Article Text

Abstract
The myocardial interstitial or extracellular space exists as a complex and dynamic environment, vital for normal cardiac structure and function. The physiological pathways for normal control of collagen turnover, and the pathological development of fibrosis are beginning to be understood, as are their relationships to cardiac remodelling and adverse outcomes. Emerging non-invasive imaging techniques (echocardiography, cardiovascular magnetic resonance, positron emission tomography) may allow a clearer understanding and measurement of these processes in vivo. Preliminary results are exciting, spanning valvular and congenital heart disease, cardiomyopathy and rarer diseases such as amyloid. In this review, such developments and research directions are explored, including the rapid developments in cardiovascular magnetic resonance T1 mapping and its use with contrast to derive extracellular volume. The authors present a state-of-the-art assessment of the strengths and weaknesses of each modality, and distil a framework to equip the reader with an understanding of the technical issues useful for the interpretation of emerging clinical studies.
- Interstitial space
- extracellular space
- fibrosis
- cardiac imaging techniques
- cardiac function
- imaging and diagnostics
- MRI
- myocardial fibrosis
- myocardial ischaemia and infarction
- cardiomyopathy
- cardiac imaging
- hypertrophic cardiomyopathy
- myocardial infarction
Statistics from Altmetric.com
- Interstitial space
- extracellular space
- fibrosis
- cardiac imaging techniques
- cardiac function
- imaging and diagnostics
- MRI
- myocardial fibrosis
- myocardial ischaemia and infarction
- cardiomyopathy
- cardiac imaging
- hypertrophic cardiomyopathy
- myocardial infarction
Introduction
The cardiac interstitium provides a complex and dynamic environment vital for normal structure and function. In disease, one of the hallmarks of pathology is expansion of the interstitial space usually through the development of fibrosis. This is strongly associated with left ventricular remodelling and adverse outcomes such as heart failure, arrhythmia and death. The present gold standard for evaluation of the interstitial space is invasive endomyocardial biopsy. However, this not only carries potential morbidity and mortality, but its accuracy is confounded by sampling error and a lack of whole heart representation. Blood biomarkers for fibrosis assessment are also known to have complex confounding factors. Therefore, non-invasive imaging assessment of the interstitial space has the potential to provide an important ‘missing biomarker’ in cardiac disease. Such a tool, or toolset, would promise greater pathophysiological understanding, early disease detection, disease sub-typing and the potential for more individualised therapy. A variety of imaging techniques are evolving, with different modalities at different developmental stages in progression to clinical utility and some (such as cardiovascular magnetic resonance (CMR)) developing multiple variants on a theme.
