Article Text

Abstract
Background Despite an ageing Fontan population, data on late outcomes are still scarce. Reported outcome measures and determinants vary greatly between studies making comprehensive appraisal of mortality hazard challenging.
Methods We conducted a systematic review to evaluate causes and factors associated with late mortality in patients with Fontan circulation. Late mortality was defined as mortality beyond the first postoperative year. Studies were included if they had ≥90 patients or ≥20 late mortalities and/or transplants. Studies with overlapping patients were rationalised to include only the most recent studies to avoid duplication.
Results From 28 studies, a total of 6707 patients with an average follow-up time of 8.23±5.42 years was identified. There were 1000 deaths. Causes of late death were reported in 697 cases. The five most common causes were heart/Fontan failure (22%), arrhythmia (16%), respiratory failure (15%), renal disease (12%) and thrombosis/bleeding (10%). Factors associated with late mortality were evaluated and classified into 9 categories.
Conclusions Causes and factors associated with late mortality after the Fontan operation are summarised in this study. The presented information will aid in identifying patients at highest risk for mortality and guide our risk stratification efforts in this patient population.
Statistics from Altmetric.com
Introduction
The Fontan procedure has transformed the lives of patients born with single ventricle physiology and offered them the potential for survival and good quality of life well into adulthood.1 ,2 Since it was first performed in 1968, surgical techniques have evolved enormously2 as have the perioperative landscape including intensive care and cardiac catheter based interventions. As this patient population is ageing multiple morbidities are encountered which lead to premature death. Given the large number of patients with Fontan circulation reaching adulthood, we sought to systematically review and describe late mortality outcomes and its determinants in Fontan patients.
Methods
A systematic review of published studies that evaluated long-term mortality and/or heart transplantation in Fontan circulation was performed. Randomised, prospective and retrospective non-randomised studies were considered eligible for inclusion, provided that the study population included at least 90 patients with a Fontan circulation or at least 20 mortalities and/or transplants to maintain statistical power. We excluded studies that focused on short-term mortality within the 1st year of the Fontan procedure. We searched PubMed and the Cochrane Library for studies published in English with no restriction on date of publication. Search strategies for each database are presented in the online supplementary data. Two independent investigators conducted the search for studies initially, reaching