Article Text

Abstract
Objective: To compare head to head the indices of left ventricular contractile reserve assessed by high-dose dobutamine in the five-year prognosis of patients with idiopathic dilated cardiomyopathy.
Design and setting: Prospective study in a tertiary care centre.
Patients: 63 consecutive patients with idiopathic dilated cardiomyopathy.
Interventions: High-dose dobutamine stress echocardiography was performed in progressive stages lasting 5 min each. Wall motion score index, ejection fraction, cardiac power output and end systolic pressure to volume ratio were evaluated as indices of left ventricular contractility.
Main outcome measure: Five-year cardiac mortality.
Results: During the follow up of 59 patients, 27 (45.8%) died of cardiac causes. According to Kaplan–Meier and receiver operating characteristic analyses all indices of contractile reserve differentiated patients with respect to cardiac death. Wall motion score index achieved the best separation (log rank 21.75, p < 0.0001, area under the curve 0.84), followed by change in ejection fraction (log rank 11.25, p = 0.0008, area under the curve 0.79), end systolic pressure to volume ratio (log rank 14.32, p = 0.0002, area under the curve 0.75) and cardiac power output (log rank 9.84, p = 0.0017, area under the curve 0.71). Cox’s regression model identified wall motion score index as the only independent predictor of cardiac death.
Conclusions: These data show that all examined indices of left ventricular contractile reserve are predictive of five-year prognosis, but change in wall motion score index may have the greatest prognostic potential.
Statistics from Altmetric.com
Dobutamine stress echocardiography is an established modality for the assessment of patients with dilated cardiomyopathy of ischaemic origin.1,2 The direct assessment of left ventricular contractile reserve during dobutamine stress echocardiography may improve the prognostic evaluation of patients with heart failure due to dilated cardiomyopathy,3,4 as well as predicting response to treatment with β blockers.5 As there is no consensus on the definition of contractile reserve indices, in various studies they have been defined differently,6,7 making direct comparison of their prognostic values difficult. Moreover, different studies used different means of pharmacological and exercise stress and enrolled patients with heart failure of both ischaemic and idiopathic origin, which may further complicate attempts at comparison.8,9 We have shown recently that various indices of contractile reserve are strongly, but differently, related to interstitial fibrosis and myocyte diameter,10 but it is not clear how this finding will translate to five-year prognosis.
Having these issues in mind, we undertook the present study to make a head-to-head comparison of various indices of left ventricular contractile reserve assessed by high-dose dobutamine in the five-year prognosis of patients with idiopathic dilated cardiomyopathy.
METHODS
Study patients
The study group comprised 63 consecutive patients (55 men, mean age 50.1 (SD 9.6) years) with idiopathic dilated cardiomyopathy who met the following criteria: (1) left ventricular end diastolic diameter ⩾ 60 mm; (2) ejection fraction ⩽ 35%; and (3) adequate echocardiographic window (defined as visualisation of at least 13 of 16 segments of the left ventricle). All patients underwent coronary angiography and right-heart catheterisation. Diagnosis of idiopathic dilated cardiomyopathy was established by echocardiography if there was no evidence of alcohol intake, arterial hypertension, toxin exposure, myocarditis, hypertrophic cardiomyopathy, valvular heart disease or significant coronary artery disease (defined as ⩾ 50% diameter stenosis of the major epicardial vessel). The study protocol was approved by the Dedinje Cardiovascular Institute Ethical Committee, and the investigation conforms with the principles outlined in the Declaration of Helsinki.
On admission, seven patients (11%) were in New York Heart Association class (NYHA) I, 37 patients (59%) were in class II, 17 patients (27%) were in class III and two patients (3%) were in class IV heart failure. The patients received the following drugs: digoxin, 25 of 63 (40%); angiotensin-converting enzyme inhibitors, 60 of 63 (95%); diuretics, 56 of 63 (89%); and β blockers (carvedilol) 55 of 63 (87%). They were followed up for five years after enrolment for cardiac death. Follow-up data were collected by a structured telephone interview with either the patient or the relatives of the patients, conducted in prespecified (yearly) time intervals. This was done by the first author, who is an experienced cardiologist.