The cardiac interstitial space in health and disease
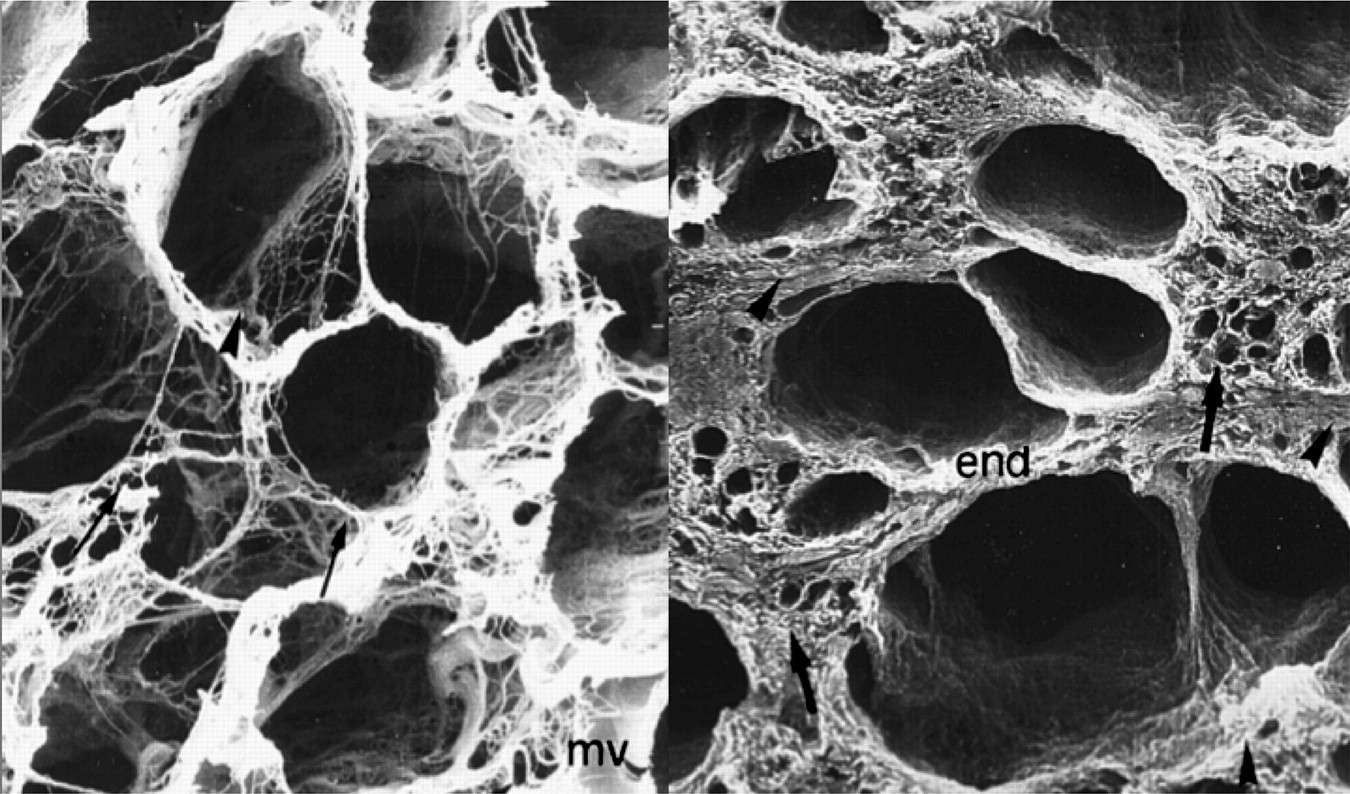
The interstitium is a complex three-dimensional space into which cardiac cells, blood vessels and nerves are embedded. In the normal human heart, the extracellular matrix (ECM) is predominantly made up of collagen scaffolding of types I (80%) and III (11%), seen in figure 1.1–3 The matrix contains a ground substance of proteoglycans and glycosaminoglycans, and among others fibroblasts and immune cells.4 A delicate interstitial ‘milieu’ exists, the interstitium being actively maintained by the relationships between itself, myocytes, the neuro-hormonal system, mechanical forces and cardiac fibroblasts.5 Fibroblasts are far more preponderant than might be expected, representing up to 60% of the total myocardial cell population in some species.6 They are also morphologically different to fibroblasts in other organs, and form an intricate syncytium throughout the ECM collagen, a synergistic structural support and communication network coupled together by gap junctions (mainly of connexins 43 and 45).7 Within theses coexisting matrices, a constant flux of tissue and collagen turnover— (growth and repair)—occurs, orchestrated by regulatory cytokines, growth factors, enzymes, hormones and direct cell-to-cell communication.8
In disease, mechanical stress, hormonal environment and inflammatory responses metaplase fibroblasts into myofibroblasts and heralds a change in the interstitial status quo.9 Intracellular myofibroblast smooth muscle actin increases10 and titin phosphorylation occurs.11 12 Cell:cell and cell:ECM connections alter with changes in connexin and desmin. An increase in collagen abundance results with relatively larger diameter higher-tensile type I collagen (in comparison with type III),13 and more fibre cross-linking. On a larger scale, the increased fibrosis occurs in different, partly disease specific patterns described as compact or ‘focal’ scars, perimyseal, perivascular, plexiform or patchy fibrosis.14 Combined changes alter myocardial properties, both of function (initially diastole) and conduction (zig-zag conduction, electrocardiogram fractionation).15 While early changes may be physiological in response to demand, further changes may transmit to morbidity and mortality through functional impairment and arrhythmia.
