Article Text

Abstract
Objective Supplemental oxygen therapy may increase myocardial injury following ST-elevation myocardial infarction (STEMI). In this study, we aimed to evaluate the effect of the dose and duration of oxygen exposure on myocardial injury after STEMI.
Methods Descriptive analysis of data from a multicentre, prospective, randomised, controlled trial of 441 patients with STEMI randomised to supplemental oxygen therapy or room air breathing. The primary endpoint was myocardial infarct size as assessed by cardiac biomarkers, troponin (cTnI) and creatine kinase (CK). Oxygen therapy was commenced by paramedics, and continued for up to 12 h postintervention in hospital. Supplemental oxygen exposure was calculated as the area under the dose×time curve for oxygen administration over the first 12 h, and then assessed for its association with cTnI/CK release using multivariable linear regression.
Results The median supplemental oxygen exposure was 1746 L (IQR: 960–2858). After adjustment for potential confounders, every 100 L increase in oxygen exposure in the first 12 h was associated with a 1.4% (95% CI 0.6% to 2.2%, p<0.001) and 1.2% (95% CI 0.7% to 1.8%, p<0.001) increase in the mean peak cTnI and CK, respectively. Excluding patients who developed cardiogenic shock, recurrent myocardial infarction or desaturations (SpO2<94%) during admission, every 100 L increase in oxygen exposure was associated with a 1.2% (95% CI 0.2% to 2.1%, p=0.01) and 1.0% (95% CI 0.3% to 1.7%, p=0.003) increase in the mean peak cTnI and CK, respectively. The median supplemental oxygen exposure of 1746 L would result in a 21% (95% CI 3% to 37%) increase in infarct size according to the cTnI profile.
Conclusions Supplemental oxygen exposure in the first 12 h after STEMI was associated with a clinically significant increase in cTnI and CK release.
Statistics from Altmetric.com
Introduction
Although several studies of supplemental oxygen therapy in patients suffering acute myocardial infarction (AMI) have indicated the presence of deleterious physiological and clinical outcomes,1–3 its use remains common in clinical practice.4 Recently, in the multicentre, prospective, randomised, Air Versus Oxygen in myocarDial infarction (AVOID) controlled trial, normoxic patients with ST-elevation myocardial infarction (STEMI) randomised to routine supplemental oxygen experienced a 27% increase in creatine kinase (CK) compared with patient's breathing room air.2 This finding comes almost four decades after Rawles and Kenmure demonstrated in a double-blind randomised controlled trial that inhaled oxygen therapy increased myocardial injury by 24% in patients with AMI compared with breathing compressed air.1 Furthermore, supportive data from smaller physiological studies also show that supplemental oxygen may reduce coronary perfusion and heighten oxidative stress.3 ,5–7
The threshold at which oxygen therapy begins to increase myocardial injury following AMI remains unclear. To date, both the dose and duration of treatment of oxygen therapy have varied considerably across clinical studies. Earlier physiological studies have opted for relatively high concentrations of supplemental oxygen of 10–15 L/min delivered for short periods of time,3 a practice that varies from those adopted in contemporary clinical trials.8–10 In the AVOID trial, patients randomised to the oxygen group received oxygen therapy at 8 L/min via facemask in the prehospital setting, while inhospital oxygen use was administered according to local hospital protocols.9 This resulted in heterogeneous oxygen administration that reflects real-world utility of oxygen therapy in the setting of AMI.
It is not known whether the deleterious effects of oxygen therapy in AMI are dependent on the dose and duration of its administration. In this descriptive analysis of data from the AVOID trial, we evaluate the effect of supplemental oxygen exposure on biochemical and cardiac MRI (CMR) measures of myocardial injury in patients with STEMI.
Methods
Design, setting and participants
The study was a descriptive analysis of data from a multicentre, prospective, randomised, controlled trial. The AVOID trial randomised 638 prehospital suspected patients with STEMI between October 2011 and July 2014, who were transferred to 9 percutaneous coronary intervention (PCI)-capable hospitals in Melbourne, Australia. Details of the trial design, protocol and results have been published elsewhere (NCT01272713).2 ,9 The trial and this study were approved by ethics committees at each participating hospital, and delayed written informed consent from the patient or next of kin was sought after stabilisation in hospital.
