Hypertension and ethnic group
BMJ 2006; 332 doi: https://doi.org/10.1136/bmj.332.7545.833 (Published 06 April 2006) Cite this as: BMJ 2006;332:833
- Morris J Brown, professor (mjb14{at}cam.ac.uk)1
Are there ethnic differences in the pathogenesis of hypertension and are these sufficient to influence choice of treatment? I will also consider prevalence and complications. Because hypertension is the biggest and an almost entirely treatable cause of cardiovascular disease, even small ethnic differences in its optimum management have large implications for health resources. Ethnic differences in the type of hypertension give us the strongest evidence that we have for the concept that hypertension exists in two broad types. As for diabetes, hypertension can usefully be considered as of type 1 or type 2, each with its own preferred treatment. Results of recent trials support this view and emphasise the importance of choosing the right strategy for the type of hypertension to be treated.
Sources and selection criteria
Numerous published studies, including many reviews, compare one or more of the four parameters to be discussed in different ethnic groups. A few have prospectively identified similar numbers in the ethnic groups being compared or a minimum proportion of the ethnic minority. But most are retrospective analyses of studies in which a multi-ethnic population was recruited. I found relevant studies with Medline and Google-Scholar, searching for “hypertension” with either “ethnic” or the names of individual ethnic groups. White and black people are the key ethnic groups to have been compared. Some prevalence studies included Asians, but these studies give insufficient information on which to make reliable statements about pathogenesis or treatment.
Pathogenesis
Progress in understanding the pathogenesis of hypertension has been slow because essential hypertension is extremely complex at a molecular level.1 Conversely, hypertension exists in only two broad physiological types. This has been long predictable in theory from Poiseuille's law (that blood pressure is the product of vasoconstriction and volume) and supported in practice from the observation that a few of the syndromes where hypertension is due to a single identifiable factor (monogenic or secondary) are characterised either by increased vasoconstriction (for example, phaeochromocytoma) or increased volume (for example, primary hyperaldosteronism, Liddle's syndrome). More unexpectedly, the large choice of drugs for hypertension have turned out to resolve into just two groups that act, broadly, on either the vasoconstriction or volume components of hypertension.2 Laragh has called these two types of hypertension R (renin) and V (volume).w1 Type 1 and type 2 hypertension are more memorable alternatives, arising from an analogy with diabetes, in which the relative deficit or excess of insulin is largely related to age and race.3
Plasma renin and hypertension
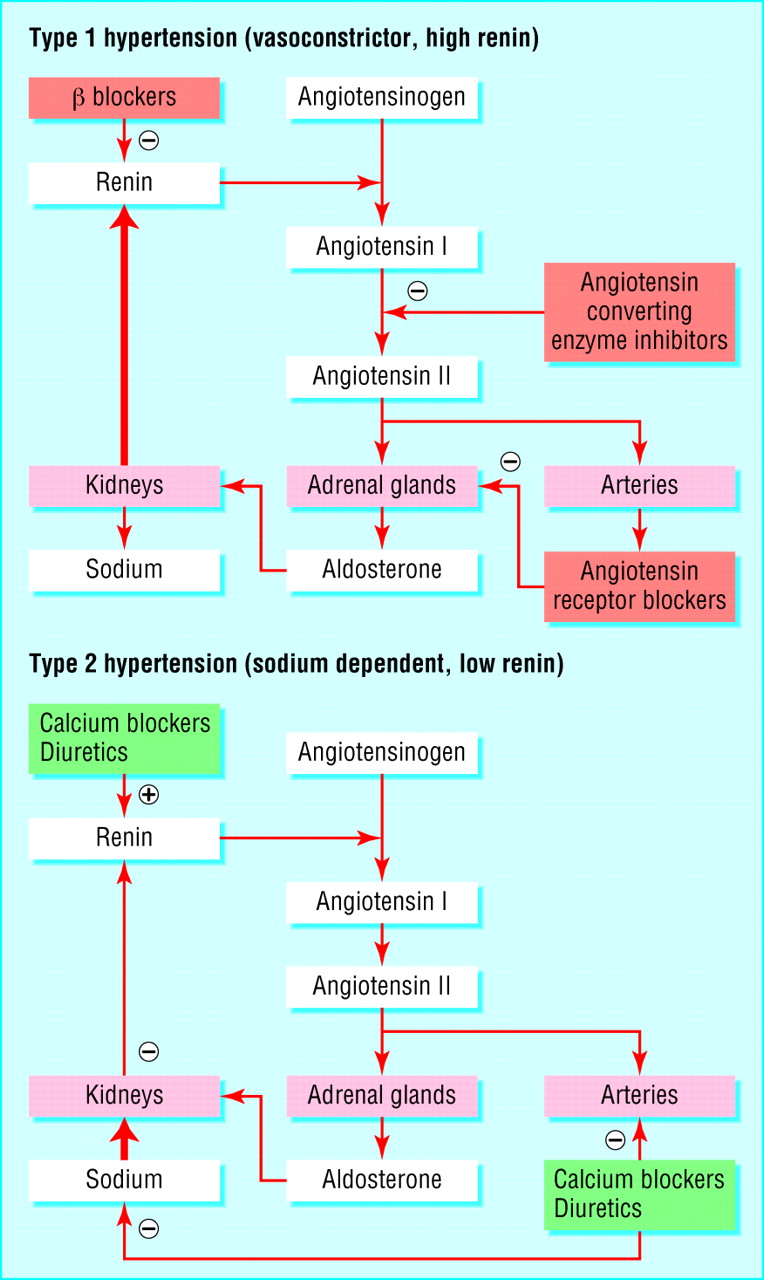
