferative agents, has improved upon the safety profile of early generation DES by significantly reducing the risk of stent thrombosis during the long term.4 ,5 It is noteworthy that this has not compromised their effectiveness, which has been further improved by the use of newer generation DES, with a significant reduction in the risk of target lesion revascularisation (TLR) compared with the early generation DES.5 ,6 Accordingly, newer generation DES—including durable polymer based Xience (Abbot Vascular, California, USA) and Promus (Boston Scientific, California, USA) everolimus eluting stents (EES), Resolute zotarolimus eluting stents (ZES) (Medtronic, California, USA), as well as biodegradable polymer based Biomatrix (Biosensors, Switzerland) and Nobori (Terumo, Japan) biolimus eluting stents, and Yukon Choice PC SES (Translumina, Germany)—have become the standard of care in all patient and lesion subsets with excellent long term results.1
Stent technology continues to evolve and novel DES with biodegradable polymer coatings, polymer-free DES, self-expanding and mesh covered stents, as well as fully biodegradable coronary scaffolds, have been developed and are currently under clinical investigation (figure 1). These technologies aim to improve arterial healing further, avoiding long term complications and potentially reducing dual antiplatelet therapy duration. This article provides an overview of these novel stent platforms based on data published or presented at major conferences.

Schematic representation of coronary stent technologies. From left to right: drug eluting stents (DES) with durable polymer coatings, DES with biodegradable polymer coatings, polymer-free DES, and fully bioresorbable coronary scaffolds. The top panels summarise the features of the coronary cross sections and stent cross sections at the time of implantation, whereas the bottom panels show the same features after the completion of drug release. In the coronary cross sections, the vessel lumen is displayed in red, the intima in yellow, and the stent struts in grey.
DES with biodegradable polymer coatings
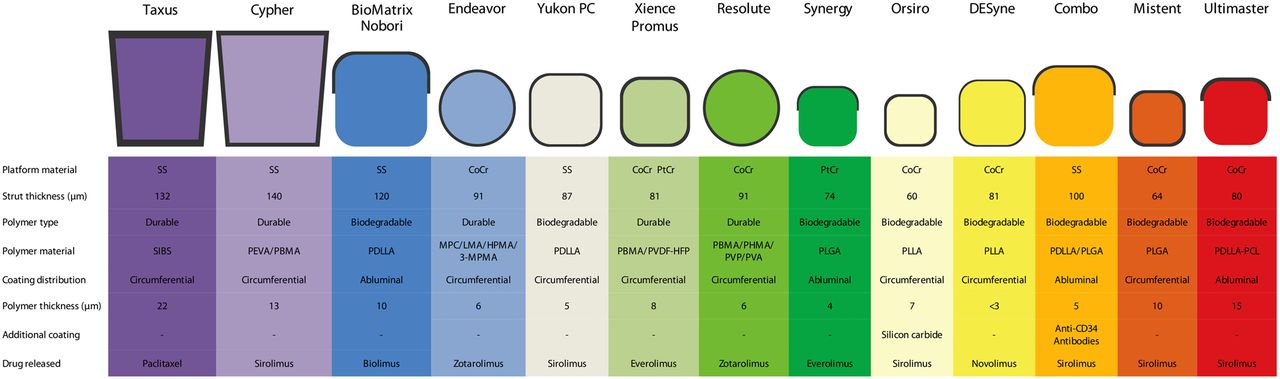
Durable polymer coatings permanently reside on the stent surface beyond the time period of drug release, and have been identified as a possible trigger of delayed arterial healing. DES with biodegradable polymer coatings—which degrade after completion of drug release—have been developed to overcome this limitation. Most biodegradable polymer coatings consist of polylactic acid (PLA) isoforms or polyglycolic acid which fully degrade over a variable period of time (table 1). Experience with the first DES with biodegradable polymer coatings—Biomatrix, Nobori, and Yukon Choice PC—have shown a reduced risk of stent thrombosis, very late stent thrombosis, and TLR compared with early generation DES with durable polymer coating during long term follow-up in large scale clinical trials.5 ,7 Moreover, two recent studies have shown comparable outcomes with biodegradable polymer based Nobori biolimus eluting stents compared with newer generation durable polymer EES.8 ,9 An overview of early and newer generation DES based on durable or biodegradable polymer coatings is presented in figure 2. Several new DES based on biodegradable polymer coating are currently under investigation (table 2).