Patients were randomised according to the following criteria: age ≥18 years; chest pain symptoms <12 h prior; prehospital ECG evidence of STEMI, including (1) ST-segment elevation of ≥0.1 mV in two contiguous limb leads or (2) ≥0.2 mV in two contiguous chest leads, or (3) new left bundle branch block pattern. Exclusion criteria included hypoxaemia on room air (SpO2<94% measured on pulse oximeter), oxygen administration prior to randomisation, altered conscious state or planned transport to a non-participating hospital.
Randomisation and interventions
Patients were randomly assigned to either the oxygen or room air using opaque envelopes containing computer-generated treatment allocation. In the oxygen group, paramedics administered supplemental oxygen via face mask at 8 L/min until arrival at hospital. Inhospital oxygen administration was according to hospital treatment protocols. In the room air group, patients received no supplemental oxygen either prehospital or inhospital unless their oxygen saturations fell below 94%. Oxygen was then indicated to maintain a target oxygen saturation of 94%. Details of oxygen use were recorded in the case report form at regular intervals, including at randomisation, at hospital arrival, at the catheterisation laboratory and at two-hourly intervals thereafter up to 12 h postprocedural intervention. Individuals involved with the delivery of oxygen therapy prehospital and inhospital were not blinded to treatment assignment, due to the impracticality and potential risk of concealing oxygen treatment.
Study outcomes
Definitions of the end points are detailed elsewhere.2 The AVOID trial utilised highly correlated co-primary endpoints of peak troponin I (cTnI) and CK. To obtain a comprehensive picture of the treatment effect, the area under the curve (AUC72) for cTnI and CK concentration in serum for the first 72 h were also measured. Blood sampling was conducted at baseline and then six hourly for the first 24 h and 12 hourly out to 72 h after admission. Secondary endpoints measured at hospital discharge and 6 months included ECG ST-segment resolution; mortality and major adverse cardiac events (includes death, recurrent myocardial infarction, repeat revascularisation and stroke). At 6 months, a contrast-enhanced CMR scan was performed on consenting patients with no contraindications (n=139, 31.5%).
Statistical analysis
A detailed description of the statistical analysis is provided in the online supplementary appendix. Statistical analyses were performed using Stata Statistical Software 11 (StataCorp, 2009, College Station, Texas, USA). The primary analysis was performed on the intention-to-treat population, or 441 patients with confirmed STEMI following emergent coronary angiogram. Supplemental oxygen exposure in litres was calculated using trapezoidal integration for the area under the dose×time curve over the first 12 h. We used spearman's rank correlations to compare the unadjusted relationship between myocardial injury and varying time intervals of supplemental oxygen exposure (see online supplementary appendix table 1). The total oxygen exposure between baseline and 12 h (AUC12) had the strongest correlation with measures of myocardial injury and was adopted for all multivariable analyses.
For the comparison of baseline characteristics, procedural details and clinical outcomes, we stratified the population into four groups. Patients receiving oxygen were stratified into thirds on the basis of supplemental oxygen exposure (AUC12). The final groups included patients with no supplemental oxygen exposure (n=128), low supplemental oxygen exposure of between 1 and 1160 L (n=105), moderate supplemental oxygen exposure of between 1161 and 2376 L (n=104) and high supplemental oxygen exposure of >2376 L (n=104). Variables that approximated a normal distribution were summarised as mean ±SD, and groups were compared using analysis of variance. Non-normal variables were represented as median and first and third quartiles (Q1, Q3), and groups were compared using the Wilcoxon rank sum test. Binomial variables were expressed as proportions and 95% CIs and groups compared using χ2 tests.
To estimate the total cTnI and CK release in the first 72 h we used trapezoidal integration of AUC72. Missing biomarker assays were replaced with multiple imputation using the Markov Chain Monte Carlo method.11 ,12 The adjusted effect of oxygen exposure on biochemical measures of myocardial injury (peak and AUC72 cTnI/CK) was assessed using linear regression models. The inclusion of variables in the model was based on previous literature,13 and included age, gender, diabetes, smoker status, hypertension, culprit artery, Killip class, preintervention and postintervention thrombolysis in myocardial infarction flow, procedural complication and symptom-to-intervention time. The final model was tested for goodness-of-fit, normality of residuals and multicolinearity. A log-transformation of the outcome data significantly improved the normality of residuals. Comparison of the treatment effect was made after back-transformation, representing the percentage change in geometric mean cTnI and CK release (refer to the see online supplementary appendix for additional detail). For ease of interpretation, the effect of oxygen exposure on myocardial injury was presented as increments of 100 L of supplemental oxygen in the first 12 h (equivalent to administering oxygen at 4 L/min for 25 min). Measures of infarct size assessed by CMR at 6 months (infarct mass in grams and infarct size as a proportion of left ventricular mass) were also assessed using the same approach. Simple curves for the predicted geometric mean peak cTnI and CK were constructed for the average patient by back-transforming the regression function.