Echocardiography
All examinations were performed with a Hewlett Packard Sonos 2500 machine (Andover, Massachusetts, USA) equipped with a 2.5 MHz transducer and stored on videotape for later analysis. Left ventricular diameters, ejection fraction and cardiac output were calculated according to the recommendations of the American Society of Echocardiography.11
Dobutamine stress echocardiography
Dobutamine stress echocardiography was performed in all patients in incremental stages lasting 5 min each, with an initial dose of 5 μg/kg/min, which was increased to 10 μg/kg/min, then to 20 and 30 μg/kg/min, and finally to the maximum dose of 40 μg/kg/min. The infusion was discontinued before the maximum dose if 85% of the maximum predicted heart rate for age group was achieved or a symptomatic non-sustained or sustained ventricular tachycardia was observed. β blockers were stopped 48 h before dobutamine testing in all patients taking these agents.
Contractile reserve
Wall motion score index, ejection fraction, cardiac power output and end systolic pressure to volume ratio were evaluated as indices of left ventricular contractility. Contractile reserve was defined as the difference between the values of these indices obtained at peak dobutamine dose during the test and the baseline values.
Wall motion score index
Left ventricular wall motion score index was calculated by using a 16-segment model of the left ventricle.11
Ejection fraction
Ejection fraction was determined by Simpson’s biplane formula. The cut-off point to identify patients with preserved contractile reserve (dobutamine-induced increase in ejection fraction ⩾ 6%) was calculated by receiver operating characteristic curves.
Cardiac power output
Mean arterial pressure, in mm Hg, was calculated in a standard manner: mean arterial pressure = (systolic blood pressure + 2 × diastolic blood pressure)/3.
Cardiac power output, in Watts, was then computed by the following equation: cardiac power output = (cardiac output × mean arterial pressure) × 2.22 × 10−3, where 2.22 × 10−3 is the conversion factor.12
End systolic pressure to volume ratio
As mean arterial pressure has been shown to underestimate end systolic pressure, we calculated end systolic pressure, in mm Hg, by using the previously validated equation13 end systolic pressure = 1.32 × mean arterial pressure − 22.6 mm Hg.
End systolic pressure to volume ratio was then computed as the ratio between end systolic pressure and the end systolic volume index.
Statistical analysis
All data are expressed as mean (SD). The t test was used to compare the subgroups for continuous variables (a value of p < 0.05 was considered significant). Kaplan–Meier curves were constructed to assess cardiovascular event-free survival during the five-year follow up. Receiver operating characteristic curves were computed to determine cut-off points for the dobutamine-induced change in the examined indices of left ventricular contractility and to calculate area under the curve for each index to determine its prognostic significance. After initial univariate Cox proportional hazards regression analysis to identify univariate predictors of future cardiovascular events, we proceeded with a forward stepwise multivariate Cox model, with the p levels for the entry into and removal from the model set at 0.05 and 0.1, respectively.
RESULTS
Study patients
Table 1 shows baseline demographic, clinical, haemodynamic and echocardiographic characteristics of enrolled patients. Briefly, patients were predominantly middle aged men with moderate to severe reduction of left ventricular contractility. Somewhat less than one third of them had advanced symptomatic heart failure judged as NYHA class III or IV.
Baseline demographic, clinical and haemodynamic data (n = 63)
Dobutamine stress echocardiography
The maximum given dose of dobutamine averaged 38.6 (4.3) μg/kg/min. Heart rate at peak-dose dobutamine was 118 (24) beats/min, and systolic and diastolic arterial pressures were 131 (24) and 84 (14) mm Hg, respectively. Resting and peak dobutamine heart rate did not differ between survivors and non-survivors (82.47 (15.68) v 89.81 (17.07), p = 0.09; and 116.09 (21.23) v 118.81 (27), p = 0.67, respectively). Additionally, the difference between peak dobutamine and resting heart rate was similar between the groups (33.63 (15.60) v 29 (17.50), p = 0.29). Extrasystoles were noted in 56 of 63 (88.9%) patients, couplets in 20 (31.7%) and a non-sustained ventricular tachycardia in 6 (9.5%). The longest run of ventricular tachycardia had eight complexes in a row and it did not cause haemodynamic compromise. Nausea and dizziness were noted in 9 of 63 (14.3%) patients. No test was stopped due to complications or side effects.