Biodegradable polymers used for coronary devices
Summary of novel DES with biodegradable polymer coatings

{kind=link}
{kind=link}
Drug eluting stents with durable or biodegradable polymer coatings. SS, stainless steel; CoCr, cobalt chromium; PtCr, platinum chromium; SIBS, poly(styrene-b-isobutylene-b-styrene); PEVA, poly-ethylene-co-vinyl acetate; PBMA, poly n-butyl methacrylate; PVDF-HFP, co-polymer of vinylidene fluoride and hexafluoropropylene; MPC, methacryloyloxyethyl phosphorylcholine; LMA, lauryl methacrylate; HPMA, hydroxypropyl methacrylate; 3-MPMA, trimethoxysilylpropyl methacrylate; PVP, polyvinyl pyrrolidinone; PHMA, polyhexyl methacrylate; PVA, polyvinyl acetate; PLGA, poly-lactic co-glycolic acid; PLLA, poly-L-lactic acid; PDLLA, poly-D, L-lactic acid.
Synergy EES with biodegradable polymer
The Synergy stent (Boston Scientific, Massachusetts, USA) is based on a 74 µm thick platinum chromium stent platform which releases everolimus from an ultrathin abluminal biodegradable poly-lactic co-glycolic acid (PLGA) polymer coating of 4 µm thickness, which is resorbed during a period of 3–4 months. The Synergy stent was directly compared with the Promus Element EES in the randomised EVOLVE I non-inferiority trial investigating two different doses of everolimus (full dose 113 µg/20 mm and half dose 56 µg/20 mm stent surface).10 Overall, 291 patients were randomised 1:1:1 to receive Synergy full dose, Synergy half dose, or Promus Element stents. At 6 months, both Synergy stent platforms were shown to be non-inferior to the Promus Element stent with respect to the primary end point of in-stent late lumen loss (LLL) (full dose 0.10±0.25 mm vs half dose 0.13±0.26 mm vs Promus 0.15±0.34 mm, p non-inferiority <0.001 for both comparisons). Clinical outcomes were comparable between the three groups at up to 2 years follow-up.w1 In the meantime, the Synergy full dose platform has gained CE approval and is currently being assessed in the larger scale EVOLVE-II trial—powered for clinical end points—compared with Promus Element stents.
Orsiro SES with biodegradable polymer
The Orsiro stent (Biotronik, Germany) consists of a 60 µm thick cobalt chromium platform which releases sirolimus from biodegradable poly-L-lactic acid (PLLA) polymer coating which is resorbed during a period of <2 years. The metal platform is also coated with a layer of silicon carbide which aims to reduce corrosion related to the interaction of the metallic surface with blood flow. The BioFLOW-II trial randomly assigned 452 patients in a 2:1 ratio to the Orsiro or the Xience EES, and established non-inferiority of the former for in-stent LLL at 9 months (0.10±0.32 mm vs 0.11±0.29 mm, p non-inferiority <0.0001).w2 In-segment binary restenosis was also comparable between Orsiro and Xience Prime (4.0% vs 4.7%, p=0.72) as were clinical outcomes, with no stent thrombosis observed at 9 months follow-up. Several ongoing trials powered for clinical end points are comparing the Orsiro stent with other newer generation DES.
DESyne novolimus eluting stent with biodegradable polymer
The DESyne BD (Elixir, California, USA) stent consists of an 81 µm thick cobalt chromium stent platform with a biodegradable poly-D-L-lactic acid (PDLLA) coating which is degraded during a period of 6–9 months and releases novolimus—a sirolimus derivative. The DESyne BD novolimus eluting stent was shown to be non-inferior to Endeavour ZES for in-stent LLL at 6 months in the EXCELLA-BD trial (0.12±0.15 mm vs 0.67±0.47 mm, p non-inferiority <0.001), in which 146 patients were randomly assigned in a 3:1 ratio to DESyne BD or Endeavour ZES.w3 In addition, angiographic binary restenosis was significantly lower with DESyne as compared to Endeavour ZES (0.0% vs 7.9%, p=0.003), while clinical events were comparable up to 2 years follow-up.w4
Combo SES with biodegradable polymer and anti-CD 34 antibody coating
The Combo stent (OrbusNeich, Florida, USA) is based on a 100 µm thick stainless steel platform coated abluminally with a biodegradable polymer matrix (PDLLA and PLGA) releasing sirolimus. In addition, the stent has a circumferential layer of anti-CD34 antibodies aiming to promote re-endothelialisation. Findings from an animal study, evaluating histology and optical coherence tomography (OCT) at 28 days in a porcine model, suggest that the combination of biodegradable polymer with coatings of anti-CD34 antibodies enhances endothelialisation and reduces neointimal hyperplasia as well as inflammation compared with standard SES and a stent coated with anti-CD34 antibodies only.w5 In the REMEDEE trial, 183 patients were randomly assigned in a 2:1 ratio to receive the Combo stent or the Taxus PES. At 9 months, the Combo stent was found to be non-inferior to the Taxus PES for the primary angiographic end point of in-stent LLL (0.39±0.45 mm vs 0.44±0.56 mm, p non-inferiority =0.0012).11 Clinical event rates were low and comparable in both groups.