The two types of hypertension can be distinguished by measuring plasma renin (fig 1). Renin secretion is suppressed when the kidney detects that the amount of sodium ions reaching the sodium sensor (macula densa) in the nephron is raised. So a low plasma renin is an excellent clinical clue to the presence of excess sodium in the circulation. This standard physiological teaching receives strong clinical support from the typically suppressed plasma renin concentrations in syndromes like Conn's and Liddle's, in which excess sodium retention is due, respectively, to increased aldosterone secretion or response.

Two types of hypertension: the role of the renin-angiotensin system. Type 1: renin secretion inappropriately high for blood pressure and elimination of salt load is exaggerated. Common in young white people, responds better to AB drugs (angiotensin converting enzyme inhibitors, angiotensin blockers, and β blockers), which block the renin-angiotensin system. Type 2: renin secretion suppressed by kidney's detection at the macula densa of excessive sodium reabsorption. Commoner in young black people, responds better to CD drugs (calcium channel blockers and diuretics), which are natriuretic and vasodilating
{kind=link}
Conversely, plasma renin in the upper end of its range is not universally recognised as a marker of vasoconstrictor hypertension. But even if the renin and angiotensin are not the primary cause of vasoconstriction, they are secreted in response to the pressure induced natriuresis that any other vasoconstrictor induces.4w2 Renin concentrations also determine how far blood pressure falls on salt restriction.5
Using plasma renin, together with its predicted influence upon drug response, it is possible to determine whether the types differ in special situations and to examine the evidence for different preferred treatments. The attraction of examining these hypotheses in ethnic groups is that these are more discrete, and the definition less arbitrary, than groups like “old” or “young”. So far, however, in only black people have sufficient studies been done to permit certainty of a difference in type of hypertension and drug response.
Ethnic variation in renin
Black people tend to develop hypertension at an earlier age, and target organ damage differs from that in white people.w3 w4 The first study to compare the renin-angiotensin system in black and white hypertensive people was done in 1964 and reported that 30% of black people with hypertension had no detectable plasma renin activity. Renin was still suppressed after the stimulus of a low salt diet and treatment with diuretics. Most but not all subsequent studies have confirmed that renin activity is lower than in white people in both hypertensive and normotensive black people.6–9 w5 w6 Laragh and Buhler noted that younger patients responded better to βblockers, older to diuretics, and they linked this observation to the decline in plasma renin with age.10w7

An Englishman tastes the sweat of an African (Serge Daget, 1725). Is the captain assessing the prisoner's health or has he learnt that salty sweat presages reduced ability to withstand the voyage?