The control of fibrotic remodelling is beginning to be understood. When secreted, procollagens are cleaved from their N- and C- end terminals by proteinases (procollagen C proteinase) allowing collagen molecules to self-assemble into fibrils and then large fibres. A family of proteolytic enzymes, the matrix metalloproteinases, regulate degradation and are themselves regulated by their tissue inhibitors.16 Fibrils are strengthened by cross-links catalysed by lysyl oxidase (LOX), overexpressed in states of persistent myocardial injury, and may be influenced by advanced glycation end products at a transcriptional level, and possibly procollagen C proteinases themselves.17 Other matricellular proteins (such as secreted protein, acidic and rich in cysteine)18 and small leucine rich proteoglycans19 play a role in collagen fibre assembly. These complex pathways provide a rich source of potential therapeutic targets and may betray their activation states by the ratio and absolute levels of serum biomarkers for the different pathways.20 However, pathological processes of fibrosis described are not necessarily irreversible. In both animal models21 and humans,22 interstitial fibrosis can regress, with alterations in physical loading (detraining and afterload reduction; hypertension; aortic valve replacement in stenosis given sufficient time). Many current treatments, such as angiotensin-aldosterone blockade either specifically or indirectly target these pathways and novel therapies are in development.23–25
Non-invasive imaging and the interstitial space
Non-invasive imaging of the heart in clinical application mainly measures aspects of myocyte function or whole tissue composite. Targeting imaging to the interstitium promises sensitivity to processes otherwise missed, and new insights into disease. Interstitial imaging techniques can be considered by modality, (echocardiography, CMR, positron emission tomography (PET) as below), but also, conceptually, by the processes measured, for example, measuring mechanical properties of fibrosis (echocardiography tissue doppler, CMR tissue tagging); the relative size of the extracellular space (contrast CMR, non-targeted PET tracers); and specific molecular species in fibrosis (molecular imaging, particularly by PET). Whatever the modality, the stage such techniques have reached along a developmental pathway to clinical utility is important; a generic pathway is outlined in box 1.26 Currently all available techniques have some way to go before routine clinical use, but rapid progress is being made.
Framework of incremental steps required for development of imaging techniques to quantify interstitial change and diffuse myocardial fibrosis (adapted from Sado et al26)
Each step is harder to fulfil. No current test in development achieves more than six of these 15 steps—eight if abstracts are included—and many whole imaging modalities have never achieved the final step.
Technical development and theoretical basis of test.
Direct comparison (animal models and then human autopsy material).
Detection of changes in established disease compared with normal subjects.
Correlation with known cardiac markers of diffuse fibrosis (eg, diastolic function, left ventricular hypertrophy).
Correlation with known biomarkers of diffuse fibrosis (eg, blood biomarkers).
Demonstration of the test in more than one clinical scenario.
Demonstration of test sensitivity (early disease or with age).
Demonstration of the ability to track change (with time, after treatment).
Demonstration of predictive or prognostic value of the test.
Standardisation of the test (reproducibility, different equipment, in non-research settings, quality control, limitations of test).
Development of robust age/ethnic normal reference ranges.
Changes in biomarker remain tied to the disease after treatment.
Demonstration of the test as a surrogate trial endpoint.
Clinical use and regulatory approval of the test.
Proof test use improves clinical outcome.
Echocardiography
Routine echocardiographic parameters of ejection fraction and indexed atrial area provide a guide to heart function and filling pressures that are deranged in conditions associated with fibrosis. Endomyocardial biopsy studies have suggested an inverse relationship between collagen content and tissue doppler-derived parameters of diastolic and systolic tissue velocity27 and this may be specifically related to increased type 1 collagen and excess cross-linking by LOX in patients echocardiographically defined as heart failure with normal ejection fraction.28 More specifically, integrated backscatter (IBS), first developed in the 1980s, continues to mature and appears a more specific echocardiographic interstitial imaging technique. Increased collagen decreases tissue elasticity, changing the acoustic impedance of myocardial tissues and their reflectivity. Signal measurement reliability can be improved by employing pericardial backscatter as an internal control (figure 2).29 In small studies of a number of cardiac diseases (aortic stenosis,30 dilated cardiomyopathy,31 post-cardiac transplantation32), IBS has been validated against biopsy. It also appears to correlate with diastolic function in hypertrophic cardiomyopathy (HCM)33 and end-stage renal disease,34 and also with collagen biomarkers in hypertension.35 Although IBS is cheap and potentially widely available, it may be technically difficult with low reproducibility; excellent image quality is needed for optimal correlations with biopsy.36