MiStent SES with biodegradable polymer
The MiStent (Micell Technologies, North Carolina, USA) is a 64 µm thick cobalt chromium stent coated with a biodegradable PLGA polymer which degrades during a period of approximately 2 months and elutes sirolimus.w6 In the DESSOLVE-I first-in-man study the MiStent was implanted in 30 patients and showed an in-stent LLL—the primary end point—of 0.09±0.10 mm at 8 months angiographic follow-up. Intravascular ultrasound (IVUS) showed a neointimal obstruction of 10.9% and OCT showed a mean strut coverage of 96.5%. No binary restenosis or TLR was observed up to 12 months.w7 In the DESSOLVE-II trial, 184 patients were randomised 2:1 to MiStent or Endeavour ZES. At 9 months, MiStent was superior to Endeavour ZES in terms of in-stent LLL (0.27±0.46 vs 0.58±0.41, p<0.001).w8 Clinical outcomes were similar with the two stents through the 9 months. A large scale, all-comers clinical trial will directly compare the MiStent with the Xience EES.
Ultimaster SES with biodegradable polymer
The Ultimaster (Terumo, Japan) consists of a 80 µm thick cobalt chromium stent coated abluminally with a PDLLA and polycaprolactone copolymer which is resorbed within 3–4 months and releases sirolimus. The Ultimaster stent was implanted in 105 patients in the CENTURY study and showed an in-stent LLL of 0.04±0.35 mm at 6 months angiographic follow-up. Stent strut coverage assessed by OCT was 96.2±5.4% at 6 months. Clinical event rates were low at 12 months follow-up.w9 The CENTURY-II trial comparing Ultimaster with the Xience EES is ongoing.
Polymer-free DES
Polymer-free DES are based on different technologies for drug binding and release without the use of polymer coatings. Antiproliferative agents can be applied to the surface by covalent bonding or chemical precipitation. Alternatively, they can be dissolved in non-polymeric biodegradable substances directly applied to a porous surface or within the stent's body. Several polymer-free DES have been investigated in clinical studies and are listed in table 3.
Summary of polymer-free DES
Yukon choice polymer-free SES
The Yukon Choice PF (Translumina, Germany) stent consists of an 87 µm thick stainless steel platform with a sand blasted microporous surface, with 2 µm deep micropores serving as the drug reservoir.w10 An interesting feature of the Yukon Choice PF is that it allows loading of different antiproliferative agents with different concentrations in the catheterisation laboratory, by a coating process taking 3–8 min depending on stent length. The device has been tested with a dual coating of sirolimus and probucol—referred to as Dual DES—dissolved in a 1:1 ratio, combined with a shellac resin used to improve adherence of the agents to the stent and to enhance structural integrity of the coating.
The Yukon has been directly compared with Cypher SES and Endeavour ZES in the randomised ISAR-TEST 2 trial (N=1007, 1:1:1 stent allocation), showing the superiority of Yukon compared with Endeavour ZES (11.0% vs 19.3%, p=0.002) and similar outcomes between Yukon and Cypher SES (11.0% vs 12.0%, p=0.68) in terms of binary restenosis at 6–8 months. Angiographic surveillance at 2 years showed binary restenosis in 13.9% of Yukon, 18.6% of Cypher SES, and 20.9% of Endeavour ZES treated lesions (p=0.047).w11 Of note, binary restenosis between 6–8 months and 2 years was lower with Yukon compared with Cypher SES (p=0.023).
