Article Text

Abstract
Background In patients with acquired heart failure, hypoalbuminaemia is associated with increased risk of death. The prevalence of hypoproteinaemia and hypoalbuminaemia and their relation to outcome in adult patients with congenital heart disease (ACHD) remains, however, unknown.
Methods Data on patients with ACHD who underwent blood testing in our centre within the last 14 years were collected. The relation between laboratory, clinical or demographic parameters at baseline and mortality was assessed using Cox proportional hazards regression analysis.
Results A total of 2886 patients with ACHD were included. Mean age was 33.3 years (23.6–44.7) and 50.1% patients were men. Median plasma albumin concentration was 41.0 g/L (38.0–44.0), whereas hypoalbuminaemia (<35 g/L) was present in 13.9% of patients. The prevalence of hypoalbuminaemia was significantly higher in patients with great complexity ACHD (18.2%) compared with patients with moderate (11.3%) or simple ACHD lesions (12.1%, p<0.001). During a median follow-up of 5.7 years (3.3–9.6), 327 (11.3%) patients died. On univariable Cox regression analysis, hypoalbuminaemia was a strong predictor of outcome (HR 3.37, 95% CI 2.67 to 4.25, p<0.0001). On multivariable Cox regression, after adjusting for age, sodium and creatinine concentration, liver dysfunction, functional class and disease complexity, hypoalbuminaemia remained a significant predictor of death.
Conclusions Hypoalbuminaemia is common in patients with ACHD and is associated with a threefold increased risk of risk of death. Hypoalbuminaemia, therefore, should be included in risk-stratification algorithms as it may assist management decisions and timing of interventions in the growing ACHD population.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
The number of adult patients with congenital heart disease (ACHD) is increasing. Despite ongoing research and continuous improvement in care in what is increasingly recognised as a condition with multiorgan involvement, mortality remains considerable.1 Risk stratification is an essential component of the management of patients with ACHD, and identification of parameters, both cardiac and non-cardiac, strongly related to outcome is crucial.2–4
Hypoalbuminaemia is a marker of liver and renal dysfunction, but also advanced cardiovascular disease, subclinical systemic inflammation and endothelial dysfunction.5 Albumin is the most abundant protein in plasma and the main determinant of plasma oncotic pressure. It counterbalances hydrostatic pressure and controls fluid distribution in body compartments. Moreover, albumin affects the pharmacokinetics of many drugs, thus, modulating response to treatment. Hence, hypoalbuminaemia may result or contribute to pulmonary or peripheral congestion, influence pharmacological therapy and, ultimately, mortality in ACHD.6 Hypoalbuminaemia has been reported in selected subgroups of patients with ACHD, but the prevalence of hypoalbuminaemia and its relation to outcome across the spectrum of patients with ACHD remains unknown.
We sought to examine the prevalence and prognostic significance of hypoalbuminaemia in a large single-centre cohort of patients with ACHD.
Patients and methods
This was a retrospective cross-sectional study. Data on all patients with ACHD under active follow-up at our institution since 2000 were retrieved and studied. Adult patients who had albumin levels assessed at our institution were enrolled in the study; when multiple tests were performed, the first test during the study period was included and analysed.
Albumin was assessed in all patients hospitalised in our institution, in patients undergoing routine, periodic comprehensive 1-day assessment (day case assessment), as well as in the outpatient clinic setting mainly in symptomatic patients and those on heart failure or other treatments. Over the last several years, albumin levels were also routinely assessed in patients with Fontan-type circulation and in patients with cyanotic heart disease with or without pulmonary arterial hypertension.
For the scope of this study, we defined the start of adulthood as age of ≥16 years. Demographic and clinical data were obtained from our dedicated clinical database and the patient's clinical records. Mortality data were retrieved from the national database.