{kind=link}
The evolutionary driver to hypertension is likely the need to protect the circulation and therefore sodium. In most patients with low renin hypertension, the cause of the barrier to sodium excretion is uncertain. Nephron mass is lower in black than in white people.11 The fall in renin with age accompanies a similar reduction in nephron number.w8 The rare monogenic syndromes of hypertension can occur in both groups. However, black people with hypertension have a common threonine to methionine substitution, T594M, in the epithelial sodium ion channel, which is insufficient on its own to cause hypertension but is a significant contributory factor to the low renin hypertension of black UK citizens. This is, to date, the only clear example of a genetic variant contributing to hypertension in one race but not another.12 However, the public single nucleotide polymorphism (SNP) databases now contain thousands of ethnic specific SNPs, including many that direct a change in amino acid. It is a statistical certainty that some of these will be relevant to ethnic variation in disease.
The substantial difference in phenotype between the hypertension in black and white people tells us that pathogenesis is likely to differ fundamentally, and supports the search for genetic and pharmacogenetic variation in our attempts to understand hypertension at a molecular as well as physiological level. There has been considerable speculation that sodium retaining alleles are more likely to be selected in a hot, low salt environment, with the possibility of further selection created by the terrible conditions in the slave transports (fig 2).13 w9-w11 In such a genetic background, hypertension is more likely to ensue when it is transferred to an environment where salt is plentiful, and this is one possible explanation for the steep gradient in hypertension prevalence between black people in Africa, through the Caribbean to the United States.w12
Prevalence
Most studies in the United Kingdom and United States report a higher prevalence and lower awareness of hypertension in black than in white people. NHANES (the national health and nutrition examination survey) is a sample of the civilian US population. It includes a survey interview population of 7000 US adults aged 20 years and 5000 respondents who completed a health examination each year. Hypertension was defined as having an average systolic blood pressure of 140 mm Hg or diastolic blood pressure of 90 mm Hg or taking drugs for blood pressure. Table 1 compares prevalence, awareness, and control in black people with those in two groups of white people of different social status. Black people clearly have a higher prevalence than either group of white people; however, this recent series did not confirm previous reports of lower awareness and poorer control. The picture is similar in the UK. A recent review summarises 14 studies.14 w14 Data for other ethnic groups is more sparse, and shows some difference between children and adults (see bmj.com). The South London study of several ethnic groups, however, reported twice as much hypertension in black and Asian people (fig 3).15
Estimated non-institutionalised US adults with hypertension, by sex, ethnic group, and age, 1999-2002. Values are percentages (95% confidence intervals). (Adapted from Centers for Disease Control and Preventionw28)

Prevalence of hypertension, diabetes, and raised cholesterol by ethnic group relative to white people, adjusted for age and sex. Those for obesity and smoking are age adjusted in men (M) and women (W) separately. Bars show 95% confidence intervals (adapted from Cappuccio et al19)
{kind=link}
Complications
Older data for England and Wales showed that mortality from hypertension in African-Caribbean born people is 3.5 times the national rate; the excess in Caribbean born women is more than sixfold.16 w15 Similar data have been published for black US citizens.w16 More recently, these differences have been challenged.w17 w18 Strokes are commoner in black people, but coronary heart disease is commoner in Asians.17w19 Both groups have a higher incidence of chronic renal failure than white people, but this is more due to hypertension in black people, and to diabetes in Asians.w15 British Asians also have raised mortality from hypertension, with rates about 1.5 times national rates.w15 For echocardiography, a cohort study of 1500 US citizens has recently shown that the substantially large mass indices in black people is independent of their blood pressure.w20 An explanation is the smaller nocturnal dip in blood pressure, resulting in a higher average pressure over 24 hours.18w21
Treatment