In the ISAR-TEST 3 trial, the Yukon stent was compared with a similar stent with a biodegradable polymer coating (Yukon Choice PC) and with Cypher SES in 605 patients. At 6–8 months angiographic follow-up, the Yukon Choice PF stent did not meet the prespecified criteria for non-inferiority compared with Cypher SES in terms of in-stent LLL (0.47±0.56 mm vs 0.23±0.46 mm, p non-inferiority =0.94). Notwithstanding, at 2 years of follow-up delayed LLL was lower among patients treated with the Yukon Choice PF stent compared with the Cypher SES and the Yukon with biodegradable polymer coating (−0.01±0.36 mm vs 0.16±0.41 mm vs 0.17±0.42 mm).12 These results suggest that polymer-free Yukon Choice PF may provide a therapeutic option to overcome late progression of neointimal hyperplasia observed with several durable polymer DES.2 Recently, a cobalt chromium version of the Yukon Choice PF with thinner struts (68 µm) has been developed.
BioFreedom polymer-free biolimus eluting stent
The BioFreedom polymer-free biolimus eluting stent (Biosensors, Switzerland) is made of stainless steel with a strut thickness of 112 µm and a micro-structured, polymer-free surface alteration at the abluminal stent side. In the BIOFREEDOM first-in-man study, 182 patients were randomised 1:1:1 to the BioFreedom stent with two different biolimus doses (15.6 and 7.8 µg/mm) or to the Taxus PES.w12 The primary angiographic end point of in-stent LLL was evaluated at 4 and 12 months in two different cohorts. BioFreedom with both standard dose and low dose were superior compared with Taxus PES at 4 months (0.08 (0.02–0.14) mm vs 0.12 (0.07–0.25) mm vs 0.37 (0.14–0.50) mm, p<0.001 for both comparisons). At 12 months, BioFreedom standard dose was non-inferior to Taxus PES (0.17 (0.09–0.39) mm vs 0.35 (0.22–0.57) mm, p non-inferiority =0.001, p superiority =0.11), whereas BioFreedom low dose did not meet the non-inferiority margin compared with Taxus PES (0.22 (0.17–0.66) mm vs 0.35 (0.22–0.57) mm, p non-inferiority =0.21, p superiority =0.55). Similar clinical outcomes were observed with the BioFreedom and Taxus stents up to 3 years of follow-up.w13 The LEADERS FREE trial currently compares BioFreedom with BMS among 2456 patients at high risk of bleeding requiring a short duration of dual antiplatelet therapy of only 1 month.w14
Cre8 polymer-free SES
The Cre8 stent (CID, Italy) is based on an 80 µm thick cobalt chromium platform with abluminal reservoirs. Cre8 releases sirolimus formulated with an organic acid—namely amphilimus—that enhances drug stability, facilitates sustained drug elution, and modulates drug bioavailability. The platform also has a passive carbon coating. A preclinical study in a porcine model indicated that the carbon coating is associated with reduced neointimal thickness and inflammatory scores compared with the same stent platform without carbon coating as well as the Cypher SES.w15 In the NEXT trial, 323 patients were randomised to Cre8 or Taxus PES. At 6 months, Cre8 was not only non-inferior but also superior to Taxus PES in terms of in-stent LLL (0.14±0.36 mm vs 0.34±0.40 mm, p non-inferiority <0.0001, p superiority <0.0001).13 A post-hoc analysis of 82 diabetic patients showed a lower LLL with Cre8 compared with Taxus PES (0.12±0.28 mm vs 0.43±0.41 mm, p<0.0001). Overall rates of clinical end points were low and comparable between the two groups at 12 months follow-up. In the recent Demonstr8 trial (N=38), Cre8 was found to be non-inferior compared with a cobalt chromium BMS in terms of strut coverage assessed by OCT at 30 days. Ongoing clinical trials are evaluating the safety of Cre8 in patients taking dual antiplatelet therapy for shorter duration (Assur8 trial) and the efficacy of Cre8 in diabetic patients (Particip8 and RESERVOIR trials).
