Article Text

Statistics from Altmetric.com
Learning objectives
Upon completion of this module, the reader will be able to:
Explain the mechanism of action and role of aspirin, clopidogrel, ticagrelor, vorapaxar, unfractionated heparin, low-molecular-weight heparins and fondaparinux in the medical management of patients with non-ST-segment elevation acute coronary syndromes.
Explain the side effects of aspirin, clopidogrel, ticagrelor, unfractionated heparin, low-molecular-weight heparins fondaparinux and rivaroxaban in the medical management of patients with non-ST-segment elevation acute coronary syndromes.
Recall the 2011 European Society of Cardiology guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation.
Introduction
Non-ST-segment elevation acute coronary syndromes (NSTE-ACS) comprise unstable angina and non-ST-segment elevation myocardial infarction (NSTEMI). Among patients admitted for myocardial infarction (MI), nearly two times more were hospitalised for NSTEMI as compared with ST-segment elevation myocardial infarction (STEMI) in a recent community-based registry.1 In the French Registry of Acute Coronary Syndrome (FAST) MI registry, only 20% of patients presenting with NSTEMI were managed conservatively, and 75% of these were aged ≥75 years. Patients with NSTEMI also had significantly more cardiovascular (CV) complications than those with STEMI.2 Moreover, medically managed patients with NSTE-ACS are at increased risk for recurrent events as compared with patients who undergo revascularisation as shown in clinical trials and national registries.3–5
Current NSTE-ACS guidelines recommend an assessment of ischaemic and bleeding risk using validated risk assessment methods to decide on pharmacological and invasive management.6 Ischaemic events continue to occur over time after NSTE-ACS, possibly because patients with NSTE-ACS are older and have more comorbidities than patients with STEMI. Therefore, NSTE-ACS treatment strategies must equally address the acute phase as well as long-term management. Some of the major goals of conservative strategy (CS) in NSTE-ACS are angina relief, improvement in myocardial perfusion, prevention of thrombus propagation, stabilisation of vulnerable plaque and reduction of long-term recurrent ischaemic event occurrence.
Since platelet function and coagulation play pivotal roles in thrombus generation at the site of vessel wall injury, a combination of antiplatelet and anticoagulant agents (together known as antithrombotic therapy) is the cornerstone of treatment for patients with NSTE-ACS. Since many patients with NSTE-ACS are elderly and have multiple comorbidities associated with both increased ischaemic and bleeding risks, it is often challenging to select a treatment strategy that achieves a desirable antithrombotic effect at an acceptable bleeding risk.
Antiplatelet therapy
Antiplatelet agents approved for conservative management of patients with NSTE-ACS include aspirin (acetylsalicylic acid) and P2Y12 receptor antagonists (ticagrelor, clopidogrel) (figures 1 and 2).

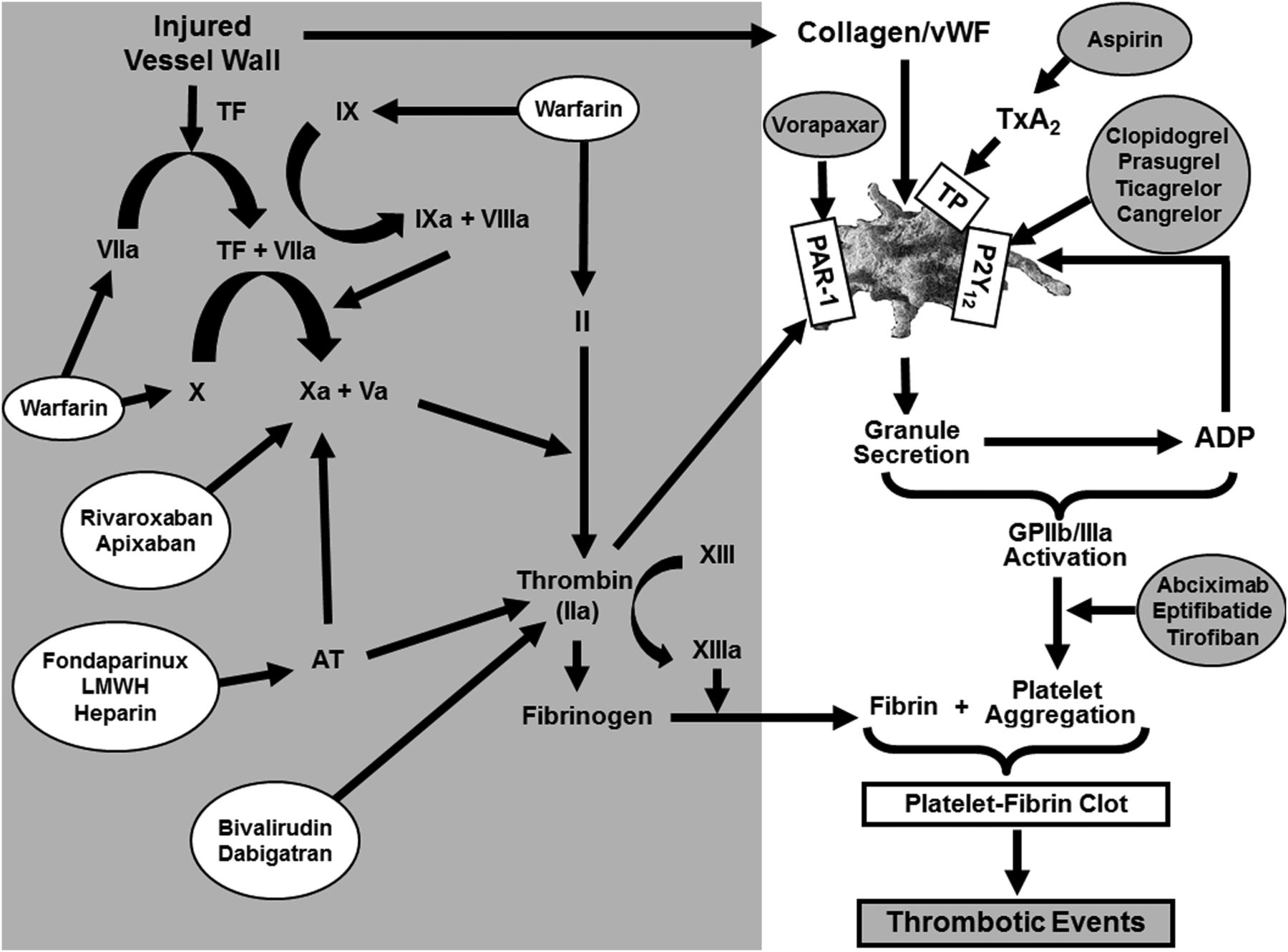
Antithrombotic therapy targets (adapted from Gurbel and Tantry41). During thrombosis, at the site of ‘altered’ vessel wall, exposure of the subendothelial matrix leads to adhesion and activation of platelets and subsequent release of secondary agonists, TxA2 and ADP. These two locally generated secondary agonists play a critical role in the sustained activation of GP IIb/IIIa receptors and stable platelet aggregation. During venous thrombosis, TF delivered by microparticles to the site of vessel wall injury binds to autoactivated factor VII (VIIa) to form TF–FVIIa complex which in turn activates factor X to Xa. Initial formation of small amounts of Xa initiates the coagulation process on the surface of activated platelets and leucocytes where large amounts of thrombin are generated. During arterial thrombosis, TF is exposed at the site of plaque rupture and initiates the coagulation process. Xa along with Va converts factor II to factor IIa. Simultaneously, trace amounts of thrombin activate factors VIII and V, which dramatically enhances catalytic activity of factors IX and X, respectively. Thrombin-activated factor XIIIa catalyses the formation of covalent cross-links between adjacent fibrin chains to form polymerised fibrin. Finally, together with aggregated platelets, the polymerised fibrin network leads to the formation of a stable, occlusive, platelet-fibrin clot and subsequent ischaemic events. Antiplatelet strategies in patients with NSTE-ACS treated with CS include aspirin and a P2Y12 receptor blocker (clopidogrel or ticagrelor). Anticoagulant strategies in patients with NSTE-ACS treated with CS are, heparin and fondaparinux. ADP, adenosine diphosphate; AT, antithrombin; CS, conservative strategy; Factor II, prothrombin; Factor IIa, thrombin; Factor I, fibrinogen; Factor Ia, fibrin; GP, glycoprotein; LMWH, low-molecular-weight heparin; NSTE-ACS, non-ST-segment elevation acute coronary syndromes; PAR-1, protease activated receptor-1; TxA2, thromboxaneA2; TF, tissue factor; TP, thromboxaneA2 receptor; vWF, von Willebrand factor.