agreement on the studies to be included by consensus among the entire group (figure 1). The risk of bias was assessed using the Cochrane risk of bias tool for randomised controlled trials3 and the modified Newcastle Ottawa scale for non-randomised studies.4 When more than one study included the same patients we excluded the studies with overlapping patients and we included only the most recent study that included these patients in the final analysis.
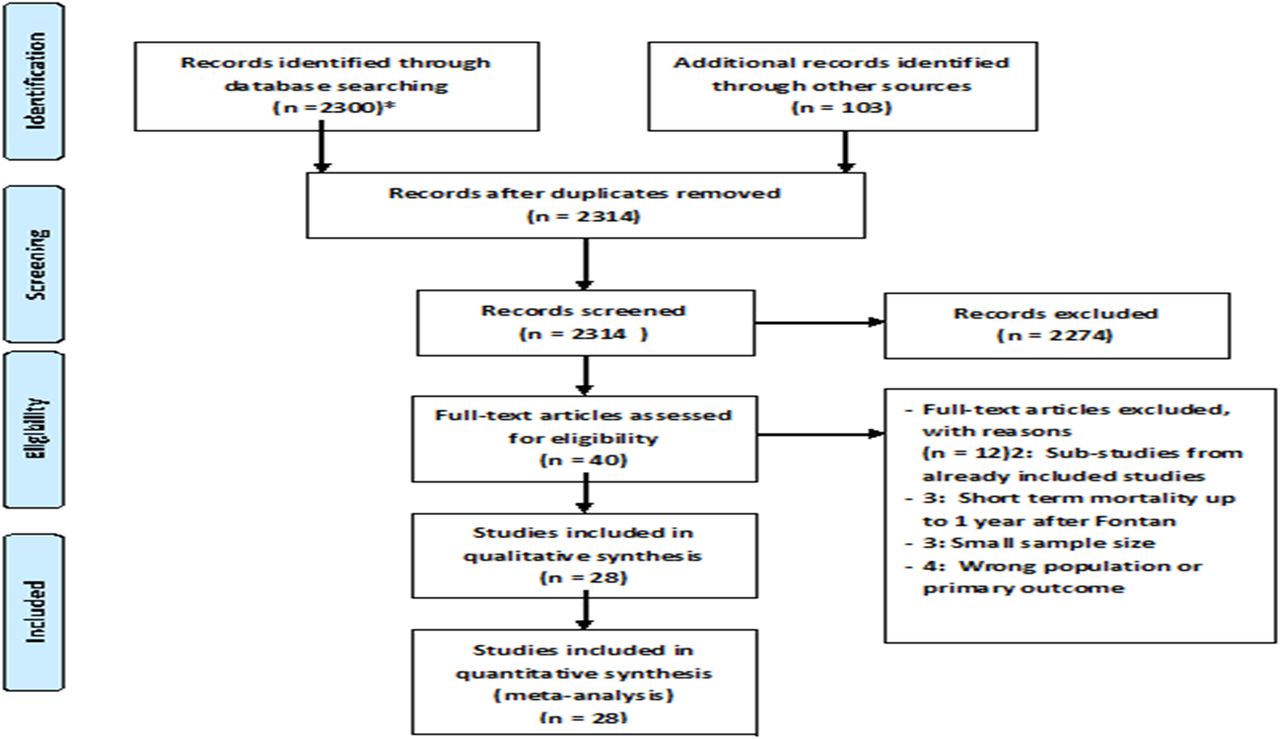
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram—study identification, selection and exclusions.
supplementary data
The factors associated with long-term mortality were divided into nine different categories as detailed in the results section. Each article was assigned to one or more category, depending on the mortality risk factors reported in the study. Each category of predictors was summarised by one or two researchers depending on their area of expertise and experience.
Results
Our search identified 28 studies eligible for inclusion (figure 1). These encompassed a total of 6707 patients with an average follow-up time of (8.23±5.42) years (table 1). Overall there were 1000 mortalities and 138 heart transplantations. The overall pooled mortality rate was 2.1% per year of follow-up. Additional characteristics are presented in online supplementary table S1.
Characteristics of included studies for mortality risk after Fontan procedure
supplementary table
Causes of long-term mortality
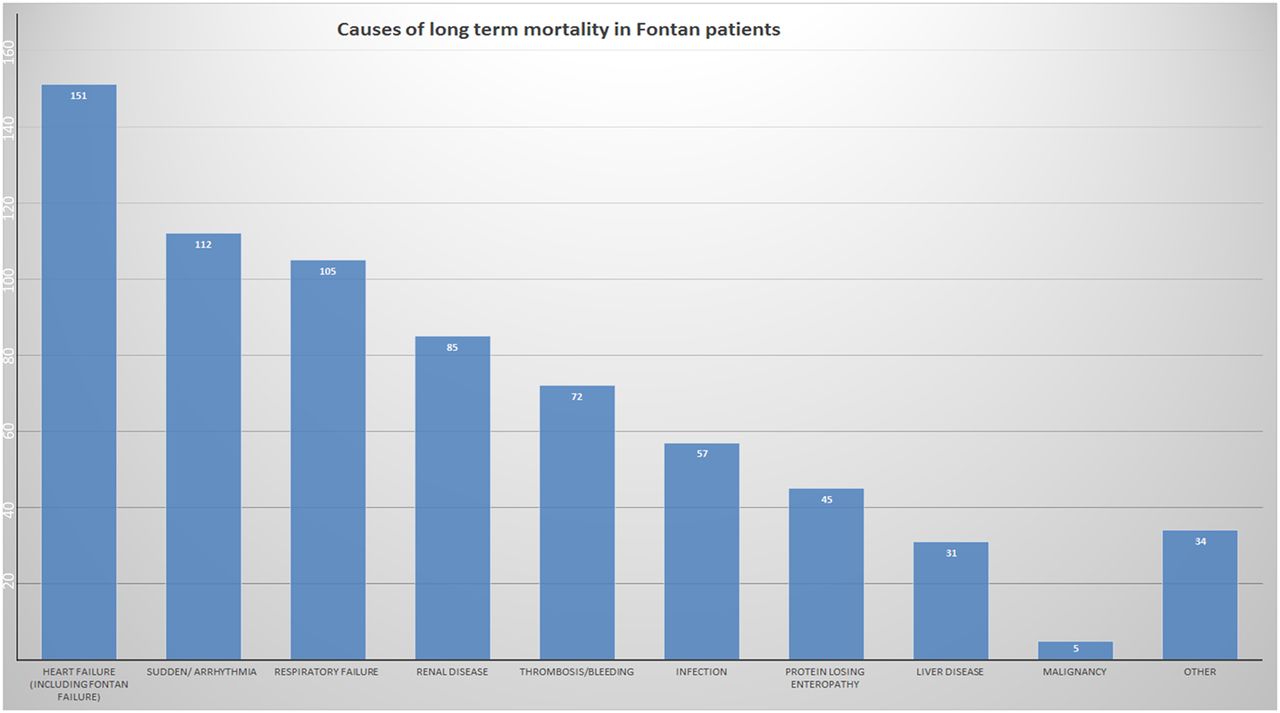
Causes of mortality were inconsistently reported between studies. A cause of late mortality was reported in 697 (70%) of the 1000 late mortalities. Of the reported causes, heart failure including Fontan failure was the leading cause accounting for 151 patients (22% of late mortality). Sudden death/arrhythmia was the cause of death in 112 patients (16%). Respiratory failure and renal disease were the most common non-cardiac causes of late mortality and accounted for 105 and 85 cases of mortality (15% and 12% of late mortality) (figure 2).
{kind=link}
{kind=link}
Causes of late mortality after Fontan procedure.
Predictors of long-term mortality
Era of operation
Earlier date of operation, that is, those operated on in the 1970s and early 1980s was associated with worse long-term outcomes including mortality, Fontan takedown and/or heart transplantation.5–8 This appears to be mainly related to changes in myocardial protection and surgical techniques.6 A recent large study showed a 10-year survival rate after the Fontan procedure of 79% for patients operated on before 1990 compared with 95–98% beyond 1990.9
Preoperative risk factors
The preoperative risk factors reported include age at operation, gender, type of congenital heart defect, single ventricular anatomy (right or left ventricle) and function and atrioventricular (AV) valve regurgitation.