Receiver operating characteristics curves identified dobutamine-induced changes in wall motion score index ⩾ 0.19, ejection fraction ⩾ 6%, cardiac power output ⩾ 0.44 W and end systolic pressure to volume ratio ⩾ 0.33 as the best cut-off points to distinguish patients with favourable and poor five-year prognosis.
Follow up and contractile reserve
Data for five-year follow up were available for 59 of 63 (93.6%) patients. During the follow up, 27 of 59 (45.8%) patients died of cardiac and 2 (3.4%) of non-cardiac causes.
Patients who did not die of cardiac causes had higher contractile reserve measured by all indices (table 2).
Contractile reserve with respect to cardiac mortality during five-year follow up
Kaplan–Meier curves (fig 1A–D) show that all indices of contractile reserve distinguished patients well with respect to cardiac mortality during the follow up. The distinction was the best, however, when change in wall motion score index was used (log rank 21.75, p < 0.0001), followed by change in end systolic pressure to volume ratio (log rank 14.32, p = 0.0002), ejection fraction (log rank 11.25, p = 0.0008), and cardiac power output (log rank 9.84, p = 0.0017). Similarly, when receiver operating characteristics curves were constructed and area under the curve was calculated for each index, the change in wall motion score index emerged again as the most potent prognostic variable (area under the curve 0.84) but followed by change in ejection fraction (area under the curve 0.79), and then by change in end systolic pressure to volume ratio (area under the curve 0.75) and cardiac power output (area under the curve 0.71) (fig 2). There was no difference between area under the curve for tested indices, except