Aspirin
The antithrombotic property of aspirin is primarily attributed to irreversible acetylation of the platelet cyclo-oxygenase (COX)-1 enzyme. Subsequently, both the generation of thromboxane (Tx)A2 and TxA2-induced platelet aggregation are inhibited for the lifespan of the platelets. Non-COX-1 effects of aspirin in platelets and other pleiotropic effects may also contribute to the antithrombotic properties.7
The optimal aspirin dose for NSTE-ACS is controversial. In a meta-analysis, daily doses of 75–1500 mg showed similar clinical efficacy, while doses lower than 75 mg/day demonstrated a 50% reduction in efficacy.8 Current guidelines are presented in box 1. When administered in conjunction with ticagrelor, aspirin, 75–100 mg/day is the recommended dosage; more than 100 mg daily aspirin may decrease the effectiveness of ticagrelor. A non-enteric-coated tablet is recommended as initial therapy as it provides more rapid buccal absorption and immediate antiplatelet effect. There is a strong rationale for concomitant use of aspirin even if other antithrombotic drugs such as clopidogrel or warfarin are administered.
2015 ESC recommendations for antiplatelet agents in medically managed patients with NSTE-ACS (adapted from Roffi et al6)
Antiplatelet agents
Aspirin
Aspirin is recommended for all patients without contraindications at an initial oral loading* dose of 150–300 mg (in aspirin-naive patients) and a maintenance dose of 75–100 mg/day long-term regardless of treatment strategy (class I, level A)
P2Y12 inhibitor
A P2Y12 inhibitor is recommended, in addition to aspirin, for 12 months unless there are contraindications such as excessive risk of bleeds (class I, level A).
Ticagrelor (180 mg loading dose, 90 mg twice daily) is recommended, in the absence of contraindications,† for all patients at moderate-to-high risk of ischaemic events (eg, elevated cardiac troponins), regardless of initial treatment strategy and including those pretreated with clopidogrel (which should be discontinued when ticagrelor is started) (class I, level B).
Clopidogrel (300–600 mg loading dose, 75 mg daily dose) is recommended for patients who cannot receive ticagrelor or prasugrel or who require oral anticoagulation (class I, level B).
P2Y12 inhibitor administration in addition to aspirin beyond 1 year may be considered after careful assessment of the ischaemic and bleeding risks of the patient (class IIb, level A).
A proton pump inhibitor in combination with DAPT is recommended in patients at higher than average risk of gastrointestinal bleeds (ie, history of gastrointestinal ulcer/haemorrhage, anticoagulant therapy, chronic NSAID/corticosteroid use or two or more of the following: age ≥65 years, dyspepsia, gastro-oesophageal reflux disease, Helicobacter pylori infection, chronic alcohol use) (class I, level B).
*Non-enteric-coated formulation; 75–150 mg intravenously if oral ingestion is not possible.
†Contraindications for ticagrelor: previous intracranial haemorrhage or ongoing bleeds. Contraindications for prasugrel: previous intracranial haemorrhage, previous ischaemic stroke or transient ischaemic attack or ongoing bleeds; prasugrel is generally not recommended for patients aged ≥75 years or with a bodyweight <60 kg.
DAPT, dual antiplatelet therapy; NSAID, non-steroidal anti-inflammatory drugs; NSTE-ACS, non-ST-segment elevation acute coronary syndromes.
The most common side effect of aspirin treatment is gastrointestinal intolerance. In patients with coronary artery disease treated with aspirin, the incidence of upper gastrointestinal bleeding was 1.5% per year, which was significantly associated with morbidity.9 Clopidogrel is recommended for patients who are allergic to, or who cannot tolerate, aspirin. Concomitant administration of non-steroidal anti-inflammatory drugs (NSAIDs) should be avoided if possible. NSAIDs, particularly ibuprofen, affect the access of aspirin to its binding site within COX-1 and influence its antithrombotic efficacy. Either alternative NSAIDs should be administered or administration of ibuprofen should be delayed at least 30 min after immediate-release aspirin or at least 8 h before aspirin administration.7
P2Y12 receptor antagonists
Although TxA2 and adenosine diphosphate (ADP) act synergistically during platelet aggregation, the ADP–P2Y12 receptor interaction plays a central role in sustaining the activation of glycoprotein (GP) IIb/IIIa receptors by amplifying the response to agonists. P2Y12 activation also modulates platelet procoagulant activity, P-selectin expression and inflammation.10
Clopidogrel
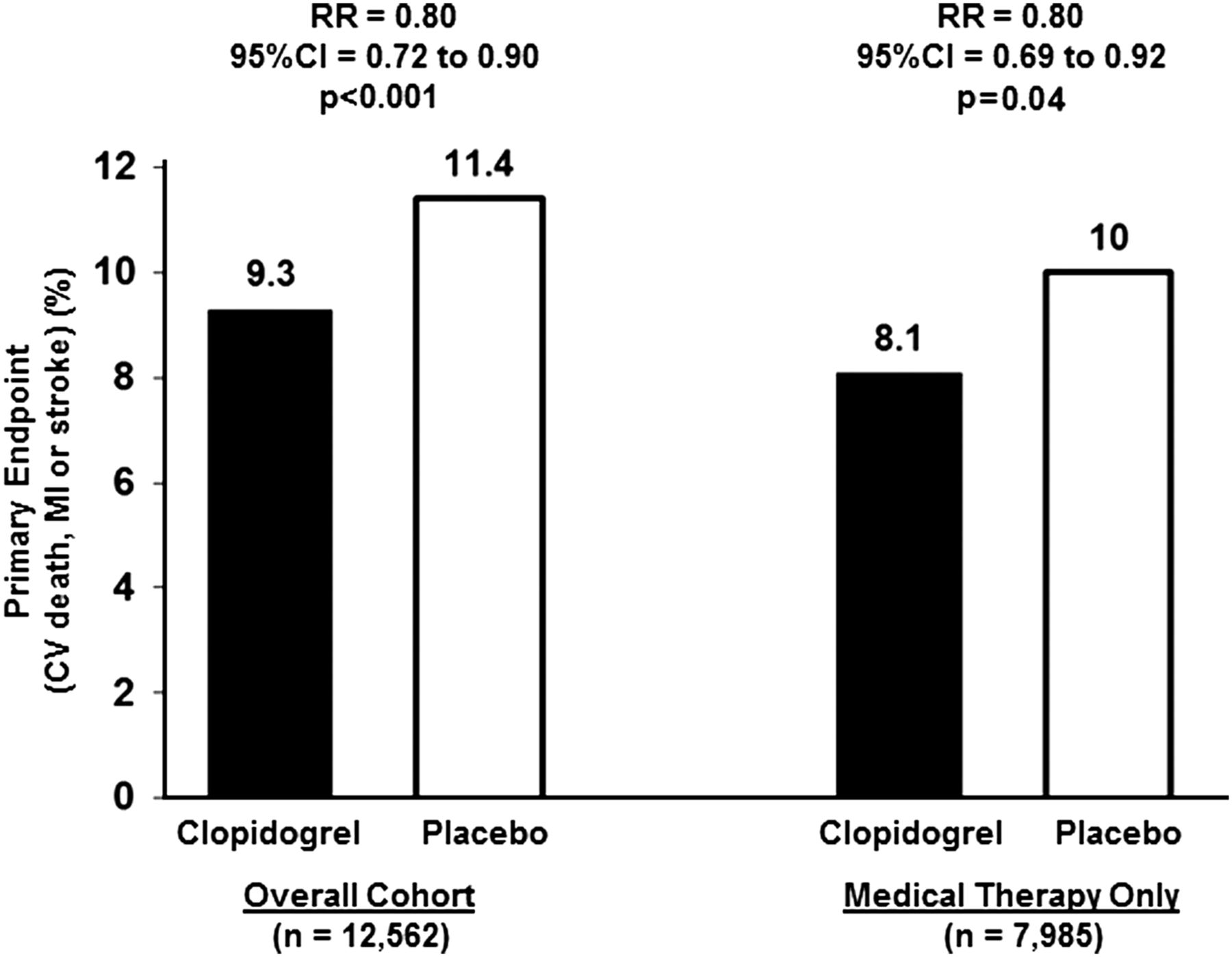