The observation that older age at Fontan operation is associated with worse survival was first denoted by Fontan in 1990.10 In a large Australian/New Zealand popula`tion-based registry, follow-up data of 1006 hospital survivors were collected. Patients operated at >7 years of age had worse long-term survival (HR=2.7, 95% CI 1.2 to 5.7) in multivariable analysis.11 More specifically, in a recent large study of 1052 patients, optimal late survival was observed in patients operated between 2 years and 4 years of age using univariate analysis, although age of operation was not a statistically significant predictor of outcomes in multivariable analysis.9 Some studies reported worse long-term outcomes in men compared with women11 ,12 although a recent large study did not support such sex based differences.9
The type of congenital heart defect was reported to impact late mortality.13–15 Hypoplastic left heart syndrome is associated with worse late outcomes (including death or Fontan failure) in a large contemporary cohort of 529 patients with Fontan circulation. After adjustment for other significant covariates, hypoplastic left heart syndrome had an almost threefold increased risk for late Fontan mortality (HR=2.8, 95% CI 1.1 to 7.5).16 In the same cohort, AV septal defect was not found to predict long-term mortality and this observation was attributed to the more aggressive management of AV valve regurgitation.11 Importantly, heterotaxy syndrome was associated with decreased survival in a number of studies.5 ,13 ,17–19 In a Japanese study that included 335 Fontan patients, heterotaxy syndrome was shown to be an important risk factor for late mortality in multivariate analysis (HR=12.70, 95% CI 1.68 to 150).17
Haemodynamic status prior to Fontan surgery was associated with long-term outcomes in several studies. Higher preoperative pulmonary artery pressure was associated with worse survival with 15 mm Hg reported as a threshold in most studies.12 ,20 ,21 Impaired preoperative ventricular function also correlated with worse long-term survival.20 AV valve regurgitation prior to Fontan completion had an almost twofold increased risk for late mortality (HR=1.9, 95% CI 1.15 to 3.20).13 Additionally patients who had a pacemaker prior to Fontan completion and patients who were not in sinus rhythm prior to Fontan completion, appear to have worse outcomes.9
Operative factors
Long-term outcomes were superior in patients with cavopulmonary Fontan (lateral tunnel and extracardiac conduit) compared with atriopulmonary Fontan.11 ,12 ,18 ,22 In a recent large study 10-year survival for patients who survived 30 days post Fontan procedure was 80% after atriopulmonary connection, 84% after lateral tunnel Fontan and 97% after extracardiac conduit Fontan.9 The survival difference between lateral tunnel and extracardiac conduit was however not statistically significant and was attributed to using