VESTAsync hydroxyapatite coated SES
VESTAsync (MIV Therapeutics, Georgia, USA) consists of a cobalt–chromium platform with a nanothin microporous hydroxyapatite surface coating impregnated with a low dose lipid–sirolimus mixture (55 µg). While sirolimus is released over 90 days, the hydroxyapatite coating dissolves over 9–12 months after stent implantation. An animal study indicated that the low dose of sirolimus released—which is made possible by the hydroxyapatite coating—results in improved arterial healing compared with Cypher SES.w16 In the VestaSync-I first-in-man trial, the VESTAsync stent was implanted in 15 patients with an LLL of 0.36±0.23 mm assessed by quantitative coronary angiography (QCA) and percentage neointima obstruction assessed by IVUS of 6.1±4.2% at 9 months.14 In the Vesta-Sync-II trial 75 patients were randomised 2:1 to VESTAsync or an equivalent BMS, and showed superiority of the former device in terms of in-stent LLL at 6 months angiographic surveillance (0.39±0.20 mm and 0.74±0.52 mm, p=0.03).w17
Amazonia Pax polymer-free PES
The Amazonia Pax (Minvasys, France) stent is based on a 73 µm thick cobalt chromium platform and releases paclitaxel. The latter is applied on the abluminal surface only, by a microdrop spray crystallisation process, ensuring 98% paclitaxel release within 30 days and complete uncoating within 45 days. The Amazonia Pax stent was evaluated in two angiographic trials: PAX A and PAX B. In the PAX A study, 31 patients were randomised 1:1 to Amazonia Pax or Taxus PES.w18 At 4 months, in-stent LLL and IVUS percentage neointimal obstruction for the Amazonia Pax and Taxus PES were 0.77 mm vs 0.42 mm (p=0.20) and 19.2% vs 9.3% (p=0.08), respectively. OCT evaluation indicated a higher rate of covered struts with Amazonia Pax compared with Taxus PES (99.6% vs 91.7%, p<0.01). Clinical events rates were low and comparable through 2 years. In PAX B—a prospective multicentre registry—103 patients were treated with Amazonia Pax. At 9 months angiographic surveillance, the primary end point of binary restenosis was observed in 19.7% of patients. At 2 years follow-up, myocardial infarction (MI) had occurred in 5.8% of patients and TLR in 25.2% of patients, and no stent thrombosis was observed.
Fully bioresorbable coronary scaffolds
Fully bioresorbable coronary scaffolds are made of polymeric materials which provide transient vessel support and site specific drug delivery followed by complete resorption during a time period of several months to years.15 These devices promise benefit beyond current metallic stent platforms by avoiding permanent caging of the stented segment, with the potential to improve long term vessel patency, vasomotion, adaptive shear stress, sealing of plaques, and access to side branches. Available evidence suggests that as the treated vessel is uncaged over time, restoration of physiologic vasomotion and arterial healing—with formation of a neocap which seals the treated atherosclerotic plaque—are observed.w19 Moreover, vessel remodelling with lumen enlargement and plaque reduction have been observed after implantation of bioresorbable scaffolds in animal models and humans.16 Several bioresorbable coronary scaffolds are undergoing clinical investigation (table 4).
Summary of bioresorbable coronary scaffolds
Bioresorbable everolimus eluting vascular scaffold
The everolimus eluting bioresorbable vascular scaffold (BVS, Abbot Vascular, California, USA) is the most widely investigated scaffold to date, and has received the CE mark for coronary use. BVS is based on a PLLA backbone coated with a 1:1 mixture of PDLLA matrix allowing release of everolimus. The first available BVS (V.1.0) consisted of out-of-phase sinusoidal hoops with straight and direct links between struts, which had a thickness of 150 μm. In the first-in-man ABSORB Cohort A study, this device was implanted in 30 patients with de novo lesions.15 At 6 months, angiographic surveillance showed an LLL of 0.43±0.37 mm, which was lower than the figures obtained with BMS but higher than that observed with newer generation metallic DES. Of note, LLL with BVS V.1.0 was related to a combination of neointimal hyperplasia and a reduction in scaffold area directly related to scaffold shrinkage and non-uniform vessel support. The study included intracoronary imaging evaluation with IVUS, OCT, and palpography at 6 months and 2 years follow-up. Effective bioresorption was supported by the following intracoronary imaging findings: (1) a 35% reduction in the number of struts assessed by OCT at 2 years; (2) a notable reduction in IVUS hyperechogenicity of individual struts; (3) a change in plaque composition visualised by virtual histology; (4) an increase in strain pattern on palpography; and (5) a recovery of vasomotion of the treated segment after administration of ergometrine or acetylcholine. Clinical follow-up showed no adverse events except for one non-Q wave MI observed in up to 5 years.