Once absorbed, ∼85% of the clopidogrel is converted by esterases into an inactive metabolite (SR26334), and the remaining 15% of the prodrug undergoes a two-step activation process mediated by several cytochrome P450 (CYP) enzymes, mainly CYP2C19 and CYP3A4, to produce a major active metabolite (R-130964). This active metabolite forms a disulfide bond selectively with P2Y12 and inhibits the binding of ADP to the receptor, thereby irreversibly inhibiting ADP-stimulated platelet aggregation.10 Since the ADP–P2Y12 interaction is pivotal for the amplification of platelet activation and stable platelet thrombus generation, the early focus of antithrombotic therapy has been inhibition of the P2Y12 receptor. In the Clopidogrel in Unstable Angina to Prevent Recurrent Events (CURE) study, clopidogrel therapy (300 mg loading dose followed by 75 mg/day) and aspirin (75–325 mg/day) in patients (n=12 562) with NSTE-ACS was associated with 20% reduction in the combined end point of CV mortality, non-fatal MI and stroke (9.3% vs 11.4%, p<0.001). A significant increase in major bleeding (3.7% vs 2.7%, p=0.001) and a non-significant increase in life-threatening bleeding (2.1% vs 1.8%, p=0.13) and no difference in fatal bleeding (0.2% vs 0.2%) with dual antiplatelet therapy (DAPT) compared with aspirin monotherapy were observed. Among 7985 patients treated medically and without revascularisation, DAPT therapy was associated with similar reduction in primary end point occurrence (8.1% vs 10.0%; risk reduction (RR)=0.80) compared with the overall trial results (figure 3).11 The results of the CURE trial strongly influenced the current strategy of DAPT with aspirin plus a P2Y12 receptor inhibitor for the treatment of the patients with NSTE-ACS.

Primary outcome of Clopidogrel in Unstable Angina to Prevent Recurrent Events trial in overall and NSTE-ACS cohorts (adapted from Fox et al11). CV, cardiovascular; MI, myocardial infarction; NSTE-ACS, non-ST-segment elevation acute coronary syndromes; RR, risk reduction.
Pharmacodynamic studies in patients undergoing stenting indicate that clopidogrel is associated with variable and moderate levels of irreversible platelet inhibition, and a delayed onset of effect. High on-treatment platelet reactivity (HPR), observed in approximately one in three patients treated with clopidogrel, has been strongly linked to poststenting ischaemic event occurrence.12 However, the clinical relevance of HPR in patients with medically managed ACS is less clear. In the Targeted Platelet Inhibition to Clarify the Optimal Strategy to Medically Manage Acute Coronary Syndromes (TRILOGY ACS) platelet function substudy, patients with medically managed ACS were treated with prasugrel versus clopidogrel on top of aspirin and HPR was associated with the occurrence of the primary composite end point of CV death, MI or stroke through 30 months in an unadjusted but not in an adjusted analysis.13
Clopidogrel metabolism is influenced by single-nucleotide polymorphisms (SNPs) of genes encoding cytochrome isoenzymes (CYP2C19*2 in particular), concomitant administration of drugs that either compete with or inhibit the same cytochrome isoenzymes associated with clopidogrel metabolism and other factors such as smoking, increased bodyweight, renal inefficiency and diabetes. The presence of a loss-of-function allele has been associated with a diminished pharmacodynamic response to clopidogrel and an increased risk for poststenting ischaemic event occurrences. However, in medically managed patients with NSTE-ACS, the influence of SNP carriage on outcomes in patients treated with clopidogrel is unclear. In addition to loss-of-function allele carriage, clopidogrel has a lesser pharmacodynamic effect in patients treated with proton pump inhibitors, particularly omeprazole.10
Prolonged or permanent withdrawal of clopidogrel is discouraged in high-risk patients unless strongly clinically indicated. In very high-risk patients in whom cessation of antiplatelet therapy before surgery seems to carry a high risk (eg, within the first weeks after stent implantation), it has been suggested to switch before surgery to a short half-life and reversible antiplatelet agent, for example, the GP IIb/IIIa receptor inhibitors (tirofiban or eptifibatide), and DAPT should be resumed as soon as considered safe.6
Prasugrel
Prasugrel is a third-generation thienopyridine associated with greater active metabolite generation resulting in a more rapid and potent pharmacodynamic effect than clopidogrel. Prasugrel therapy is also associated with much less non-responsiveness, drug–drug interactions and loss-of-function allele influence than clopidogrel.14
The TRILOGY trial was designed to evaluate whether aspirin plus prasugrel is superior to aspirin plus clopidogrel for long-term therapy in patients with NSTE-ACS who did not undergo revascularisation. In this trial, prolonged treatment with prasugrel was not associated with reduced rate of major CV events compared with clopidogrel.15 Currently, prasugrel is not recommended for conservative management in patients with NSTE-ACS.