lateral tunnel techniques in patients with heterotaxy syndromes in combination with a significant era effect.9 Some studies suggested worse survival in patients with longer aortic cross-clamp time23 or cardiopulmonary bypass time which can be a surrogate for more complex anatomy or concomitant procedures during Fontan surgery.6 Concomitant replacement of the AV valve was associated with worse long-term survival in two studies (HR=4, 95% CI 2.1 to 7.8) in the latter.9
Postoperative factors
Only relatively few postoperative factors influencing late mortality could be identified. These included elevated left atrial pressure, persistent postoperative pleural effusions and elevated postoperative Fontan pressures.
Increased postoperative right atrial pressure (>13 mm Hg) was frequently reported to be associated with increased late mortality or a combined end point of mortality or heart transplantation with (HR=2.05, 95% CI 1.48 to 2.82) in early Fontan survivors in a recent large review of North American experience.9 Persistent pleural effusions (>30 days or requiring reoperation) increased late mortality in hospital survivors (HR=2.9, 95% CI 1.1 to 7.4) in a population-based registry.11 Prolonged pleural drainage (>3 weeks) was also recently confirmed to be associated with increased risk of late mortality in patients who survived at least 30 days after the Fontan procedure on multivariate analysis (HR=1.2, 95% CI 1.05 to 1.26).9 Increased postoperative Fontan pressures >20 mm Hg was a predictor of mortality with an HR=2.14, 95% CI 1.63 to 2.81.9
Long-term cardiac complications
Long-term cardiac complications after the Fontan procedure that may lead to late mortality include arrhythmias, thromboembolic events and heart failure.15
Heart failure/Fontan failure was found to be the most common cause of long-term mortality in our systematic review.15 ,24 Though delayed diastolic filling and time related progressive ventricular stiffness is now well recognised as part of failing Fontan pathophysiology,25 late outcomes data for those with diastolic dysfunction do not yet exist.
Arrhythmia is an important risk factor for long-term mortality in Fontan circulation (HR=1.79, 95% CI 1.18 to 2.72).9 A population based study from Denmark found a steady increase of arrhythmia with age.26 The most common arrhythmia is intra-atrial re-entry tachycardia and is more common in atriopulmonary Fontan due to the dilation of the atrium.27
A composite cardiac risk factor score that included patient age, older style Fontan (atriopulmonary connection and AV), arrhythmia and/or heart failure was indeed strongly predictive of mortality and/or transplant outcomes in a large multi-institutional cohort.28 The presence of two cardiac risk factors was associated with a 4-fold increased risk, whereas three cardiac risk factors was associated with a 10-fold increased risk of mortality or transplantation.