BVS V.1.1 is based on the same polymer but features a new design with in-phase hoops and direct links allowing more consistent drug application and more uniform vessel wall scaffolding. Structural changes were implemented in order to address late scaffold shrinkage. In the ABSORB Cohort B study, 101 patients with stable coronary artery disease were treated with BVS V.1.1.w20 Angiographic surveillance showed 0.19±18 mm LLL at 6 months, 0.27±32 mm at 1 year, and 0.27±19 mm at 2 years.16 It is noteworthy that late strut shrinkage, as observed with BVS V.1.0, was nearly eliminated. Assessment of vasomotion after ergometrine and acetylcholine intracoronary administration suggested a recovery of vasoreactivity already at 1 year follow-up with further improvement at 2 years. At 2 years clinical follow-up, adverse cardiac events had occurred in 8.9% of patients: 3.0% had a non-Q wave MI and 5.9% had a TLR. No case of stent thrombosis was observed. The BVS V.1.1 is currently being investigated in several clinical trials among stable patients as well as patients with acute MI.
DESolve novolimus eluting bioresorbable vascular scaffold
The DESolve scaffold (Elixir Medical, California, USA) is made of PLLA with a strut thickness of 150 μm, releases novolimus, and resorbs over a period of 1–2 years. A myolimus eluting version of the device was initially tested in a first-in-man study (N=16) showing an LLL at 6 months of 0.19±0.19 mm. In the recently presented DESolve Nx trial 126 patients were treated with the DESolve scaffold. In-stent LLL was 0.21±0.34 mm and 3.5% of patients had binary restenosis at 6 months angiographic follow-up. Intracoronary imaging with IVUS and OCT was performed at 6 months follow-up, showing a low percentage volume obstruction (5.1±4.2%) by IVUS as well as low neointimal thickness (0.10±0.03 mm) and a high percentage of covered struts (98.8%) by OCT. Adverse clinical events were few, with one cardiac death, one non-Q wave MI, and one TLR in 6 months.w21 Based on these data the DESolve scaffold recently received the CE mark for coronary use.
REVA and ReZolve sirolimus eluting polycarbonate scaffold
The REVA (REVA Medical Inc, San Diego, California, USA) is a poly (iodinated desaminotyrosyl-tyrosine ethyl ester) carbonate scaffold, which degrades into carbon dioxide, water, and ethanol, leaving iodinated desaminotyrosyl-tyrosine that is then absorbed and excreted. The REVA scaffold is not coated with any antiproliferative drug and biodegrades over a 36 month period. The device is characterised by a slide and locking design that provides flexibility and strength, preventing deformation and weakening during deployment. After promising results in preclinical studies, REVA was tested in 27 patients with de novo lesions in the RESORB first-in-man trial. However, polymer embrittlement led to local mechanical failure with a high rate of repeat revascularisation procedures (67%) at 6 months follow-up. The device was redesigned under the name of ReZolve with a more robust polymer and a sirolimus coating. ReZolve is currently being investigated in 22 patients enrolled in the RESTORE trial, with primary angiographic evaluation at 12 months. Interim results were recently presented and showed a preliminary in-stent LLL of 0.20±0.19 mm in the first eight patients undergoing angiographic surveillance.w22 Moreover, the RESTORE-II single arm, prospective, multicentre trial (N=125) is ongoing and will provide data for CE mark application.
IDEAL poly-anhydride ester salicylic acid sirolimus eluting scaffold
The IDEAL scaffold (Xenogenics, Massachusetts, USA) is made of a backbone of poly-anhydride ester together with salicylic acid, with a strut thickness of 200 μm and an 8.3 μg/mm sirolimus coating. This drug mixture provides antiproliferative and anti-inflammatory action. Sirolimus is released over 30 days and complete scaffold bioresorption occurs within 12 months. During bioresorption, salicylic acid is absorbed into the vessel wall with the aim of inhibiting an inflammatory response. In the first-in-man WHISPER study the IDEAL scaffold was implanted in 11 patients. At 12 months follow-up there was no evidence of acute or chronic recoil, supporting radial strength of the scaffold.w23 However, excessive neointimal growth was observed, probably due to the rapid elution of sirolimus coupled with an inadequate initial drug dosage. A revised version has been developed, with a higher drug dose and a slower drug release. In addition, the scaffold design has been optimised with thinner struts and reduced crossing profile. The iterated scaffold is currently under investigation.
ART 18Z bioresorbable scaffold
The ART 18Z (Arterial Remodeling Technology, France) is a PDLLA scaffold with a strut thickness of 170 μm and no drug release. This scaffold is currently under investigation in the ARTDIVA first-in-man, multicentre, single group, prospective trial (N=30).