Ticagrelor
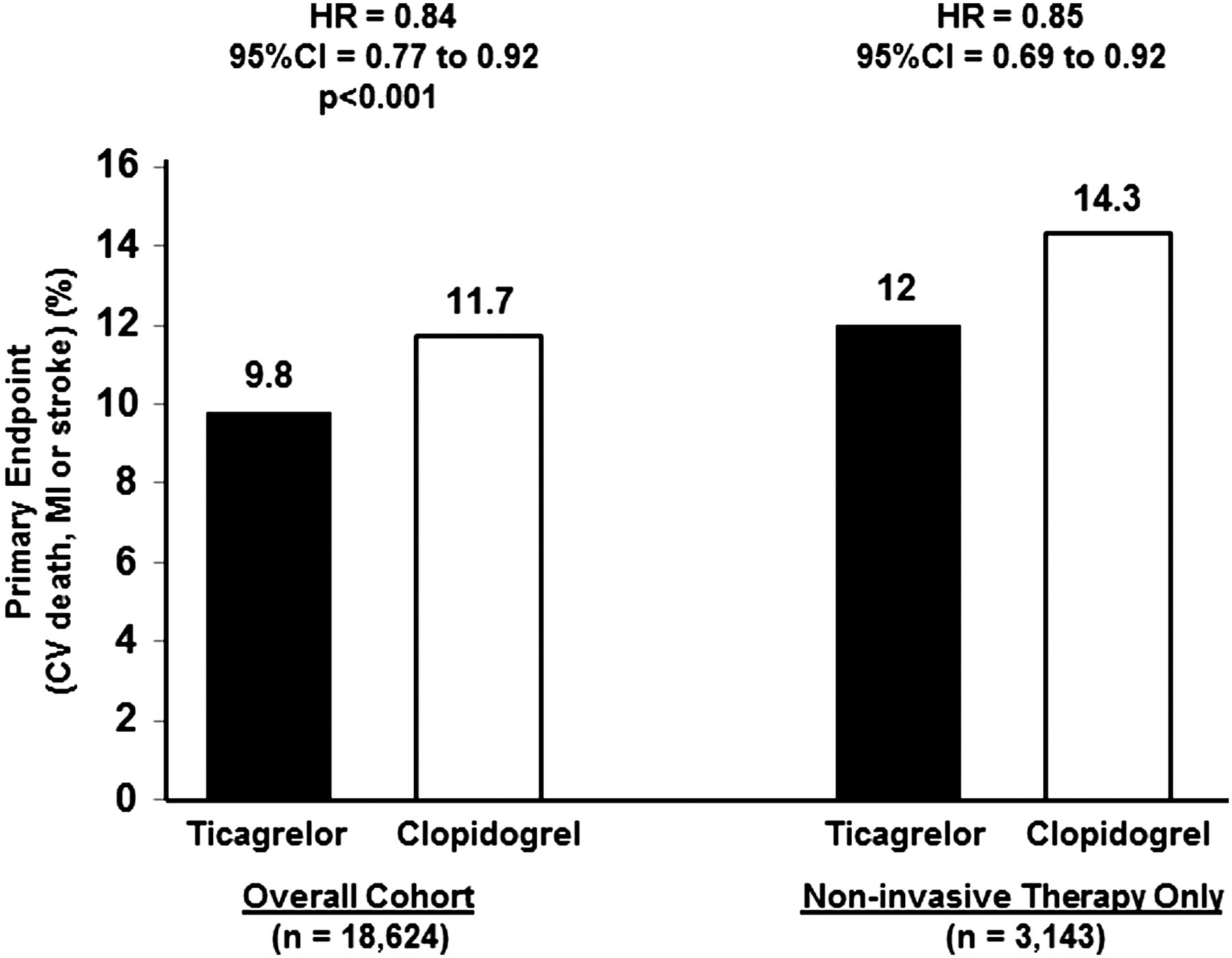
Ticagrelor, a cyclopentyltriazolopyrimidine derivative, is associated with a more rapid onset and offset of action, and greater platelet inhibition compared with clopidogrel. Ticagrelor is metabolised rapidly by CYP3A4/5 to produce AR-C124910XX, the main metabolite of ticagrelor that has been reported to be equipotent in inhibiting the P2Y12 receptor.16 ,17 In the PLATelet inhibition and patient Outcomes (PLATO) trial (n=18 624), ticagrelor therapy was associated with a significant reduction in the primary efficacy end point of vascular death, MI or stroke compared with clopidogrel at 30 days (4.8% vs 5.4%, p=0.045) and at 12 months (9.8% vs 11.7%, p<0.001) in patients with ACS treated with both conservative and invasive strategies. A remarkable observation from the PLATO trial was the significant reduction in CV and all-cause mortality associated with ticagrelor therapy. The latter effect has been attributed to greater platelet inhibition and the off-target effect of adenosine reuptake inhibition. There were no differences between ticagrelor and clopidogrel in the primary safety end point of major bleeding, as defined by either the study protocol (ticagrelor 11.6% vs clopidogrel 11.2%, p=0.43) or the Thrombolysis In Myocardial Infarction (TIMI) criteria (7.9 vs 7.7%, p=0.57), but non-coronary artery bypass graft surgery (CABG)-related major bleeding was higher following ticagrelor treatment (4.5% vs 3.8%, p=0.026 and 2.8% vs 2.2%, p=0.03, for protocol and TIMI study group defined bleeding events, respectively).18 Twenty-eight per cent of patients (5216/18 624) were intended for the non-invasive treatment strategy in the PLATO trial and among these patients 4636 had NSTE-ACS, but only 60% of the patients intended for non-invasive therapy (n=3143) were finally managed totally with a CS by the end of follow-up. Similar to overall results of the PLATO trial, ticagrelor therapy was associated with a significant reduction in the primary end point (12.0% vs 14.3%, p=0.04) and a lower mortality rate (6.1% vs 8.2%, p=0.01) in patients intended for a non-invasive strategy (figure 4). The primary safety end point of major bleeding, as defined by either the study protocol (ticagrelor 11.9% vs clopidogrel 10.3%, p=0.079) or TIMI criteria (7.9% vs 7.2%, p=0.27) were similar between ticagrelor versus clopidogrel therapy in this cohort.19 Similar results were observed in another retrospective analysis of the PLATO trial. Among patients with NSTE-ACS treated with revascularisation (5,714) or not (n=5366), ticagrelor therapy was associated with reduced primary outcome (HR 0.86 vs 0.85, interaction p=0.93) and all-cause death (HR 0.75 vs 0.73, interaction p=0.89) and there was no significant increase in overall major bleeding.20

Despite superior clinical outcomes with ticagrelor therapy in the PLATO trial, the drug did not demonstrate a superior clinical effect in the North American patient population. The latter observation has been linked to a higher aspirin dose used in North America. In addition, ticagrelor did not demonstrate a superior effect in patients with unstable angina. Dyspnoea was a much more frequent side effect of ticagrelor therapy as compared with clopidogrel. Minor adverse effects of ticagrelor therapy include increased ventricular pauses, spontaneous major bleedings and elevated uric acid and creatinine levels. Ticagrelor is contraindicated in patients with a history of intracranial haemorrhage (ICH), active pathological bleeding and severe hepatic impairment. Ticagrelor should not be administered to patients treated with strong CYP3A inhibitors or CY3A inducers given the above noted metabolic pathway. Patients receiving more than 40 mg/day of simvastatin or lovastatin may be at increased risk of statin-related adverse effects when concomitantly treated with ticagrelor.6 ,21 The most remarkable observation of the PLATO trial was a significant and consistent reduction in mortality. Therefore, ticagrelor can be administered as a first-line P2Y12 inhibitor therapy in preference to clopidogrel in patients with medically managed NSTE-ACS patients.