Thromboembolic events account for a significant portion of late mortality (up to 25% in some studies).15 Risk factors for thrombosis include haemodynamic factors with low cardiac output and less pulsatile pulmonary flow in addition to a hypercoagulable state in Fontan patients.29 A recent meta-analysis showed a pooled incidence of 11% and that prophylaxis with aspirin or warfarin decreases the risk significantly (OR 0.4, 95% CI 0.19 to 0.92).29 The location of thrombus is most commonly in the Fontan conduit, intracardiac or in the pulmonary arteries.15 ,29 ,30
Non-invasive cardiac imaging factors
Few studies reported imaging markers predictive of long-term mortality or transplant.31 One study showed that global circumferential strain on transthoracic echocardiogram is predictive of long-term mortality (HR=1.3 per unit change, 95% CI 1.1 to 1.5).32 Ejection fraction was significantly lower in patients who died but did not reach statistical significance on multivariate analysis.32 The same investigators reviewed cardiac MRI in 215 adolescents with Fontan circulation. After a follow-up period of 4 years, 24 (11%) died or were transplanted. The study found that ventricular indexed end-diastolic volume >125 mL/m2 body surface area was a predictor of late mortality (HR=7.7, 95% CI 2.8 to 21.1).31
Cardiopulmonary exercise testing factors
Cardiopulmonary exercise tolerance decreases greatly over the life span of Fontan patients.17 ,28 ,33 ,34 In a large study 321 adult Fontan survivors had cardiopulmonary exercise testing and were then observed for the combined study end point of death or transplantation or cardiac hospitalisation over 21 months. Though almost all peak exercise and anaerobic threshold parameters (VO2, % of predicted VO2, heart rate reserve, anaerobic threshold, minute ventilation (VE)/carbon dioxide production (VCO2 slope), were able to predict unscheduled cardiovascular hospital admissions, only peak VO2 was able to independently predict mortality HR=0.88 for each 1% increase in peak VO2.17 Another study showed that a peak VO2 of <16.6 mL/kg/min and peak-exercise heart rates of <122.5 bpm were predictors for long-term mortality with an HR=7.5, CI 2.6 to 21.6 and HR=10.6, CI 3 to 37.1, respectively.
Non-cardiac predictors of late mortality
Non-cardiac risk factors evaluated in the literature include plastic bronchitis (PB), hepatic disease, protein losing enteropathy (PLE), high altitude and renal dysfunction.11 ,35–37 A case–control study looking at 25 patients with PB compared with 45 Fontan patients without PB revealed a 32% mortality in patients with PB with a median transplant-free survival of 8.3 years post diagnosis.36 PB was significantly associated with mortality (OR 5.0, 95% CI 1.1 to 26.8).36 Respiratory failure is an important cause of death in the Fontan population. The mechanisms by which the lungs exert their mortality effect in this patient population are not well understood.
Few studies examined the effect of hepatic disease on mortality.38–41 A recent study reviewed liver data including histopathology and biochemistry.40 Cirrhosis was found to be a late complication with a high mortality (1-year, 43%; 2-year, 65%). The strongest predictor of developing cirrhosis was a previous diagnosis of hypoplastic left heart syndrome. The recently reported VAST score (Varices, Ascites, Splenomegaly or Thrombocytopenia, 1 point each), highlighting the importance of portal hypertension, demonstrated that a VAST score ≥2 confers a ninefold risk for a major adverse event.39 PLE is an important risk factor for mortality and/or transplantation.42 A multi-institutional study in 1998 showed that mortality in patients with PLE was at least 50% over 5 years.35 Given this devastating prognosis, the authors suggest that instead, early transplantation should be considered.35 More recently a single institution study showed improved 5-year survival (88%) and attributed these more favourable late PLE outcomes to early detection and more aggressive management strategies.43
High altitude has a significant impact on Fontan patients, reducing transplant-free survival and significantly increasing (by more than twofold) the incidence of PLE and clinical decompensation. This was attributable to increased pulmonary vascular resistance at high altitude.21
Although renal insufficiency was found to be an important non-cardiac cause of death in a number of publications, there is limited literature to describe the spectrum and the exact pathology of renal dysfunction in this population. A recent study showed that postoperative renal insufficiency is associated with increased risk of late mortality (HR=2.5, 95% CI 1.7 to 3.9).9 Another study showed a rate of acute kidney injury of 42% after the Fontan procedure.44
Serological biomarkers
Hyponatraemia and elevated brain natriuretic peptide (BNP) have been studied in Fontan patients.