Measurement of integrated backscatter (IBS) from an image in raw data format. Cyclic variation (CV) of IBS (top) may be assessed in any segment but is subject to anisotropy. Calibrated IBS (bottom), which compares reflectivity relative to a fixed reference, such as pericardium or blood pool, is a potential marker of fibrosis (reprinted with permission from Marwick TH, Schwaiger M. The future of cardiovascular imaging in the diagnosis and management of heart failure, part 1: tasks and tools. Circ Cardiovasc Imaging 2008;1:58–69).29
Cardiovascular magnetic resonance
CMR techniques are developing rapidly and are coded in table 1 into six groups. The first technique described uses the intrinsic signal (measured as the magnetic resonance parameters T1 and T2) of myocardium without a contrast agent to distinguish normal from abnormal myocardium. Rapid sequences providing T138 49 or T250 ‘maps’ in a single breath-hold are now routinely available. Differences in T1 can be detected in acute myocardial injury37 51 52 and global interstitial fibrosis—changes that may find clinical utility particularly when gadolinium contrast is contraindicated (estimated glomerular filtration rate <30, pregnancy). A problem with these techniques is that they measure a composite myocardial signal from both interstitium and myocytes. The use of an extrinsic contrast agent adds another dimension to CMR tissue characterisation. The interstitial space can be assessed directly using standard gadolinium chelates. These low-molecular weight, purely extracellular agents are small enough to pass across the vascular wall into the extracellular space, yet are large enough not to be able to penetrate cells with intact membranes. They accumulate passively in the gaps between cells through post-bolus tracer kinetics and the increased volume of distribution of interstitial expansion in ‘scar’ tissue.42 This forms the basis of the late gadolinium enhancement (LGE) technique for detection of focal fibrosis such as seen in myocardial infarction. Recent developments have built upon this and allow scrutiny of diffuse interstitial expansion.
Contrast techniques for the non-invasive CMR assessment of the interstitial space and diffuse fibrosis
At a fixed time, after contrast administration, T1 may be reduced in cardiac disease suggesting increased myocardial interstitial space (table 1, technique 2).39–41 However, care is needed as the disease may have altered body composition (a higher percentage of body fat and, thus, a greater contrast dose per unit of total body extra-cellular water), reduced renal function, or altered haematocrit. If, instead, the ratio of signal change in blood and myocardium after contrast administration is calculated, the contrast partition coefficient is derived (table 1, technique 3).42 43 By then substituting in the blood contrast volume of distribution (equal to one minus the haematocrit) the myocardial contrast volume of distribution is obtained—a fundamental property—reflecting the fraction of the tissue which is interstitial space, also referred to as the myocardial extracellular volume fraction (ECV or ECVF). The three most advanced techniques (4a–c) are based on this principle. Each of these techniques has a different method to resolve the confounding effects of kinetics. First, in technique 4a, contrast kinetics are assumed irrelevant after sufficient time has elapsed—that a pseudo or dynamic equilibrium occurs at, for example, 15 or 20 min post-contrast.44–46 Second (technique 4b), kinetics are deconvoluted through mathematical modelling.47 Third (technique 4c), contrast delivery is manipulated by using a primed contrast infusion to achieve an equilibrium (EQ-CMR)48 and thus definitively removes kinetic effects (figure 3A,B)—a technique validated against histological collagen volume fraction in two diseases. There are a number of other considerations. The actual T1 measurement sequence is important, particularly in terms of heart rate sensitivity. The risk is that as the heart rate increases (and—it may do so in disease)—many T1 measurement techniques measure falsely low T1 values unless perfectly corrected. This may suggest erroneous interstitial expansion, an effect at least partly cancelled out in the volume of distribution calculation techniques. In our practice, we recommend using blood T1 measurement as a simple control for this effect. Newer T1 mapping sequences may be more robust in measuring T1 values, and also clinically applicable, offering whole heart quantification (Modified Look-Locker Inversion recovery (MOLLI) and Shortened MOLLI (ShMOLLI)). Although to date the MOLLI sequence has been more widely applied in experimental studies, there is now early histological validation for use of the ShMOLLI sequence post-contrast.53

Apical hypertrophic cardiomyopathy. (A) Diastolic still of cine image; (B) Late gadolinium enhancement image showing anterior wall scar. (C, D) T1 maps using ShMOLLI; pre-(C) and post-contrast (D) showing marked T1 shortening, particularly in the scar area. (E) The two T1 maps are combined with 1-haematocrit blood correction to create an extracellular volume (ECV) map.46 Note the elevated ECV fraction in the scar area.
A limitation of all extracellular contrast techniques to measure the interstitium is that they essentially measure the relative size of the extracellular space. All techniques will miss qualitative interstitial fibrosis parameter changes (such as collagen type I:III ratio and cross-linking). Likewise, interstitial expansion may represent many other processes than just collagen, for example, such as oedema in myocarditis, or infiltration with amyloid protein.