As postrandomisation data may introduce selection bias in our analyses, we verified our results using a series of sensitivity analyses excluding subgroups, which could confound the treatment effect, including (1) patients randomised to room air; (2) patients who developed cardiogenic shock, recurrent myocardial infarction or a desaturation (SpO2<94%) and (3) patients with any adverse clinical event at discharge, including mortality, recurrent myocardial infarction, stroke or transient ischaemic attack, cardiogenic shock, coronary artery bypass grafting, major bleeding and arrhythmia.
Results
Study population
All 218 patients randomised to the oxygen group received oxygen therapy in the first 12 h. Of the 223 patients randomised to the room air group, 102 (45.7%) patients received oxygen in the first 12 h according to protocol. Figure 1 of the online supplementary appendix shows the distribution of supplemental oxygen exposure (AUC12) for the first 12 h in the overall population and by treatment arms. The median supplemental oxygen exposure was 1746 L (IQR: 960–2858) in the overall population, but was higher in patients randomised to the oxygen group compared with the room air group (2258 L vs 960 L, p<0.001). When oxygen was administered, the median oxygen dose was lower in the room air group compared with oxygen group (3 L/min vs 6 L/min, p<0.001).
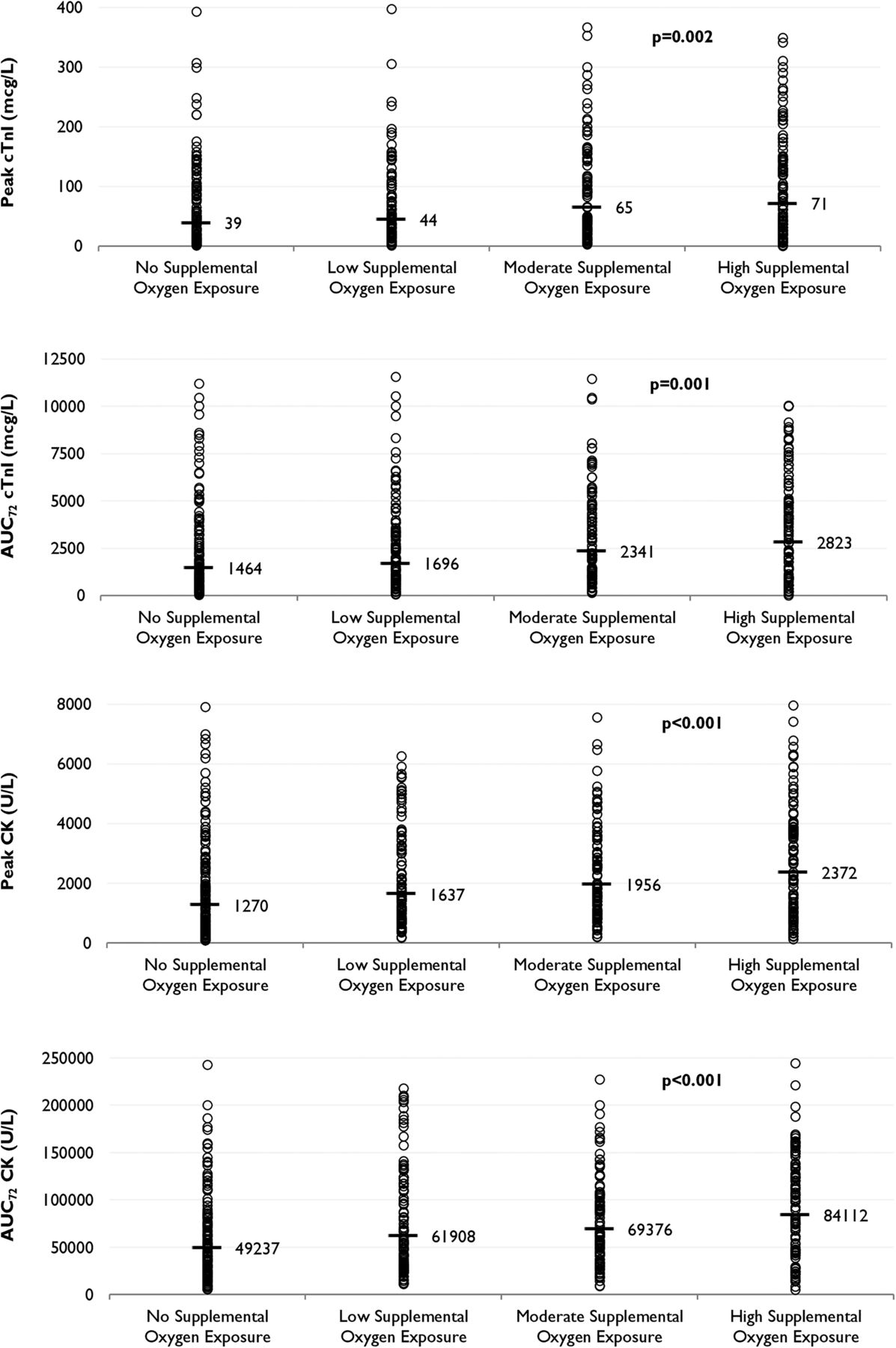
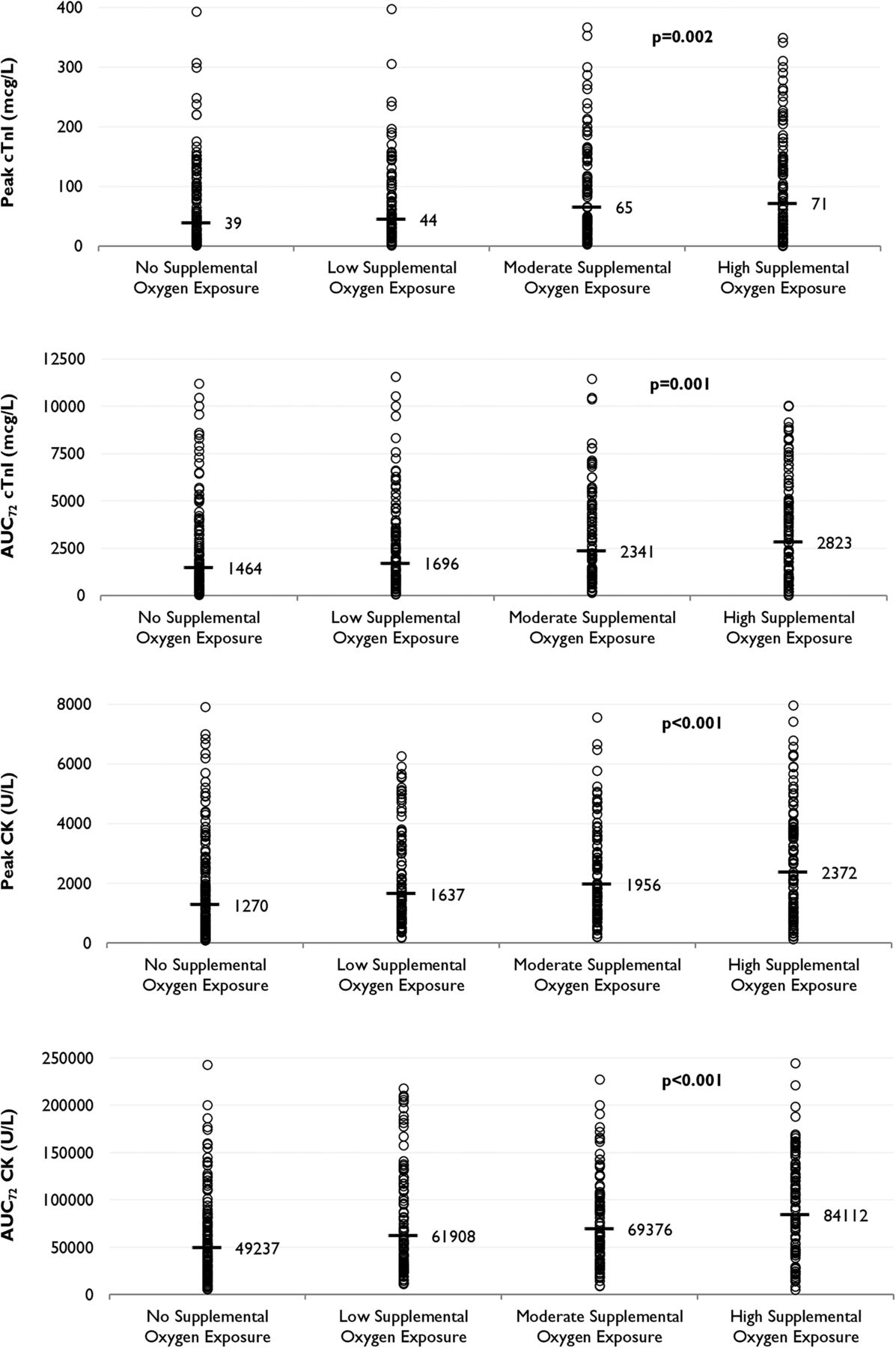
Distribution of biochemical measures (troponin I (cTnI)/creatine kinase (CK)) across oxygen exposure groups. Black lines represent geometric mean peaks. p Values calculated using one-way analysis of variance for the difference in log-transformed means.