Thrombin receptor antagonists
Inhibition of the thrombin–protease activated receptor (PAR)-1 interaction may further attenuate ischaemic event occurrence in selected patients treated with DAPT. Vorapaxar, a PAR-1 inhibitor, was studied on top of standard antiplatelet therapy for the acute treatment of patients with NSTE-ACS in the Thrombin Receptor Antagonist for Clinical Event Reduction in Acute Coronary Syndrome (TRACER) study (n=12 944). The study was prematurely stopped due to increased bleeding in the vorapaxar group. In TRACER, vorapaxar did not significantly reduce the primary composite end point occurrence of CV death, MI, stroke, hospitalisation for ischaemia or urgent revascularisation (18.5% vs 19.9%; p=0.07). There was a 1.35-fold increase in moderate and severe bleeding (7.2% vs 5.2%; p<0.001) and a 3.39-fold increase in ICH with vorapaxar therapy (1.1% vs 0.2%, p<0.001).22
In the Thrombin Receptor Antagonist in Secondary Prevention of Atherothrombotic Ischaemic Events-TIMI 50 (TRA2°P-TIMI 50) trial, patients with a history of spontaneous MI or ischaemic stroke within 2 weeks to 12 months or peripheral arterial disease (n=24 449) were treated with vorapaxar or placebo on top of standard medical care. TRA2°P was run concurrently with TRACER. Because of an alarming rate of ICH observed in patients with prior stroke treated with vorapaxar, the Data Safety Monitoring Board recommended that vorapaxar be discontinued in patients enrolled in TRA2°P with prior stroke and in patients who suffered a stroke during the study. In the overall study, vorapaxar therapy was associated with a significantly lower rate of the composite end point occurrence of 3-year CV death, MI or stroke (9.3% vs 10.5%, p<0.001), with an increase in the primary safety end point occurrence of the Global Use of Strategies to Open Occluded Arteries (GUSTO) moderate or severe bleeding (4.2% vs 2.5%, p<0.001) and in ICH (1.0% vs 0.5%; p<0.001).23
In the post-MI group of TRA2°P with no history of stroke or transient ischaemic attack (TIA) (n=16 897, 64% of the overall population), vorapaxar therapy was associated with a significant reduction in the composite end point occurrence of CV death, MI and stroke (7.4% vs 9.0%, p<0.001), which was mainly attributed to a significant reduction in MI (4.6% vs 5.7%; p<0.001). There was an increase in the primary safety end point occurrence of GUSTO moderate or severe bleeding (3.0% vs 2.0%, p<0.001), major or minor TIMI bleeding (3.4% vs 2.3%; p<0.001) and a non-significantly increased rate of ICH (0.5% vs 0.4%; HR=1.44; p=0.160).24 The European Medicines Agency approved the coadministration of vorapaxar and aspirin and, where appropriate, clopidogrel, to reduce atherothrombotic events in adult patients with a history of MI. It is contraindicated in patients with a history of stroke or TIA and ICH and patients with any active pathological bleeding, hypersensitivity to the active substance and severe hepatic impairment.25
Glycoprotein IIb/IIIa inhibitors
The GP IIb/IIIa receptor is the most abundant platelet GP receptor with ∼80 000 receptors present per platelet. Platelet activation by various agonists and stimuli induces a conformational change in GP IIb/IIIa receptor that markedly enhances its affinity for fibrinogen and platelet–platelet aggregation. In addition to inhibition of platelet aggregation, GP IIb/IIIa inhibitors induce platelet disaggregation and may attenuate microembolisation and the release of vasoconstrictors. The three GP IIb/IIIa inhibitors approved for intravenous administration, abciximab, eptifibatide and tirofiban, have different pharmacodynamic properties. Reduction in death or MI was observed with GP IIb/IIIa inhibitor therapy in a meta-analysis of 29 570 patients initially managed medically and planned for PCI (10.7% vs 11.5%, p=0.02), but not in patients exclusively managed with CS. Increased major bleeding complications and thrombocytopenia, but not intracranial bleeding was demonstrated in patients treated with GPIs compared with placebo.26 The increased use of the prasugrel or ticagrelor, P2Y12 inhibitors with a rapid onset of potent pharmacodynamic effects, may obviate the future role of GP IIb/IIIa inhibitors in the treatment of patients with NSTE-ACS. In patients with NSTE-ACS managed conservatively, GP IIb/IIIa inhibitor therapy is not recommended for patients on DAPT.6
Anticoagulants
It has been demonstrated that anticoagulation therapy is effective in addition to antiplatelet therapy and the combination of antiplatelet and anticoagulant therapies are more effective than either treatment alone.27 ,28
Major anticoagulants are:
indirect thrombin inhibitors that require antithrombin-III for action—unfractionated heparin (UFH) and low-molecular-weight heparins (LMWHs)
indirect Xa inhibitors that require antithrombin for their full action—LMWHs and fondaparinux
direct factor Xa inhibitors (xabans)—apixaban, rivaroxaban
direct thrombin inhibitors—dabigatran and bivalirudin.