Other PLA based scaffolds
A few other bioresorbable coronary scaffolds have been developed (eg, Xinsorb BRS, Huaan Biotechnology, China; Amaranth BRS, Amaranth Medical, California, USA); however, these devices have not progressed beyond preclinical evaluation at this point in time.
Absorbable metallic scaffold
The AMS-1 scaffold (Biotronik, Germany) is made of an alloy of magnesium (93%) and rare metals (7%), with a strut thickness of 165 μm. Preclinical studies showed a rapid endothelialisation of the scaffold, with magnesium degrading into inorganic salts within 60 days without any significant inflammatory response. The AMS-1 scaffold was evaluated in 63 patients with single de novo lesions in the PROGRESS-AMS trial.17 Patients treated with AMS-1 showed recovery of vasomotion within the stented segment. However, rates of TLR were 39.7% at 4 months follow-up and 45.0% at 1 year. Moreover, IVUS findings suggested that the 1.08 mm in-stent LLL at 4 months was mainly related to a lower radial force of AMS-1 compared with BMS during the early phase, possibly due to the rapid resorption of the scaffold. The revised AMS-2 was therefore developed with a different magnesium alloy with a higher collapse pressure and a slower resorption. In addition, AMS-2 features a reduced strut thickness (120–130 μm) and a change in the cross-sectional shape, with square instead of rectangular struts to improve radial strength.
Drug eluting absorbable metallic scaffold
The AMS-2 scaffold employed drug release in the DREAMS stent (Drug-Eluting AMS, Biotronik, Germany) by coating the platform with biodegradable PLGA for release of paclitaxel. Controlled release of paclitaxel occurs during the first 90 days, with subsequent biodegradation of the PLGA coating. In the BIOSOLVE-1 first-in-man, prospective, multicentre trial, the DREAMS scaffold was implanted in 46 patients.18 At angiographic surveillance at 12 months, the in-scaffold LLL was 0.52±0.39 mm and the in-scaffold percentage volume obstruction assessed by IVUS was 6.24±5.00%. In terms of clinical events, three (7%) of the patients had target lesion failure at 12 months. Two of these were clinically driven TLR, whereas the third patient suffered a periprocedural MI at the time of the 12 month angiography. The scaffold will undergo a further modification to release sirolimus instead of paclitaxel.
Other novel coronary stents
Stentys self-apposing stent
Vessel size among ST segment elevation MI (STEMI) patients undergoing primary percutaneous coronary intervention (PCI) is often underestimated due to vasoconstriction and thrombus between the stent surface and arterial wall. Balloon expandable stents used in this setting have been associated with acute stent malapposition, a risk factor for stent thrombosis in 20–30% of cases as assessed by intracoronary imaging.w24 Moreover, high pressure balloon expansion and use of oversized stents may provoke distal embolisation of plaque and thrombus material, which impairs myocardial perfusion and increases infarct size and mortality. Self-expanding stents used in the setting of STEMI aim to overcome both limitations—impaired myocardial perfusion and stent malapposition—by allowing for less traumatic, acute stent implantation coupled with the ability of the stent to grow in volume during the first days after the procedure, thus minimising stent malapposition. The Stentys self-apposing stent (Stentys, France) is a 68 μm thick, self-expanding, nitinol BMS. Use of the Stentys resulted in fewer malapposed struts (0.58% vs 5.46%, p<0.001) and a lower proportion of patients with >5% malapposed struts (0% vs 28%, p<0.001), as assessed by OCT, compared with thin-strut, balloon expandable, cobalt–chromium BMS in a randomised trial of STEMI patients undergoing primary PCI (table 5).19 Self-expanding BMS have been associated with an increased risk of restenosis and, as such, LLL of the above mentioned stent platform amounted to 0.71 mm at 6 months. It remains to be seen whether further refinements of this technology, combining drug elution with stent self-expansion, will further improve clinical outcomes among STEMI patients.
Other novel coronary stents
MGuard mesh covered stent
A stainless steel stent covered with an ultrathin (20 μm) polyethylene terephthalate flexible micronet (MGuard, InspireMD, Israel) has been developed to immobilise thrombus and atheroma between the micronet and the vessel wall during stent expansion, mitigating distal embolisation (table 5). Among STEMI patients undergoing primary PCI, this device significantly increased the primary end point of complete (>70%) ST segment resolution (57.8% vs 44.7%, p=0.008) and improved TIMI 3 flow (91.7% vs 82.9%, p=0.006) compared with standard BMS and DES in a randomised clinical trial.20 The large scale MASTER II trial (N=1100) comparing efficacy (ST segment resolution at 60–90 min and infarct size at 2–7 days) and safety (death or reinfarction at 30 days) of the MGuard device with BMS and DES among STEMI patients undergoing primary PCI is planned to begin in 2013.