Baseline and procedural characteristics
With the exception of dyslipidaemia, demographics and medical history did not differ significantly after stratification of patients into supplemental oxygen exposure groups (table 1). Patients with high oxygen exposure described higher baseline pain scores, but had similar findings with respect to the extent of coronary artery disease and procedural details (table 2). Both symptom-to-intervention time and door-to-intervention did not differ between groups. Length of hospital stay was higher in patients with high oxygen exposure (p<0.001).
Baseline characteristics of patients with confirmed STEMI
Procedural details of patients with confirmed STEMI
Adverse clinical outcomes
At hospital discharge, recurrent myocardial infarction, cardiogenic shock, major bleeding and arrhythmias were experienced more frequently in patients receiving oxygen, with the highest proportion of events occurring in the high oxygen exposure group (table 3). The median time to recurrent myocardial infarction after admission was 2 days (IQR: 1–4). With the exception of recurrent myocardial infarction, adverse outcomes at 6 months were similar across groups.
Adverse clinical endpoints at hospital discharge and 6-month follow-up in patients with confirmed ST-elevation myocardial infarction
Relationship between oxygen exposure and myocardial injury
The difference in the unadjusted geometric mean peak/AUC72 for cTnI and CK was statistically significant across oxygen exposure groups (figure 1). After adjustment for potential confounders of myocardial injury, table 4 shows that every 100 L of oxygen exposure was associated with a 1.4% (95% CI 0.6% to 2.2%, p<0.001) and 1.2% (95% CI 0.7% to 1.8%, p<0.001) increase in the geometric mean peak cTnI and CK, respectively. Similar estimates for the increase in AUC72 cTnI and AUC72 CK release were also found. A 1.2% (95% CI 0.1% to 2.3%, p=0.03) increase in the geometric CMR infarct mass and a 0.9% (95% CI 0.01% to 1.9%, p=0.06) increase in the infarct size as a proportion of left ventricular mass was observed in a subgroup of 139 patients undergoing a 6-month CMR.
Unadjusted and adjusted effect of supplemental oxygen exposure (per every 100 L increase in the first 12 h) on biochemical and CMR measures of myocardial infarct size
For the sensitivity analyses, excluding subgroups that could potentially confound the treatment effect resulted in a slight diminution of the treatment effect (table 4). In patients randomised to the oxygen group, the effect of every 100 L of supplemental oxygen exposure in the first 12 h was associated with a 1.5% (95% CI 0.2% to 2.7%, p=0.02) increase in the geometric mean peak cTnI and a 1.1% (95% CI 0.2% to 2.0%, p=0.01) increase in the geometric mean peak CK. Similarly, after excluding patients who developed cardiogenic shock, recurrent myocardial infarction or desaturations (SpO2<94%) during admission, every 100 L of supplemental oxygen exposure in the first 12 h was associated with a 1.2% (95% CI 0.2% to 2.1%, p=0.01) increase in the geometric mean peak cTnI and a 1.0% (95% CI 0.3% to 1.7%, p=0.003) increase in the geometric mean peak CK. Excluding all patients with any adverse outcome at hospital discharge resulted in similar findings. The predicted increase in geometric mean peak cTnI and CK after holding all other covariates at their mean value is shown in figure 2.