Among patients treated conservatively for NSTE-ACS, the recommended major anticoagulants are UFH, LMWHs and fondaparinux. The guidelines do not recommend the use of bivalirudin among conservatively managed patients due to limited data.6
Unfractionated heparin
UFH is a heterogeneous mixture of polysaccharide molecules. The pentasaccharide sequence of UFH binds to antithrombin and enhances the inhibition of thrombin and also factor Xa. In a pooled analysis of randomised trials enrolling patients with NSTE-ACS, short-term UFH versus placebo was associated with significant RR in death and MI (OR=0.67, p=0.04), whereas UFH plus aspirin versus aspirin was associated with a trend towards a benefit, but with an increased risk of bleeding.28
UFH strongly binds to plasma proteins resulting in unpredictable levels of free heparin in the circulation. Therefore, UFH is associated with significant variability in antithrombotic effects and requires close monitoring. Another disadvantage is the need for continuous intravenous administration and heparin-induced thrombocytopenia, which can occur with or without thrombosis in patients with ACS. Serial haemoglobin/haematocrit and platelet counting are recommended during UFH therapy to monitor thrombocytopenia. Mild thrombocytopenia may occur in 10%–20% of patients, whereas significant thrombocytopenia (platelet count <100 000) occurs in 1%–5% of patients and typically appears after several days of therapy. The more dangerous complication of immune-mediated heparin-induced thrombocytopenia with thrombosis occurs more rarely (<0.2%). Thrombocytopenia typically resolves after discontinuation of heparin.29
Low-molecular-weight heparins
LMWHs have a lesser inhibitory effect on thrombin than factor Xa, less plasma binding, greater bioavailability and a lower risk of immune-mediated thrombocytopenia than UFH. LMWH therapy can be administered subcutaneously on a weight basis and does not require dose monitoring. The benefit of LMWH therapy may be more pronounced in the setting of a CS as demonstrated in older trials. To date, the best investigated LMWH in cardiology is enoxaparin. In a meta-analysis of 21 946 patients, enoxaparin versus UFH was associated with ∼10% reduction in combined end point of 30 days death or MI (10.1% vs 11.0%), with no significant differences in major bleeding outcomes in patients with ACS and this analysis included patients managed with CS.30 Overall, in patients with ACS, LMWHs are superior to UFH in decreasing the risk of major adverse cardiac events (MACE), despite a mild increase in bleeding. Patients with renal insufficiency require lower doses since LMWHs are renally cleared. Similar to UFH, a ‘rebound’ phenomenon has been observed with cessation of LWMH therapy. It is unclear to what extent this older observation is clinically relevant in the current era of ACS management with potent P2Y12 receptor blockade.
Fondaparinux
Fondaparinux is a synthetic pentasaccharide that is structurally similar to the antithrombin binding site of heparin and LMWH. Fondaparinux reversibly binds to antithrombin with high affinity and catalyses the antithrombin-mediated inhibition of factor Xa. Fondaparinux can be administered in a fixed dose subcutaneously (2.5 mg once daily) and weight-based adjustment. Routine monitoring is not necessary since fondaparinux is associated with a predictable antithrombotic effect and has low interindividual variability and intraindividual variability. The agent is rapidly absorbed and completely bioavailable with a predictable dose-dependent response. Finally, we have no significant clinical trial evidence to support fondaparinux on top of potent P2Y12 inhibitors.
In the Fifth Organization to Assess Strategies in Acute Ischemic Syndromes Investigators (OASIS 5) trial, 20 078 patients with NSTE-ACS were treated with fondaparinux versus enoxaparin; both agents were administered subcutaneously for a mean of 6 days. More patients in this trial were managed conservatively than in other current ACS trials: overall, approximately two-thirds of patients underwent diagnostic coronary angiography. The rates of the primary composite end point of death, MI or refractory ischaemia at 9 days were similar between fondaparinux and enoxaparin (5.8% vs 5.7%) and mortality rates at 30 days (2.9% vs 3.5%) and at 180 days (5.8% vs 6.5%) were significantly lower with fondaparinux, but bleeding events were significantly lower with fondaparinux (2.2% vs 4.1%, p<0.001) that persisted at 30 and 180 days follow-up (figure 5). Lower bleeding in fondaparinux group led to the recommendation in the guidelines for the use of this agent in conservatively managed patients (box 2).31
Current ESC Recommendations for Antiplatelet agents and anticoagulants in Medically Managed patients with NSTE-ACS
20015 ESC recommendations for anticoagulation in medically managed patients with NSTE-ACS
Parenteral anticoagulation is recommended at the time of diagnosis according to both ischaemic and bleeding risks (class I, level B).
Fondaparinux (2.5 mg daily) is recommended as having the most favourable efficacy–safety profile regardless of the management strategy (class I, level B).
Enoxaparin (1 mg/kg subcutaneously twice daily) or UFH is recommended when fondaparinux is not available (class I, level B).
Crossover between UFH and LMWH is not recommended (class III, level B).
In patients with NSTEMI with no prior stroke/TIA and at high ischaemic risk as well as low bleeding risk receiving aspirin and clopidogrel, low-dose rivaroxaban (2.5 mg twice daily for approximately 1 year) may be considered after discontinuation of parenteral anticoagulation (class IIb, level B).
2015 ESC recommendations for combining antiplatelet agents and anticoagulants medically managed patients with NSTE-ACS requiring chronic oral anticoagulation
In patients with a firm indication for an oral anticoagulant (eg, atrial fibrillation with a CHA2DS2-VASc score ≥2, recent venous thromboembolism, LV thrombus or mechanical valve prosthesis), oral anticoagulant is recommended in addition to antiplatelet therapy (class I, level C).
One antiplatelet agent in addition to oral anticoagulant should be considered for up to 1 year (class IIA, level C).
LMWH, low-molecular-weight heparins; LV, left ventricular; NSTE-ACS, non-ST-segment elevation acute coronary syndromes; NSTEMI, non-ST-segment elevation myocardial infarction; TIA, transient ischaemic attack; UFH, unfractionated heparin.

Outcomes in Fifth Organization to Assess Strategies in Acute Ischemic Syndromes Investigators trial (adapted from Yusuf et al31). CV, cardiovascular; MI, myocardial infarction; RI, refractory ischaemia.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
A decision algorithm of antithrombotic therapy in medically managed patients with NSTE-ACS. NSAID, non-steroidal anti-inflammatory drug; NSTE-ACS, non-ST-segment elevation acute coronary syndromes; NSTEMI, non-ST-segment elevation myocardial infarction; TIA, transient ischaemic attack; UFH, unfractionated heparin.
Rivaroxaban
Factor Xa plays a pivotal role in the amplification of thrombin generation. Compared with thrombin, factor Xa has fewer effects in addition to coagulation and together with factor Va (prothrombinase complex), the function of factor Xa is mainly confined to the conversion of prothrombin to thrombin. Moreover, factor Xa inhibition only prevents thrombin generation and does not affect pre-existing thrombin. The latter properties have been proposed to explain the superior safety profile of Xa inhibitors compared with other anticoagulants such as heparin or warfarin.