Hyponatraemia is a well established mortality marker for non-congenital heart disease associated heart failure.45 In a retrospective study of 1004 patients with adult congenital heart disease, including 54 adult Fontan patients, the presence of hyponatraemia (<136 mmol/L) was observed in 29.6% of Fontan patients.46 Hyponatraemia was associated with a significant increase in risk of death in this study (HR=2.59, 95% CI 1.68 to 3.97).46
Several studies report data on BNP levels in the Fontan physiology.47 In a study that included 369 patients with Fontan circulation, elevated BNP was a predictor of mortality (HR=1.13 per 10 pg/mL; 95% CI 1.02 to 1.25).48 Other studies suggested an association between elevated BNP levels and worse functional status in Fontan patients as expressed by NYHA class rather than mortality.47
Discussion
For this systematic review, 28 relevant articles which described late mortality in Fontan patients were evaluated. Overall, late mortality in Fontan patients was 2.1% per year and largely attributable to Fontan/heart failure (22%) and sudden cardiac/arrhythmic death (16%). Overall, we found considerable differences between studies in design and reported risk factors. To facilitate better and more uniform risk stratification risk factors were classified into nine different categories.
Patients with congenital heart disease and a Fontan circulation are at serious risk for late complications such as arrhythmias, Fontan failure and early death.9 Theoretically, this unfavourable course may be improved by risk appropriate surveillance leading to timely intervention such as Fontan revision surgery, invasive arrhythmia management and/or cardiac transplantation.27 Thus appropriate identification of high-risk patients is important for improving long-term care.
In this systemic review, we found a large number of risk factors reported in literature. The 35 risk factors (see table 2) identified were divided into the following predefined categories: (1) era-related, (2) preoperative factors, (3) operative factors, (4) postoperative factors (5) long-term cardiovascular complications, (6) cardiac imaging, (7) exercise stress testing, (8) non-cardiac factors, (9) serological factors (table 2). Preoperative anatomical factors such as hypoplastic left heart are likely disadvantageous because a morphological Right ventricle (RV) is more likely to become dysfunctional during long-term follow-up.16 High pulmonary or Fontan pressures preoperatively or postoperatively may reflect early vascular changes in the pulmonary vasculature, which may further progress over time.9 Atriopulmonary Fontan is associated with high rates of supraventricular arrhythmias, after which further clinical deterioration is common.22 Extracardiac manifestations such as PLE or hepatic fibrosis can be considered a sign of Fontan failure, and increasing central venous pressures.9 In stress testing, reduced peak heart rate emerged as the most promising factor. This may reflect autonomic dysfunction and the inability to enhance pulmonary blood flow during exercise.34 Although cardiac imaging and serological testing are potentially very useful in risk stratification, only two papers investigated the prognostic value of these parameters.
Summary of factors associated with long-term mortality classified into categories
Future directions
Retrospective, large data repositories such as the multi-institutional Australian and New Zealand Registry have proven enormously effective in lending statistical power to assess multiple unanswered questions.11 ,13 ,49 Large multinational collaboration will allow analysis of currently employed surveillance techniques and their utility in identifying at-risk Fontan patients.50 Ideally, these collaborations will produce a risk score that helps clinicians in outpatient settings. Identifying patients at high risk will guide interventions and resource utilisation in this patient population.
Limitations
Most of the studies reviewed in this systematic review, were retrospective, single-centre registries. Although these studies provided valuable outcomes information, selection or follow-up bias cannot be excluded. Importantly, across different studies, there was large variation in underlying defects, previous palliation, timing of surgery, surgical techniques used and perioperative care.
Conclusions
This systematic review provides an overview of late Fontan mortality and factors associated with late mortality across nine different categories. To facilitate and improve decision making, the factors associated with long-term mortality were classified into nine different categories. Further studies may lead to creation of a Fontan risk score for mortality to further help risk stratification and resource utilisation in this patient population.
References
Footnotes
Contributors TA wrote the first draft of the manuscript. TA, JPB, LZ, JMK, SPH and GRV reviewed the included studies in the systematic review. GRV, JPB, LZ, JMK, SPH critically revised the manuscript. BZ and MEE provided statistical support.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.