{kind=link}
{kind=link}
Effect of supplemental oxygen exposure on the predicted geometric mean peak troponin I (cTnI)/creatine kinase (CK) holding model covariates* at their mean value. Solid line represents the overall population, and the dotted line represents the population without cardiogenic shock, recurrent myocardial infarction or desaturation (SpO2<94%) during admission.
Discussion
Our findings suggest that incremental exposure to supplemental oxygen in the first 12 h after STEMI is associated with a clinically significant increase in myocardial injury. For instance, a typical patient in our study receiving the median oxygen exposure of 1746 L in the first 12 h (equivalent to receiving 6 L/min for less than 5 h) would experience a 17%–21% increase in myocardial infarct size according to the CK and cTnI profiles. As biochemical measures of myocardial injury are highly correlated with absolute infarct volume,2 ,13 our findings are of clinical importance and utility.
Our measure of oxygen exposure accounts for both the dose and duration of oxygen treatment, and has been used in previous studies to evaluate the effect of oxygen exposure on lung injury.14 ,15 In our study, the area under the 12 h oxygen dose×time curve was strongly correlated with measures of myocardial injury, which performed better than peri-interventional measures of oxygen exposure, which only account for oxygen supplementation in the early stages of reperfusion. These observations suggest that increases in myocardial injury in relation to oxygen exposure are cumulative over the duration of treatment, and not necessarily related to oxygen administration at reperfusion. This may explain why Rawles and Kenmure also demonstrated an increase in myocardial injury in patients exposed to oxygen therapy for 24 h after AMI without reperfusion.1
Since the early 1980s, oxygen-derived free radicals have been implicated in the pathogenesis of reperfusion injury, with studies showing that a sudden ‘burst’ of oxygen free radical production shortly after reperfusion can promote tissue damage and arrhythmias.16 In lung epithelium, the formation of reactive oxygen species increases rapidly after exposure to hyperoxia, but returns to pretreatment levels within 30 min of oxygen cessation.17 The intensity of free radical production is highly attenuated by the fraction of inspired oxygen, with higher doses of oxygen being exponentially associated with the production of reactive oxygen species.17 ,18 Studies have postulated that reactive oxygen species are responsible for the coronary vasoconstriction induced under hyperoxic conditions,19 which could be self-limiting after the normalisation of blood oxygen tension.20 Hyperoxaemia is also associated with a number of cardiovascular responses including a reduction in coronary blood flow and myocardial oxygen consumption, and an increase in coronary vascular resistance.3 The relatively high oxygen saturations observed in the moderate to high oxygen exposure groups indicates that hyperoxaemia was present in a large proportion of patients in our study, and this may explain why these groups experienced greater myocardial injury after STEMI.
Although the AVOID trial was not powered to detect differences in adverse clinical outcomes, there may be some evidence that oxygen increases the frequency of arrhythmias and recurrent myocardial infarctions after STEMI.2 Although the frequency of arrhythmias and recurrent myocardial infarctions was associated with increasing oxygen exposure in our study, it is plausible that this finding also represents residual confounding, where increasing levels of oxygen exposure reflect the increasing severity of illness. Conversely, many of the adverse outcomes observed in our study occurred outside the 12 h oxygen administration period, with almost 75% of recurrent myocardial infarctions occurring at least 2 days after admission. Although our models adjust for a wide range of potential confounders of myocardial injury, other factors such as individual clinical judgement including the degree of patient ‘distress’ is subjective and difficult to adjust for. Although our results were unaffected after the exclusion of patients with adverse clinical outcomes during admission (ie, the ‘complicated’ STEMIs), these sensitivity analyses reduce the sample size and widen the CIs of our estimates, and larger studies may be useful in corroborating our findings.
The results of our study should be interpreted in the context of the trial protocol. Unlike other clinical trials that assigned a standard dose of oxygen supplementation for up to 24 h after randomisation,1 ,8 ,10 the AVOID trial allocated oxygen dosing according to local hospital protocols.9 As a result, supplemental oxygen was highly heterogeneous and was infrequently administered to patients in high doses or durations, such as those recommended in other trial protocols (eg, 6 L/min over 12 h).10 In addition, the AVOID trial employed a relatively conservative threshold for hypoxaemia on pulse oximeter (SpO2<94%). As a result, a large proportion of patients randomised to the air group received supplemental oxygen in the first 12 h (45.7%), most for low-range desaturations of 90%–93% on pulse oximeter. Comparing these findings with other trials is difficult because the frequency of cross-over between groups has not been reported.1 ,8 A 90% oxygen saturation threshold on pulse oximeter is currently being evaluated by a Swedish-based clinical trial,10 and this will help determine the safety and feasibility of further reducing the need for oxygen therapy in the treatment of patients with AMI.