between change in ejection fraction and end systolic pressure to volume ratio (p = 0.037) and change in end systolic pressure to volume ratio and cardiac power output (p = 0.037). Additionally, there was a statistically marginal difference between dobutamine-induced change in wall motion score index and ejection fraction (p = 0.05).
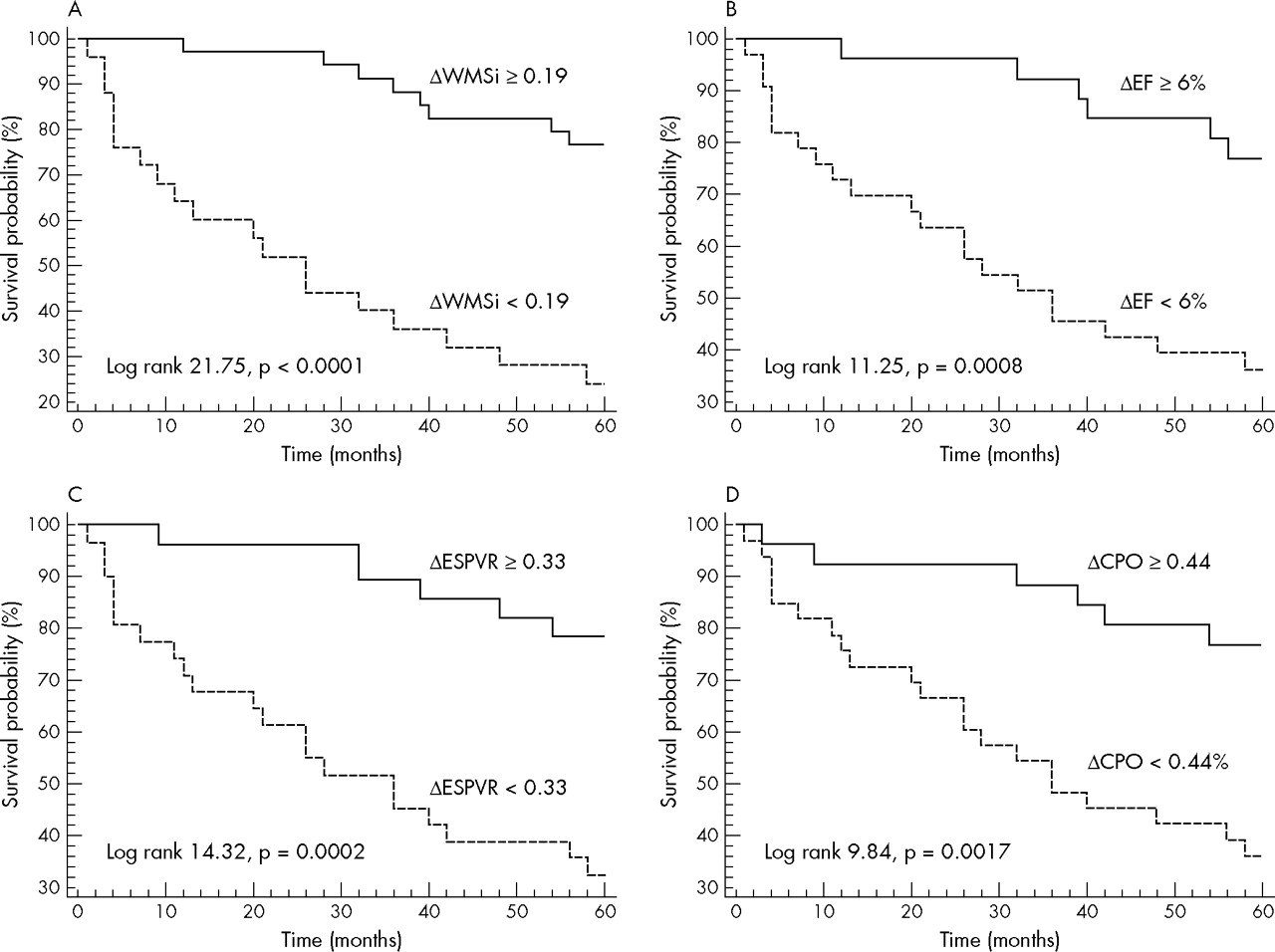
Kaplan–Meier curves for five-year survival free of cardiac death according to dobutamine-induced changes in (A) wall motion score index (WMSi), (B) ejection fraction (EF), (C) end systolic pressure to volume ratio (ESPVR) and (D) cardiac power output (CPO).
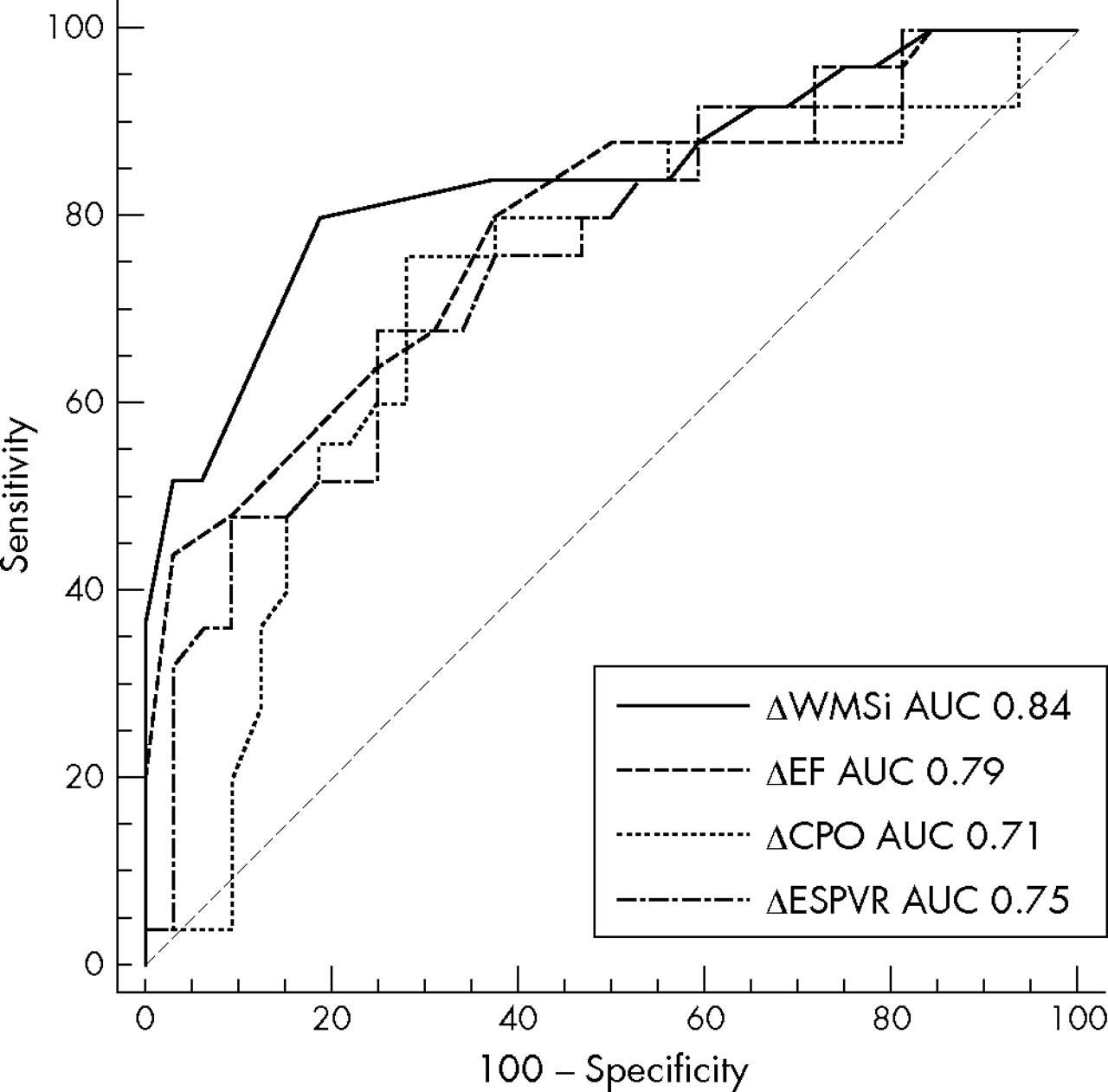
Receiver operating characteristic curves for five-year cardiac mortality for indices of left ventricular contractile reserve. Δ, dobutamine-induced change; AUC, area under the curve; CPO, cardiac power output; EF, ejection fraction; ESPVR, end systolic pressure to volume ratio; WMSi, wall motion score index.
In univariate analysis all indices of contractile reserve were predictive of cardiac death (table 3), but when they were entered into a multivariate Cox regression model only dobutamine-induced change in wall motion score index was identified as an independent predictor of cardiac mortality over the five-year period (table 3).
Univariate and multivariate Cox regression analysis of indices of left ventricular contractile reserve
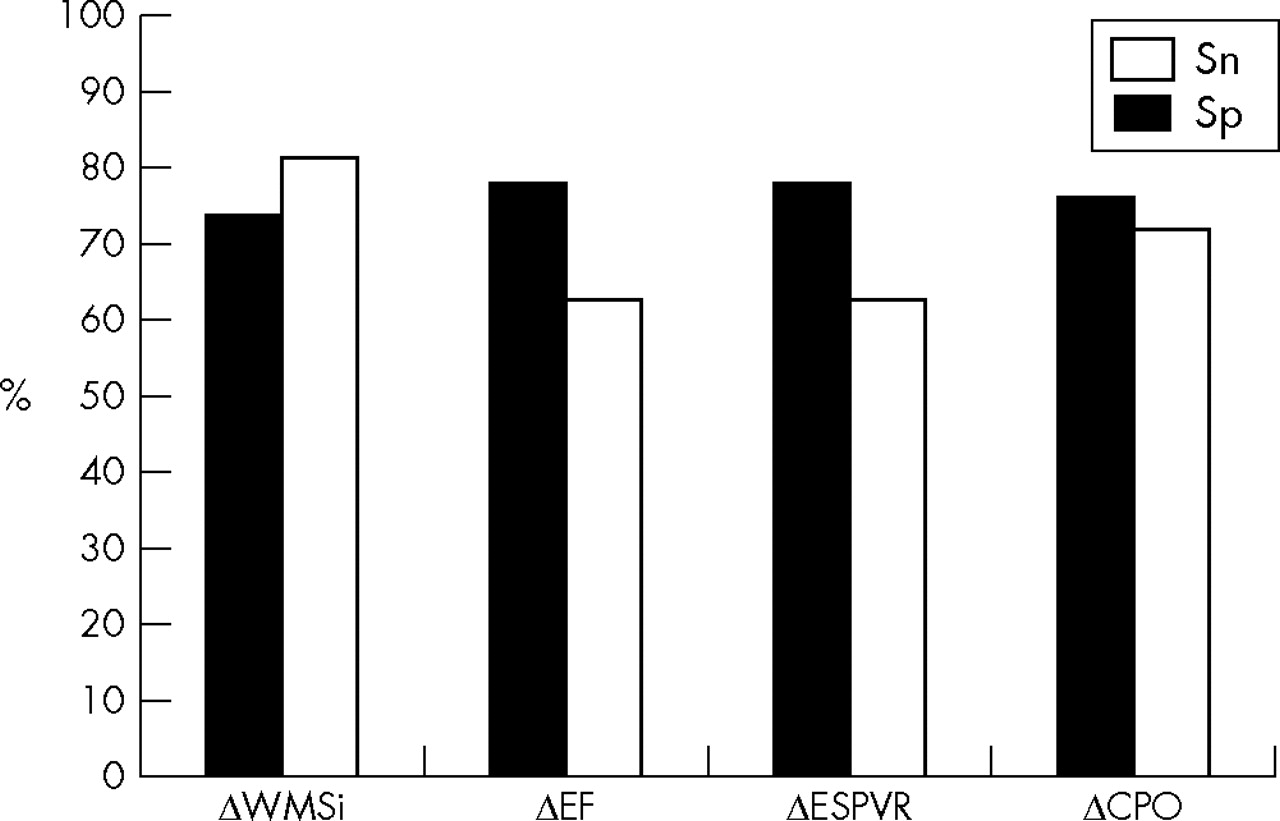
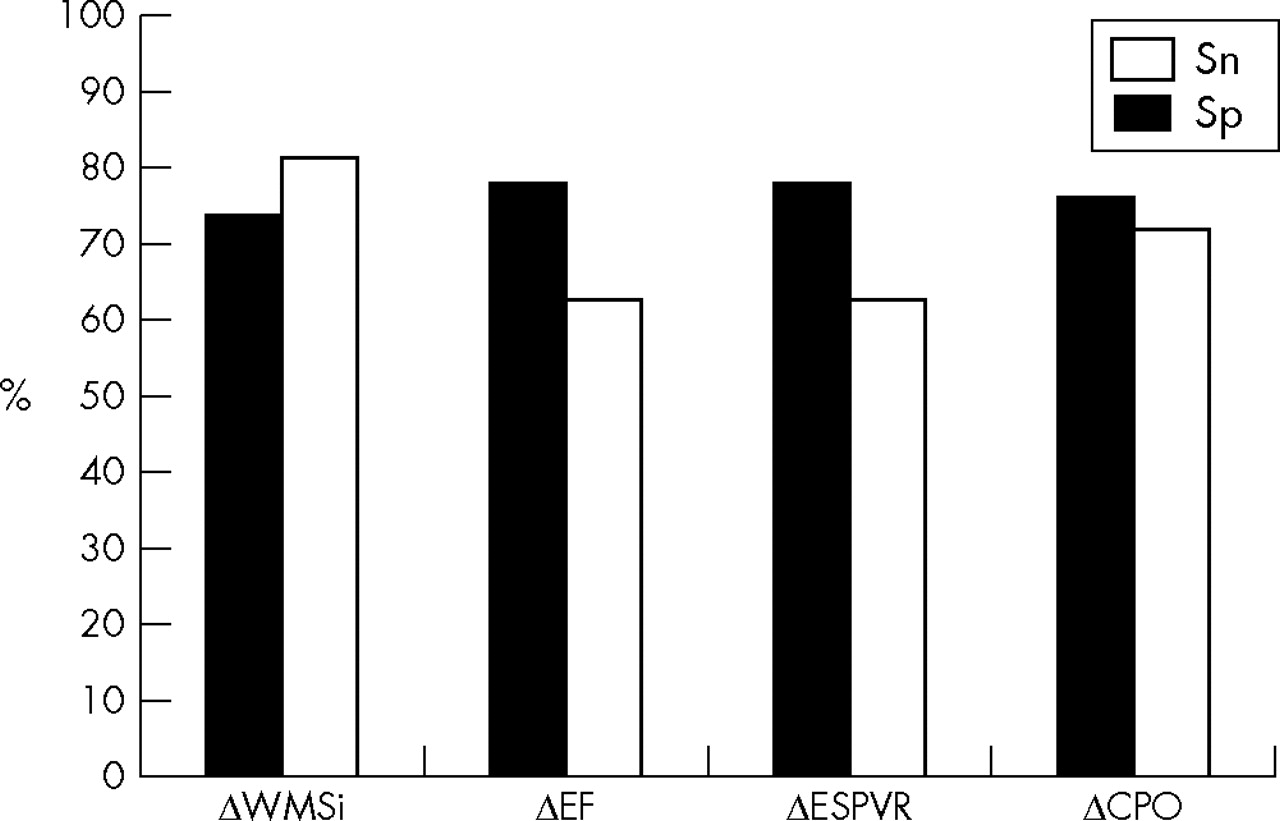