Patients were grouped by primary diagnosis into major ACHD groups. Moreover, they were classified according to ACHD complexity based on the Bethesda Conference classification.7 Estimated survival and standardised mortality ratio for an age-matched and gender-matched cohort was based on the Interim Life Tables for England and Wales (2007–2009) published by the Government Actuary's Department. Total serum protein and albumin were measured on the Beckman DxC600 or LX20 analyser (Beckman Coulter, High Wycombe, UK). Albumin was measured by a timed endpoint method at 600 nm using bromocresol purple, and total protein was measured by a timed endpoint biuret method at 560 nm.
Statistical analysis
Statistical analyses were performed using R-package V.3.0.2 for Windows and MedCalc for Windows, V.11.6.1.0 (MedCalc Software, Mariakerke, Belgium).8 Continuous variables are presented as mean±SD or median and IQR, shown in parentheses, depending on data distribution. Categorical variables are presented as number (percentage). Data distribution was assessed for normality using the Shapiro–Wilk test. In case of normally distributed variables, comparison between groups was performed using unpaired two-tailed t test or Welch test in case of unequal variances. For data demonstrating a non-normal distribution, Mann–Whitney test was used. Differences in continuous variables between multiple groups were assessed using one-way analysis of variance. Categorical variables were compared using χ2 test. Predictors of hypoalbuminaemia were identified using logistic regression analysis. The relation between hypoalbuminaemia and other clinical and demographic parameters to mortality was assessed using Cox proportional hazards regression analysis.
Threshold analysis for albumin is presented as a functional form of the unadjusted relationship between plasma albumin concentration and the hazard of death and is plotted using termplot function in R. Unadjusted Kaplan–Meier survival curves were also plotted and the difference in survival between patients with and without hypoalbuminaemia was assessed using the log-rank test. Sensitivity analysis was performed after exclusion of serum albumin measured during infection (clinical signs of infection or C-reactive protein (CRP) >20 mg/dL or white blood cells >107/mL) or within 2 weeks postcardiac surgery or percutaneous intervention. Also, as serum albumin concentration may have changed over the study period, we have performed a sensitivity analysis using all values recorded in each patient during study period and albumin analysed as a time-dependent covariate in the Cox regression model. A two-sided p value of <0.05 was considered indicative of statistical significance.
Results
Demographics
In total, 2886 patients with ACHD were included in the analysis. Demographic and clinical characteristics are presented in tables 1 and 2. Mean age at baseline was 33.3 (23.6–44.7) years, and 50.1% of patients were men. Data on serum creatinine, sodium or liver status (aspartate transaminase (AST) or alanine transaminase (ALT)) were available in 99% of patients. The largest diagnostic groups were patients with valve or left or right outflow tract disease (n=518), atrial septal defect (n=479) and tetralogy of Fallot (n=474). When classified according to the severity of the underlying congenital defect (using the Bethesda classification), 1223 (42.4%) patients had simple, 976 (33.8%) moderate and 687 (23.8%) great complexity ACHD. The majority of patients were asymptomatic (New York Heart Association (NYHA) functional class I in 57.1%, II in 34.9% and III/IV in 8.0%).
Baseline parameters and outcome results in all patients and subgroups according to Bethesda classification of disease complexity
Supplementary information on patients by leading ACHD diagnosis
Albumin, total protein and liver dysfunction
Median albumin and protein concentration was 41.0 (38.0–44.0) and 70.0 (66.0–74.0), respectively (table 1). Overall, hypoalbuminaemia (<35 g/L) was present in 13.3% of patients and hypoproteinaemia (<60 g/L) in 8.0%. Hypoproteinaemia was almost always associated with hypoalbuminaemia, with only 0.38% of patients presenting with hypoproteinaemia but no hypoalbuminaemia. The prevalence of hypoalbuminaemia was significantly higher in patients with great complexity ACHD (18.2%) compared with patients with moderate (11.3%) or simple ACHD (12.1%, p<0.001). Hypoalbuminaemia was most common in patients with Eisenmenger syndrome (26.6%) and the complex ACHD subgroup (single-ventricle physiology without evidence of pulmonary hypertension, 18.6%) and lowest in patients with aortic coarctation (9.0%, p<0.001 for comparison across diagnostic groups, figure 1). In contrast, there was no significant difference in the prevalence of hypoproteinaemia between subgroups of disease severity (great complexity ACHD 7.1%, moderate 8.0%, simple ACHD 8.5%, p=0.57).