Conclusions
Several novel coronary devices have been developed and have undergone investigation in clinical trials. These include new DES with biodegradable polymer coatings, polymer-free DES, self-expanding stents, mesh covered stents, and fully biodegradable coronary scaffolds. While preliminary evidence is promising, it remains to be shown whether these novel devices are able to further improve the excellent safety and efficacy profile of contemporary DES among patients with coronary artery disease undergoing PCI.
Novel developments in coronary stents: key points
-
Drug eluting stents (DES) have significantly improved clinical outcomes as compared with bare metal stents, primarily through a notable reduction in the risk of repeat revascularisation.
-
Newer generation DES with thinner stent struts, novel durable or biodegradable polymer coatings, and new antiproliferative agents, have improved safety and efficacy outcomes compared with early generation DES, and are the standard of care in all patient and lesion subsets.
-
Several novel DES with biodegradable polymer coating, polymer-free DES, and fully biodegradable coronary scaffolds have been developed and are currently under clinical investigation.
-
Preliminary angiographic and clinical evidence is promising; however, it remains to be shown whether these novel devices are able to further improve the excellent safety and efficacy profile of currently used DES.
You can get CPD/CME credits for Education in Heart
Education in Heart articles are accredited by both the UK Royal College of Physicians (London) and the European Board for Accreditation in Cardiology—you need to answer the accompanying multiple choice questions (MCQs). To access the questions, click on BMJ Learning: Take this module on BMJ Learning from the content box at the top right and bottom left of the online article. For more information please go to: http://heart.bmj.com/misc/education.dtl
▸ RCP credits: Log your activity in your CPD diary online (http://www.rcplondon.ac.uk/members/CPDdiary/index.asp)—pass mark is 80%.
▸ EBAC credits: Print out and retain the BMJ Learning certificate once you have completed the MCQs—pass mark is 60%. EBAC/ EACCME Credits can now be converted to AMA PRA Category 1 CME Credits and are recognised by all National Accreditation Authorities in Europe (http://www.ebac-cme.org/newsite/?hit=men02).
Please note: The MCQs are hosted on BMJ Learning—the best available learning website for medical professionals from the BMJ Group. If prompted, subscribers must sign into Heart with their journal's username and password. All users must also complete a one-time registration on BMJ Learning and subsequently log in (with a BMJ Learning username and password) on every visit.
References
- ↵
- ↵
- ↵
- ↵Large scale cohort study showing a significant risk reduction of very late stent thrombosis with newer generation durable polymer everolimus eluting stents compared with early generation sirolimus eluting and paclitaxel eluting stents.
- ↵Individual patient data pooled analysis of three large scale trials providing evidence of improved safety (stent thrombosis) and efficacy (target lesion revascularisation) with biodegradable polymer drug eluting stents compared with early generation durable polymer sirolimus eluting stents.
- ↵Network meta-analysis indicating improved clinical outcomes with newer generation compared with early generation drug eluting stents.
- ↵Long term follow-up of an all-comer randomised trial demonstrating improved clinical outcomes with biodegradable polymer biolimus eluting stents compared with early generation durable polymer sirolimus eluting stents, primarily due to a significant risk reduction for very late stent thrombosis.
- ↵
- ↵References 8 and 9 are two large scale randomised trials showing equivalent outcomes with biodegradable polymer biolimus eluting stents and durable polymer everolimus eluting stents at 1 year.
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵First investigation of a fully bioresorbable drug eluting polymeric coronary scaffold.
- ↵
- ↵
- ↵First investigation of a fully bioresorbable drug eluting metallic coronary scaffold.
- ↵
- ↵
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online references
Footnotes
-
Contributors GGS drafted the first version of the manuscript that was revised critically for important intellectual content by SW and MT. All three authors have approved the final version of the manuscript.
-
Competing interests In compliance with EBAC/EACCME guidelines, all authors participating in Education in Heart have disclosed potential conflicts of interest that might cause a bias in the article. SW has received research contracts to the institution from Abbott, Boston Scientific, Biosensors, Cordis, and Medtronic. The other authors have no competing interests.
-
Provenance and peer review Commissioned; internally peer reviewed.