Although we might have most to learn from the study of ethnic differences in pathogenesis of hypertension, it is the impact of this on choices of treatment that is thought to have greater practical importance. The difference in response pattern between black and white people is the best documented example and corresponds well with the difference in renin type described above. But overlap is sufficient, a recent meta-analysis to question the use of ethnic group to guide initial treatment found.20
If black people tend to have type 2 (low renin) hypertension, this predicts a better response to CD drugs (calcium blockers and diuretics) than to AB drugs (angiotensin converting enzyme inhibitors, angiotensin blockers, and calcium blockade). This is indeed broadly the picture. The clearest feature of hypertension in black people is that they have a poorer response to treatment with angiotensin converting enzyme (ACE) inhibitors compared to white people.21w22 w23 In ALLHAT, lisinopril was 4 mm Hg less effective than chlorthalidone in black people.22 The evidence for βblockers being less effective in black people is almost as clear cut.21w24 Diuretics, conversely, are more effective at a young age in black people, both because of the role of salt in causing their hypertension and because there is less compensatory increase in renin than in white people.23
The largest comparison of drug response by age and ethnic group is shown in fig 4. A decade later, we know from ALLHAT and INSIGHT that in patients likely, through age or ethnic group, to have low renin hypertension, diabetogenic doses of chlorthalidone or hydrochlorothiazide with amiloride are required to reveal equivalent reduction in blood pressure and cardiovascular endpoints as 10 mg of amlodipine or 60 mg of nifedipine.24

Response to single drug antihypertensives and placebo in men, by two ethnic and age groups. Numbers are sizes of each group. Arrows group drugs that had effects which did not differ significantly (adapted from Materson et al21)
{kind=link}
Two recent events show the present and future value of recognising two types of hypertension and their cognate drugs. One is the fairly radical recommendation by the National Institute for Health and Clinical Excellence that first line treatment for hypertension depends on age and ethnicity (www.nice.org.uk/page.aspx?o=292867). The second is a report from the MRC British genetics of hypertension study (BRIGHT) that indicates a substantial shared genetic component underlying the preference of type 2 patients for calcium blockade and diuretics. In a cohort of about 100 pairs of siblings who both had poor blood pressure control when treated with an AB drug, the BRIGHT team identified with a probability of more than 100 000:1 the presence of a gene in the same part of chromosome 2p as previously linked to hypertension in black US citizens.25 It is likely that some single nucleotide polymorphisms in this chromosomal region are commoner in black versus white people and in salt sensitive versus salt resistant hypertension.
Summary points
Pathogenesis, prevalence, complications, and treatment of hypertension depend on ethnic origin
Differences are less apparent than similarities; only black with white people can be reliably compared
Prevalence and complication rates vary only in degree, but pathogenesis differs fundamentally and affects choice of treatment
Young white and black people can be characterised as high and low renin hypertensives, corresponding to their better response to treatment with angiotensin converting enzyme inhibitors and β blockers or calcium channel blockers and diuretics
More study of other ethnic groups will show whether division of hypertension into high and low renin types can be generalised
Conclusions
Some readers may need no persuading that hypertension has two types. Until recently, however, the only hypertension guidelines recognising the need to tailor initial treatment according to type of hypertension was from the British Hypertension Society.w27
I have also covered known differences in risks and outcomes between ethnic groups. But here the similarities should be emphasised more than the differences. In all groups, the message of what matters is simple—“the blood pressure, stupid.” Differences in the responses of blood pressure to treatment have yet to be studied in most ethnic groups. These differences are important for patients and important for us in furthering our understanding of hypertension.
Footnotes
-
 References w1-w28 and additional text are on bmj.com.
References w1-w28 and additional text are on bmj.com. -
Contributors MJB is the sole contributor.
-
Competing interests MJB is president of the British Hypertension Society, which receives sponsorship from companies listed at www.bhsoc.org.
-
For more information visit the British Hypertension Society (www.bhsoc.org).