Prevalence of hypoalbuminaemia by adult congenital heart disease (ACHD) diagnosis. Bar width is in proportion to the number of patients in each group. Whiskers represent the SE of the prevalence estimate. CCTGA, congenitally corrected transposition of the great arteries; TGA, transposition of the great arteries.
Abnormal AST (>34 U/L) or ALT (>40 U/L), suggestive of liver dysfunction, was encountered in 10.4% of patients. Only 17.5% of patients with hypoalbuminaemia had elevated AST or ALT, whereas 74% of patients with elevated AST or ALT had both normal serum albumin and protein.
Mortality and predictors of outcome
During a median follow-up of 5.7 years (cumulative follow-up time of 18 503 patient-years), 327 (11.3%) patients died. On Kaplan–Meier statistics, 1-year, 5-year and 10-year mortality for the entire study population was 2.8% (95% CI 2.2% to 3.4%), 8.1% (95% CI 7.1% to 9.2%) and 15.9% (95% CI 14.1% to 17.7%), respectively. Overall mortality was significantly higher compared with age-matched and gender-matched UK population (standardised mortality ratio 4.03, 95% 3.56 to 4.56, p<0.001). Within the study period, 2886 patients had at least one measurement of serum albumin, while 2292 patients, being 44% of all patients attending the outpatient clinic in the study period, had no serum albumin assessment. Patients with ‘simple ACHD’ in whom albumin had been assessed during the study period had a higher mortality on multivariable Cox regression analysis (including age and functional class) compared with those with no albumin assessment (HR 1.68, 95% CI 1.08 to 2.64, p=0.023). However, this was not true for patients with ACHD with moderate disease complexity (HR 1.50, 95% CI 0.81 to 2.80, p=0.2) or high-disease complexity (HR 1.85, 95% CI 0.93 to 3.67, p=0.08).