Study limitations
Our study has several limitations. This was a descriptive analysis of data from a randomised controlled trial. Although the primary outcome was prespecified, our measure of oxygen exposure was defined a posteriori and therefore our analysis is exploratory in design. The study is also affected by limitations of the main trial, including a lack of blinding of oxygen treatment, missing biomarker data, the limited application of CMR scanning of infarct size and no central core laboratory for the assessment of biomarkers.2 In our study, we excluded 8.2% of patients with no completed cTnI assays and 0.5% with no completed CK assays. Although we attempted to limit the possibility of selection bias, it is not clear whether our sensitivity analyses and covariate adjustments completely account for illness severity factors, which could confound our measures of myocardial injury. Our CMR scans were completed in 31.5% patients, and due to feasibility constraints we could not perform early CMR scans to consider other index measures of myocardial injury such as myocardial salvage and infarct size as a proportion of area at risk. In addition, we did not collect other measures of oxygen exposure such as arterial oxygen tension and the fraction of inspired oxygen and therefore it is not known how these variables would influence our results. Finally, the validity of supplemental oxygen exposure as a variable in our models relies on the accurate measurement of the dose and duration of oxygen therapy in the clinical setting, which may not be free from measurement error.
Conclusion
In this study, supplemental oxygen administered in the first 12 h after STEMI was associated with a dose-dependent increase in cTnI and CK release. Our findings suggest that a typical patient receiving supplemental oxygen exposure in the first 12 h after STEMI would experience an approximate 20% increase in myocardial infarct size. Although minimising the dose and duration of supplemental oxygen may help limit further myocardial injury after STEMI, further research is required to better elucidate the link between hyperoxia and myocardial injury, and determine optimal oxygen saturation targets during treatment.
Key messages
What is already known on this subject?
The use of routine oxygen therapy for uncomplicated ST-elevation myocardial infarction (STEMI) is not recommended by current international treatment guidelines. Results released recently from the Air Versus Oxygen in myocarDial infarction (AVOID) randomised controlled trial suggest that routine supplemental oxygen is of no clinical benefit, and may be associated with increased myocardial injury after STEMI.
What might this study add?
The effect of the dose and duration of oxygen exposure on myocardial injury is not known in patients suffering STEMI. In this descriptive analysis of the AVOID trial data, every 100 L of supplemental oxygen administered in the first 12 h after STEMI was associated with a 1.4% and 1.2% increase in the mean peak troponin I (cTnI) and creatine kinase (CK), respectively. The treatment effect was maintained after the exclusion of complicated STEMI episodes, which could confound the treatment effect. In our study, the median supplemental oxygen exposure of 1746 L in the first 12 h would result in a 17%–21% increase in infarct size according to the CK and cTnI profiles.
How might this impact on clinical practice?
Minimising the dose and duration of oxygen administration could help limit further myocardial injury in patients with STEMI. Further research is required to determine the optimal blood oxygen saturation target in hypoxic patients with STEMI.
Acknowledgments
The authors are grateful to all paramedics and hospital staff who contributed to the AVOID trial.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Collaborators See online supplementary appendix for a full list of AVOID investigators.
Contributors ZN, DS and KS conceived and designed the research. ZN, DS and KS acquired the data and performed the statistical analyses. KS, BB, DMK, ITM, JEB, MS, SB and PC handled funding and supervision. ZN and DS drafted the manuscript, and all authors made critical revisions for key intellectual content.
Funding This work was supported by the Alfred Foundation (Melbourne, Australia), FALCK Foundation (Wijnegem, Belgium) and Paramedics Australasia (Melbourne, Australia).
Competing interests DS and JEB are both supported by co-funded NHMRC/NHF fellowships (#1090302/100516) (#1069985/100136). KS, SB, PC, AHE, AJT, ITM and DMK are supported by National Health and Medical Research Council of Australia grants.
Ethics approval Alfred Health Human Research Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.