Positron emission tomography
The fraction of myocardium that is perfusable by water or perfusable tissue index can be assessed by PET scanning using H215O and C15O tracers. As fibrotic myocardium is unable to exchange water rapidly, a reduction should correlate with fibrosis. Although not validated against biopsy, perfusable tissue index is reduced in patients with advanced dilated cardiomyopathy, correlates with reduced function,54 and is also reduced in myocardial infarction.55 Although CMR and SPECT have potential, PET sensitivity has thus far provided the primary platform for molecular imaging, which specifically targets biological processes at the molecular or cellular level with high affinity tracers.56 For example, molecular targets include both the interstitial components (figure 4)57 and parts of the control pathways (eg, myocardial adrenergic receptors or pre-synaptic norepinephrine).58 In the pre-clinical arena, tracers for matrix metalloproteinases have the potential to be useful in fibrosis evaluation.59 In animal studies, Technetium-99m-labelled Cy5.5-RGD binds to myofibroblasts and correlates with new collagen deposition in myocardial infarction.60

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Multimodality imaging of angiogenesis 2 weeks post-acute infarction. Cardiovascular magnetic resonance images with late gadolinium enhancement (A,D) and hybrid positron emission tomography or CT perfusion with 13N-ammonia (B,E) together confirm extensive transmural anteroapical infarction. Positron emission tomography (C,F) following injection of a novel 18F-labelled probe targeting integrin shows infarct zone uptake (reprinted with permission from Makowski MR, Ebersberger U, Nekolla S, et al. In vivo molecular imaging of angiogenesis, targeting alphavbeta3 integrin expression, in a patient after acute myocardial infarction. Eur Heart J 2008;29:2201).57
Clinical relevance of interstitial imaging
The non-invasive assessment of interstitial expansion may find a variety of clinical uses. Fibrosis may be an early phenomenon in some diseases.61 In established disease, fibrosis-modulating therapies (eg, the renin-angiotensin antagonists and spironolactone) are established in heart failure but have not been well explored in other conditions such as cardiomyopathy and congenital heart disease. Interstitial measurement may sub-type diseases such as hypertension or HCM to permit individualisation of treatment through targeted anti-fibrotic therapy and improve clinical trials by defining populations for study. Fibrosis may also be linked to arrhythmia outcomes raising the possibility of using its measurement to target device therapy. The direction of travel is indicated in some key diseases outlined below; however, much of the data currently exists in preliminary or abstract form.
Afterload states (aortic stenosis and hypertension)
The burden of myocardial fibrosis in severe aortic stenosis has a negative impact on postoperative outcome,62 63 and so a method of preoperative quantification is important. Parameters of IBS have been shown to correlate with histology and with improvement in postoperative ejection fraction.30 64 Histological validation of the EQ-CMR technique also exists.48 The range of fibrosis on biopsy in these patients was wide ranging; from 6% to 40% of total myocardium. Biopsy permitted non-invasive results to be expressed as per cent diffuse myocardial fibrosis rather than the more abstract term ‘volume of distribution’. In this study, per cent diffuse myocardial fibrosis was shown to be a key predictor of exercise capacity in severe aortic stenosis. Relative proportions of interstitium and cell volumes were tracked over time, and the left ventricular hypertrophy regression following aortic valve replacement at 6 months was shown to be cellular rather than fibrosis regression.65 Since the original histological validation of IBS in patients with hypertension,66 well-crafted biopsy and biomarker studies67 have provided evidence for the role of fibrotic remodelling in hypertensive heart disease.68 More importantly, these studies support a role for therapies focused on fibro-modulation. For example, the ACE-inhibitor lisinopril69 and Angiotensin II receptor antagonist losartan68 have been shown to reduce biopsy-quantified myocardial fibrosis while improving diastolic dysfunction and left ventricle wall stiffness, respectively, changes that were independent of blood pressure lowering or left ventricle mass reduction. Other agents (eg, amlodipine70 and furosemide71) did not show this same effect. Less familiar agents such as the diuretic torasemide may provide additional antifibrotic effect by acting on the LOX pathway.71
Cardiomyopathy: hypertrophic and dilated cardiomyopathy
Limited early histological validation of CMR techniques exist in HCM, despite myectomy samples showing a more patchy distribution of fibrosis.48 In dilated cardiomyopathy, preliminary results from several small studies indicate interstitial expansion and, therefore, diffuse myocardial fibrosis, is correlated with ejection fraction, and indexed left atrial area.41 72 Work is ongoing in this area.