Rivaroxaban is an oral, direct factor Xa inhibitor with high oral bioavailability, rapid onset of action and a half-life of 7–10 h. In the phase II, Anti-Xa Therapy to Lower Cardiovascular Events in Addition to Standard Therapy in Subjects With Acute Coronary Syndrome ACS –Thrombolysis In Myocardial Infarction 46 (ACS-TIMI 46) trial 3491 patients were randomised within 1–7 days after hospital administration for ACS; ∼48% of patients had NSTE-ACS and ∼35% of patients were not treated with PCI for index event. The ATLAS ACS-TIMI 46 trial demonstrated that the addition of rivaroxaban to aspirin or DAPT in patients stabilised after an ACS increased bleeding in a dose-dependent manner and reduced efficacy end point of death, MI or stroke. However, in the NSTE-ACS cohort, rivaroxaban was associated with significantly increased bleeding (13.8% vs 3.6%, p<0.0001) and numerically increased efficacy end point rate (7.2% vs 6.8%, HR=1.05).32
In the subsequent phase III ATLAS TIMI 51 trial, 15 526 patients within 7 days of hospitalisation for ACS were randomly treated with twice-daily doses of either 2.5 or 5 mg rivaroxaban versus placebo. In this study, 50% of patients had NSTE-ACS and ∼40% of patients were not treated with PCI or CABG for index event. In this trial, twice-daily 2.5 mg rivaroxaban was associated with significantly reduced primary end point of composite of CV death, MI or stroke (9.1% vs 10.7%, p=0.02), and death from CV causes (2.7% vs 4.1%, p=0.002) or from any cause (2.9% vs 4.5%, p=0.002) compared with placebo. Rivaroxaban therapy was associated with increased TIMI major bleeding not associated with CABG with both doses but with fewer fatal bleeding events occurred in patients treated with twice-daily 2.5 mg dose compared with 5 mg dose (0.1% vs 0.4%, p=0.04). In patients with NSTE-ACS, efficacy and safety outcomes were similar to overall trial results.33 Based on the favourable outcomes, rivaroxaban is approved in the European Union to prevent atherothrombotic events after an ACS (NSTE-ACS or STEMI) and the recommended dose is 2.5 mg that should be coadministered with 75–100 mg aspirin alone or with 75–100 mg aspirin plus 75 mg daily clopidogrel or a standard daily dose of ticlopidine. Rivaroxaban therapy should be initiated immediately after stabilisation of ACS events (including revascularisation), but ≥24 h after hospitalisation and at the time parenteral anticoagulation would normally be discontinued. Extending duration beyond 1 year should be done on individual basis. Since potent P2Y12 inhibitors such as ticagrelor and prasugrel are associated with an increased bleeding risk compared with clopidogrel, and there is an absence of clinical experience with the latter combinations, it is not advisable at this time to add rivaroxaban to ticagrelor or prasugrel ± aspirin. Moreover, the ATLAS trial primarily studied the effect of rivaroxaban added to clopidogrel + aspirin.
Duration of antithrombotic therapy for medically managed NSTEMI
Since medically managed NSTEMI patients are inherently at high risk for long-term recurrent event occurrences and are at even higher risk than patients managed with PCI, determination of optimal duration of antithrombotic therapy is important.3–5 However, unlike studies of patients treated with stenting, there are less large-scale randomised trial data available from clinical trials enrolling only medically managed patients. Based on the results of the CURE trial, 1 year DAPT with aspirin and clopidogrel is recommended irrespective of the management strategy.11 In a recent meta-analysis undergoing stenting, extended DAPT was associated with significantly reduced MI and stent thrombosis, but at the expense of more major bleeding and increased all-cause death among stented patients.34 In the TRILOGY ACS trial, an investigation solely enrolling patients with NSTE-ACS managed medically, overall prasugrel was associated with a similar primary efficacy end point and severe and intracranial bleeding. In a time-dependent analysis of recurrent events using a 12-month landmark time point, a significant interaction with treatment and time was observed with a divergence of treatment effect after 12 months of therapy among patients under the age of 75 years (p=0.02). The risk of recurrent ischaemic events in the prasugrel group was lower after 12 months (HR for <12 months, 0.94 (95% CI 0.79 to 1.12), vs HR for ≥12 months, 0.64 (95% CI 0.48 to 0.86)). The latter observation was consistent for both primary and component end points and was more evident in patients who had angiography done for ACS and anatomic coronary disease was confirmed.15 ,35
In this line, the Providing Regional Observations to Study Predictors of Events in the Coronary Tree (PROSPECT) trial, a prospective natural-history study of coronary atherosclerosis after an ACS, demonstrated a near-linear event rate over a 3-year period, with almost 50% of later CV events occurring in non-culprit lesions.36 These study results strongly demonstrate continued occurrence of ischaemic events beyond 1 year of recommended DAPT. Other indirect evidence to support antiplatelet therapy beyond 1 year came from the Clopidogrel for High Atherothrombotic Risk and Ischemic Stabilization, Management and Avoidance (CHARISMA), Prevention of Cardiovascular Events in Patients with Prior Heart Attack Using Ticagrelor Compared to Placebo on a Background of Aspirin–Thrombolysis in Myocardial Infarction 54 and TRA2°P-TIMI 50 trials.23 ,37 ,38 In the CHARISMA trial, in the overall cohort of patients with prior MI, stroke and peripheral arterial disease (n=9748, ∼25% patients underwent PCI and ∼17% had coronary artery bypass surgery), a median of 28 months of DAPT versus low-dose aspirin was associated with a significant reduction in primary end point of CV death, MI or stroke and a consistent elevation in the Kaplan–Meyer event curve over time in both groups was observed. Among patients with prior MI (n=4441), DAPT was associated with 23% reduction in the primary end point (8.3% vs 6.6%, HR (95% CI)=0.774 (0.624 to 0.978), p=0.031).37
In the PEGASUS trial, the efficacy and safety of 90 and 60 mg twice daily ticagrelor in addition to low-dose aspirin versus placebo for a median of 33 months in stable patients with a history of spontaneous MI 1–3 years before randomisation (41% had NSTEMI and 17% were not treated with PCI) was evaluated. Both doses of ticagrelor therapy were associated with a significantly reduced risk of CV death, MI or stroke and increased major bleeding in patients treated with PCI and without PCI (p for interaction was not significant for both doses) and the net clinical benefit favoured the 60 mg dose.38
It is important to note that despite potent P2Y12 blockade with ticagrelor in PEGASUS and PLATO, there was robust evidence of continued ischaemic event occurrence (ie, treatment failure with a potent P2Y12 receptor blocker). The latter sobering observation serves as the rationale for targeting other pathways involved in platelet activation and coagulation. In the landmark TRA2°P-TIMI 50 trial, PAR-1 blockade with vorapaxar therapy was associated with a significant reduction in the primary ischaemic end point both in the first year of treatment and also beyond 1 year, to 36 months.23
The totality of evidence above strongly indicates the continued risk among patients with prior MI and demonstrates the significant anti-ischaemic benefits of extended antiplatelet therapy beyond 1 year, but at the expense of increased bleeding. Therefore, more precise identification of high-risk patient subgroups where net clinical benefit favours long-term intensified antiplatelet therapy is an important goal for future research studies. In this line, some interesting points based on the timing of last P2Y12 inhibitor dose were observed in a recent subanalysis of the PEAGASUS trial. A 47% increase in primary end point was observed in those patients who discontinued P2Y12 inhibitor ≤30 days as compared with those who discontinued P2Y12 inhibitor after 1 year in the placebo group. It appears that the greatest benefit of extended DAPT with ticagrelor is confined to patients who continue or restart after only a brief interruption of P2Y12 inhibition (a 27% relative RR (p<0.001) in MACE but with an increased TIMI major bleeding), but not in patients who were stable for more than 2 years from their MI and safely off P2Y12 inhibition for more than a year.39 However, in the real-world, identification of patients in advance who are eligible for extended therapy without significant bleeding risk and who can safely discontinue therapy is a vexing major clinical issue. That is because, atherothrombosis is a dynamic process, and the stability of the platelet reactivity phenotype and the hypercoagulability state over time remains unclear. Therefore, in addition to traditional clinical variables, such as the period of time safely off P2Y12 inhibitor, we desperately need more specific markers that better identify the presence of vulnerable vasculature and vulnerable blood that causes high risk in the individual patient. The latter should be the major focus of future studies designed to improve patient selection for aggressive antithrombotic therapy.