To assess prognostic impact of demographic and clinical variables, we tested some of these variables in univariate model (age, sex, NYHA class, symptom duration, presence of a third heart sound, pulmonary capillary wedge pressure and left ventricular end diastolic pressure). Of the tested variables, only age (β = −0.52, p = 0.04) and NYHA class (β = 1.46, p = 0.001) emerged as univariate predictors of five-year cardiac mortality and were entered into a multivariate model along with the indices of left ventricular contractile reserve. Multivariate analysis also identified the dobutamine-induced change in wall motion score index as the only independent predictor of long-term cardiac mortality. The change in wall motion score index had the highest specificity (81.2%) for cardiac mortality, whereas change in ejection fraction and end systolic pressure to volume ratio had the highest sensitivity (77.8%) (fig 3).
{kind=link}
{kind=link}
{kind=link}
Sensitivity (Sn) and specificity (Sp) for five-year cardiac mortality for indices of left ventricular contractile reserve. Δ, dobutamine-induced change; CPO, cardiac power output; EF, ejection fraction; ESPVR, end systolic pressure to volume ratio; WMSi, wall motion score index.
Interobserver and intraobserver variability
For two observers, the coefficients of variation for measurements of change in wall motion score index, ejection fraction, end systolic pressure to volume ratio and cardiac power output were 4%, 5%, 4%, and 7%, respectively. For one observer, these values for repeated measurements were 3%, 3%, 2%, and 5%, respectively.
DISCUSSION
This is the first study to make a direct comparison of prognostic significance of various indices of left ventricular contractile reserve obtained during high-dose dobutamine echocardiography. The main finding of the study is that a dobutamine-induced change in wall motion score index appears to be the most useful prognostic index during five-year