Diabetes
The presence of focal fibrosis on CMR scar imaging (LGE), has been shown to be an independent predictor of adverse cardiac outcomes,73 but may at least partly reflect correlation of diabetes with coronary artery disease. Diffuse fibrosis may be a more specific marker of diabetic matricellular effects and its detection in early disease may permit targeted therapy to obviate progression to heart failure. Initial studies are not definitive in early disease. IBS has been shown to be worse in diabetes over and above that of left ventricular hypertrophy.74 In the field of CMR, only the most potentially confounded of the contrast T1 mapping techniques to derive extracellular volume has been used to date (technique 2, table 1—post-contrast T1 values).40 A concern is that lower T1 values in worse disease may simply reflect increased adiposity in such patients (and consequent proportional contrast overdosing per unit of total body extra-cellular water).
Amyloid
Cardiac involvement is a leading cause of morbidity and mortality in systemic amyloidosis. The extracellular deposition of amyloid fibrils can be massive—the amyloid can be the majority of the heart—marked enough to change intrinsic magnetic resonance (pre-contrast) T1/T2 signal.75 The characteristic CMR appearance of global, subendocardial LGE reflects the altered contrast kinetics caused by significant interstitial expansion, and correlates with prognosis.76 Recently, our group has demonstrated that this interstitial expansion is higher than in any other measured disease outside of the infarct zone in myocardial infarction.77 Accurate and reproducible measurements will prove useful in serial quantification of cardiac amyloid burden for monitoring new treatments, and possibly for the detection of early cardiac involvement.
Congenital heart disease
Traditional management of congenital heart disease has focused on correcting deleterious haemodynamics to slow down, or prevent progression to heart failure. There has been less emphasis on myocardial protection, unlike conventional heart failure, and only few trials exist.78 Scar imaged by CMR first confirmed the presence of gross replacement fibrosis and linked it to adverse disease markers.79 More recently, interstitial expansion, expressed as a ‘fibrosis index’, has been demonstrated in a wide range of congenital heart diseases, which correlated with end-diastolic volume index and ventricular ejection fraction.80 It may be that these changes are additive to haemodynamics and focal scar in explaining outcome.
Acute myocardial injury: myocarditis and myocardial infarction
Acute myocardial injury is accompanied by intracellular and interstitial oedema and is traditionally detected in composite by increased T2 signal, although pre-contrast T1 mapping may prove to be equally effective and robust.52 Early gadolinium enhancement techniques confirm, and are more specific for the interstitial space expansion which occurs in addition to the capillary leakage and hyperaemia. In more severe cases, cellular necrosis and subsequent fibrosis are delineated by LGE, again confirming expansion, but also hypoperfusion. A differential in expansion, or ECV, has been demonstrated between the salvaged area at risk, the infarct zone and the remote myocardium in acute myocardial infarction.81 In the longer term, a negative correlation is seen between increasing ECV of remote myocardium and lower ejection fraction.46 In myocarditis, the focal changes seen play a key diagnostic role.82 Contrast T1 mapping techniques for quantifying diffuse interstitial expansion in myocarditis have yet to be explored, and may help stratify risk in this important area.83
Conclusion
The cardiac interstitium plays a central role in health and disease. The complex cellular and interstitial processes linked to adverse outcomes and mortality are beginning to be unravelled and therapeutically targeted. Non-invasive imaging is able to quantify interstitial expansion by fibrosis or amyloid in the clinical arena. Molecular techniques provide more specific detail on the underlying processes in animal models and offer the potential for clinical utility. CMR T1 mapping and its use with contrast to derive extracellular volume has begun to offer insights into early disease but, as with any developing field, competing techniques exist with different pros and cons. The future of non-invasive imaging of the interstitial space lies in collaboration between basic science and clinical practice in order to better understand the complex pathophysiology, and realise its potential as a key missing biomarker in cardiac disease.
References
Footnotes
Funding ASF, DMS and SKW each hold a clinical research training fellowship from the British Heart Foundation. JCM is supported by the Higher Education Funding Council for England. This work was undertaken at the University College London Hospital and University College London, which received a proportion of funding from the Department of Health's National Institute for Health Research Biomedical Research Centres funding scheme.
Competing interests JCM with UCL business and in collaboration with Resonance Health Ltd have submitted a patent on EQ-CMR.
Provenance and peer review Commissioned; externally peer reviewed.