Conclusions
Antithrombotic therapy is a fundamental strategy in patients with NSTE-ACS; however, an optimal strategy that achieves a maximum anti-ischaemic effect associated with an acceptable bleeding risk remains to be determined. Since patients with NSTE-ACS overall have a high risk of recurrent ischaemic events, the investigation of management strategies beyond a year is crucial. DAPT with aspirin and clopidogrel or ticagrelor is the standard of care in the medical management of patients with NSTE-ACS; however, optimal duration of therapy is controversial. Ticagrelor can be administered as a first-line P2Y12 inhibitor therapy in preference to clopidogrel in medically managed patients with NSTE-ACS due to its significant mortality benefits. Prasugrel is not recommended in medically managed patients with NSTE-ACS. The optimal aspirin dose (81 vs 325 mg) in the secondary prevention of patients after MI or with significant coronary stenosis will be studied in the Aspirin Dosing: A Patient-centric Trial Assessing Benefits and Long-term Effectiveness study (n=2000).
Commonly recommended anticoagulants in the medical management of patients with NSTE-ACS are UFH, LMWH and fondaparinux. Due to its favourable safety profile, fondaparinux is preferred over enoxaparin in patients treated with clopidogrel and aspirin, however, we have no significant clinical trial evidence to support fondaparinux on top of potent P2Y12 inhibitors. The role of new oral anticoagulants with better safety profile than warfarin in addition to DAPT in patients with ACS is being addressed in recent and ongoing trials. ATLAS trial results suggest a role for long-term inhibition of thrombin with rivaroxaban in patients with ACS in addition to antiplatelet therapy of clopidogrel and aspirin. Recently, rivaroxaban has been approved by the European agency for secondary prevention in patients with ACS. In the Study to Compare the Safety of Rivaroxaban vs Acetylsalicylic Acid in Addition to Either Clopidogrel or Ticagrelor Therapy in Participants With Acute Coronary Syndrome trial (NCT02293395), the benefits of the dual pathway strategy of rivaroxaban or aspirin in combination with a single antiplatelet agent (clopidogrel or ticagrelor) for long-term secondary prevention of additional CV events in patients with ACS is being evaluated (n=3000). Inhibition of the thrombin receptor may further attenuate ischaemic event occurrence and vorapaxar, a PAR-1 inhibitor may also be added to antiplatelet therapy in selected patients with ACS. The potential role of parenteral P2Y12 receptor blockade (cangrelor) and parenteral PAR-1 inhibition (PZ128) with fast onset and offset of effects in the medical management of NSTE-ACS is not known.40
Understanding the mechanisms of treatment failure and bleeding during antithrombotic therapy is a major area of ongoing investigation. However, specific cohort of patients with ACS eligible for treatment with fondaparinux, rivaroxaban or vorapaxar in addition to DAPT and the efficacy and safety of fondaparinux, rivaroxaban and vorapaxar in patients treated with potent P2Y12 inhibitors such as ticagrelor or prasugrel are unknown at this time. In this line, personalisation of antithrombotic treatment strategies based on algorithms employing demographic and clinical characteristics along with objective markers of thrombotic propensity may hold promise to achieve significant advances in achieving improved net clinical benefit in medically managed patients with NSTE-ACS.
Key messages
Patients presenting with non-ST-segment elevation acute coronary syndromes (NSTE-ACS) are at high risk for acute as well as long-term thrombotic events.
Thrombosis is a major underlying mechanism leading to the development of NSTE-ACS and subsequent adverse event occurrences.
Since platelet function and coagulation play pivotal roles in thrombus generation at the site of vessel wall injury, a combination of antiplatelet and anticoagulant agents (together known as antithrombotic therapy) is the cornerstone of treatment for patients with NSTE-ACS.
Dual antiplatelet therapy (DAPT) with aspirin and clopidogrel or ticagrelor and unfractionated heparin, low-molecular-weight heparins and fondaparinux are the standard of care in the medical management of patients with NSTE-ACS.
The role of new oral anticoagulants with improved safety profile in addition to DAPT in patients with ACS is being addressed in recent trials.
The efficacy and safety of fondaparinux, rivaroxaban and vorapaxar in patients treated with potent P2Y12 inhibitors such as ticagrelor or prasugrel are unknown at this time.
Inhibition of the thrombin receptor may further attenuate ischaemic event occurrence and vorapaxar—a protease activated receptor-1 inhibitor may also be added to antiplatelet therapy in selected patients with ACS in future.
Specific cohort of patients with ACS eligible for treatment with rivaroxaban or vorapaxar in addition to DAPT and the efficacy and safety of the latter agents in patients treated with ticagrelor or prasugrel are unknown at this time.
You can get CPD/CME credits for Education in Heart
Education in Heart articles are accredited by both the UK Royal College of Physicians (London) and the European Board for Accreditation in Cardiology—you need to answer the accompanying multiple choice questions (MCQs). To access the questions, click on BMJ Learning: Take this module on BMJ Learning from the content box at the top right and bottom left of the online article. For more information please go to: http://heart.bmj.com/misc/education.dtl
RCP credits: Log your activity in your CPD diary online (http://www.rcplondon.ac.uk/members/CPDdiary/index.asp)—pass mark is 80%.
EBAC credits: Print out and retain the BMJ Learning certificate once you have completed the MCQs—pass mark is 60%. EBAC/ EACCME Credits can now be converted to AMA PRA Category 1 CME Credits and are recognised by all National Accreditation Authorities in Europe (http://www.ebac-cme.org/newsite/?hit=men02).
Please note: The MCQs are hosted on BMJ Learning—the best available learning website for medical professionals from the BMJ Group. If prompted, subscribers must sign into Heart with their journal's username and password. All users must also complete a one-time registration on BMJ Learning and subsequently log in (with a BMJ Learning username and password) on every visit.
References
Footnotes
Contributors PAG and UST are involved in both designing and writing this manuscript.
Competing interests PAG reports serving as a consultant fees/receiving honoraria from Daiichi Sankyo, Bayer, AstraZeneca, Merck, Boehringer, New Haven Pharmaceuticals, Janssen and CSL; receiving grants from the National Institutes of Health, Daiichi Sankyo/Lilly, New Haven Pharmaceuticals, Harvard Clinical Research Institute, Bayer, Haemonetics, Duke Clinical Research Institute, Sinnowa and Coramed.
Provenance and peer review Commissioned; externally peer reviewed.