follow up, which is in line with our previous findings that this index is closely related to the degree of myocardial histological disruption.10 A close link is therefore apparent between histological features, contractile reserve and long-term prognosis in patients with idiopathic dilated cardiomyopathy.
Dobutamine stress echocardiography
Patients with dilated cardiomyopathy have a decreased response to low-dose dobutamine, which is inversely related to left ventricular size and geometry.14 Low-dose dobutamine apparently does not recruit a full contractile response, especially in patients with severe heart failure, who have the most prominent β receptor downregulation.15
Contractile reserve
Several studies have investigated left ventricular contractile indices, but these studies are different with respect to the studied population, methods used to elicit left ventricular contractile response and indices of contractile reserve, all of which may preclude direct comparisons with our study.3–9
Wall motion score index
Clinical implications of contractile reserve defined by increased wall thickening (that is, a change in wall motion score index) have not been fully clarified with respect to patients with idiopathic dilated cardiomyopathy. A study by Naqvi and colleagues16 found that the dobutamine-induced change in wall motion score index predicts late spontaneous improvement in cardiac function in patients with recent-onset idiopathic dilated cardiomyopathy, but only secondarily to change in left ventricular ejection fraction and left ventricular sphericity index.16 On the other hand, we have shown that the magnitude of the dobutamine-induced change in wall motion score index has major prognostic implications for patients with idiopathic dilated cardiomyopathy.17 A recent study has elegantly shown a close correlation between regional coronary flow reserve and the corresponding contractile reserve, expressed as the dobutamine-induced change in wall motion score index, suggesting that microvascular dysfunction may have an important role in the course of idiopathic dilated cardiomyopathy.18
From the theoretical viewpoint, contractile reserve identified by the change in wall motion score index has several advantages, as it is easily applicable and does not require determination of invasive or complicated and time-consuming non-invasive indices. Furthermore, wall motion score index describes both regional and global changes in left ventricular contractility. This may be particularly important, as basal left ventricular contractility has been shown previously to have substantial regional heterogeneity, with the degree of the segmental metabolic defect being related to the wall motion abnormality on echocardiography.19
Receiver operating characteristics and Kaplan–Meier analysis, as well as the multivariate Cox regression model, have indicated that the dobutamine-induced change in wall motion score index was the most important prognostic factor for cardiac mortality during five-year follow up. This finding may be attributed to several reasons: firstly, wall motion score index is, within the physiological range, far less sensitive than other indices to changes in loading conditions; secondly, wall motion score index is easily calculated and, unlike cardiac power output and even ejection fraction, has good reproducibility; and thirdly, wall motion score index correlates most closely with myocardial morphology.
Ejection fraction
The usefulness of left ventricular ejection fraction in the assessment of contractile reserve has been a matter of debate. Ejection fraction is heavily dependant on loading conditions, which is especially true in patients with dilated cardiomyopathy, as loading conditions in these patients may be affected to various degrees by mitral regurgitation,20 compensatory neuroendocrine activation21 and enhanced interventricular dependence.22 Furthermore, dobutamine infusion has variable effects in patients with heart failure, as it may decrease afterload by 10% in patients with mild heart failure but increase afterload by 5% in patients with severe symptoms.14
Exercise-induced change of left ventricular ejection fraction, measured by radionuclide scintigraphy, has been shown to be the most powerful predictor of survival in patients with idiopathic dilated cardiomyopathy without overt heart failure.7 On the other hand, a dobutamine stress echocardiographic study of patients with more advanced symptoms due to the ischaemic form of the disease did not identify change of ejection fraction as an independent prognostic factor.3 Nevertheless, our data support the prognostic usefulness, but not primacy, of dobutamine-induced change in left ventricular ejection fraction, at least in patients with moderate to severe idiopathic dilated cardiomyopathy.
End systolic pressure to volume ratio
To our knowledge, end systolic pressure to volume ratio has not been used before to assess contractile reserve in patients with dilated cardiomyopathy, but its changes during exercise testing were used previously to assess patients after mitral valve replacement.23 The rationale of using the pressure to volume ratio is that it reflects left ventricular end systolic stiffness.24 The main drawback of this index is that it is sensitive to variations in afterload, especially in patients with large ventricular cavities25; however, it may be considered a valid measure of changes in left ventricular contractility when a purely inotropic drug is given. Our data show that the end systolic pressure to volume ratio can reliably identify patients with a worse prognosis over five-year period. Although this index has lower variability than other indices, its use in the clinical setting may be hampered by reluctance of physicians to use unfamiliar indices.
Cardiac power output
Cardiac power output reflects the combined pressure- and flow-generating capacities of the left ventricle.8 Cardiac power output has been shown, after preload optimisation, to reflect almost exclusively the contractile properties of the myocardium, as it is not afterload dependent.26 The usefulness of cardiac power output, however, whether mean or peak, in the assessment of patients with left ventricular dysfunction is somewhat controversial. Some studies have shown that this index is an independent predictor of survival,8 as well as a major determinant of exercise capacity,12 whereas others did not.9
In our study, among all the indices cardiac power output was the worse in predicting one-year prognosis. No other studies have directly compared cardiac power output with other indices of contractile reserve, except ejection fraction, and it may be hypothesised that other indices actually do have greater prognostic significance. Other potential explanations for this finding may be, firstly, the well-known limitations in the measurement of cardiac output based on the aortic velocity–time integral, which may present a significant source of error in the calculation of cardiac power output; and secondly, the crucial impact of mean arterial pressure on this index of contractility.
As all examined indices of left ventricular contractile reserve are predictive of long-term prognosis, the particular index can be chosen according to local expertise.
Limitations of the study
Although it seems reasonable to believe that all cardiac deaths were related to the principal condition (dilated cardiomyopathy), the possibility of other, unrecognised cardiac causes of death (such as new-onset coronary artery disease) cannot be completely excluded by the applied follow-up methods.
Conclusions
Our data show that all examined indices of left ventricular contractile reserve are predictive of five-year outcome and can identify patients with worse prognosis. The dobutamine-induced change in wall motion score index may, however, have the greatest prognostic potential with respect to patients with idiopathic dilated cardiomyopathy.
REFERENCES
Footnotes
-
Published Online First 31 January 2006