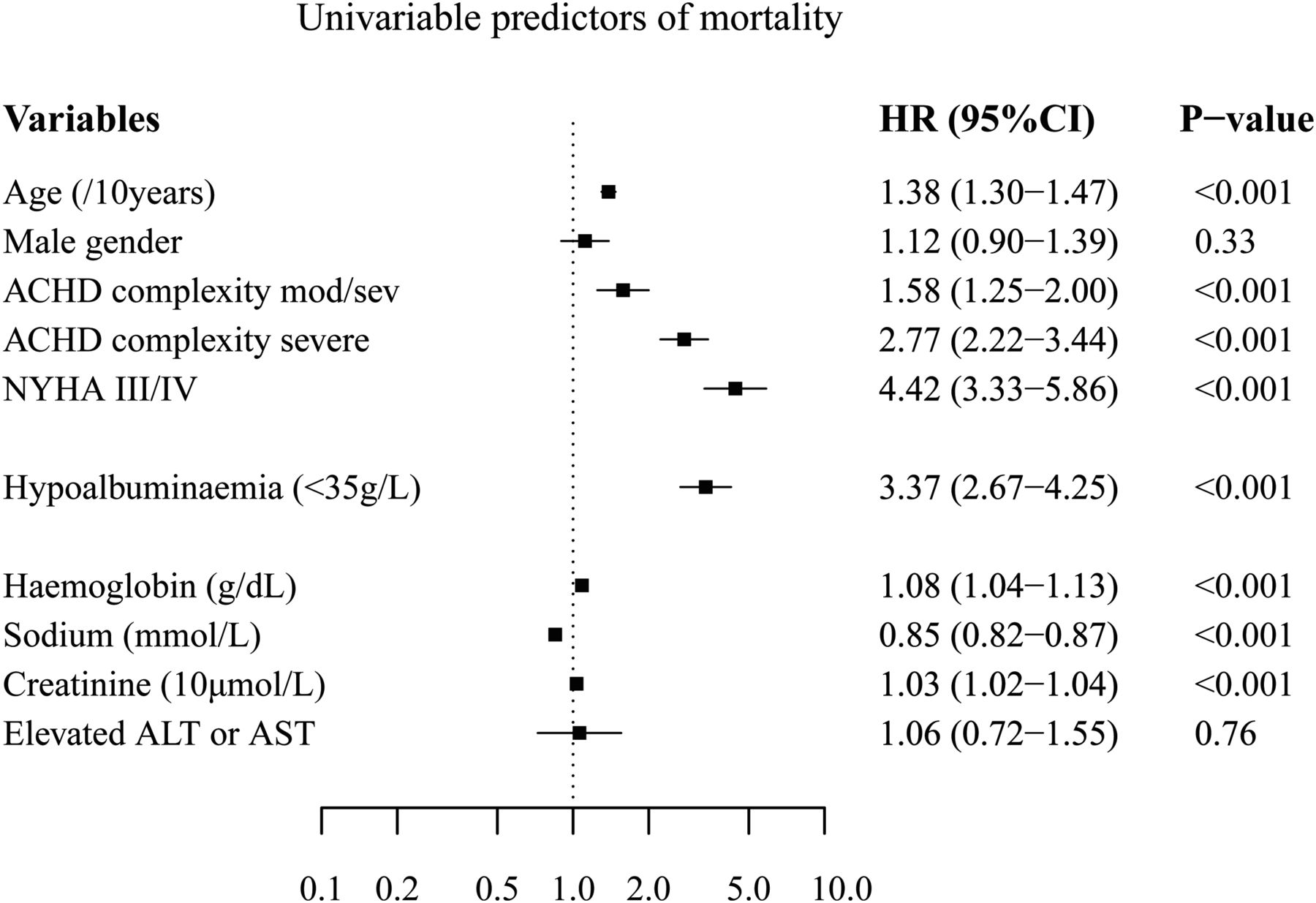
On univariable Cox regression analysis, hypoalbuminaemia (serum albumin <35 g/L) was related to a more than threefold increased risk of death (HR 3.37, 95% CI 2.67 to 4.25, p<0.001; figures 2 and 3). A twofold increased risk of death was also identified for patients with hypoproteinaemia (HR 2.24, 95% CI 1.66 to 3.01, p<0.001). When albumin was analysed as a continuous variable, a twofold increase in risk was identified for each 10 g/L decrease in albumin concentration (HR 2.08, 95% CI 1.82 to 2.38, p<0.001). As a sensitivity analysis, using multiple values of albumin over time in a repeated-measures Cox regression model, albumin remained a strong predictor of outcome as well (HR 2.26 per 10 g/L decrease, 95% CI 1.97 to 2.60, p<0.001).

Kaplan–Meier survival curves in patients with adult congenital heart disease by serum albumin. The numbers bellow the horizontal axis represent the number of patients at risk.

Results of univariable Cox proportional hazard regression analysis for overall mortality. ACHD, adult congenital heart disease; ALT, alanine transaminase; AST, aspartate transaminase; NYHA, New York Heart Association.
Threshold analysis revealed no clear cut-off for albumin in relation to mortality, with decreasing albumin levels associated with an ever-increasing risk of death (figure 4). Hypoalbuminaemia was a strong predictor of outcome in each of the three groups of diagnostic severity: HR 2.29, 95% CI 1.45 to 3.60 for simple ACHD; HR 3.66, 95% CI 2.21 to 6.05 for moderate ACHD; HR 3.51, 95% CI 2.83 to 4.87 for great complexity ACHD, p<0.001 for all.

Threshold analysis for plasma albumin presented as functional form of the unadjusted relationship between plasma albumin concentration and the hazard of death and 95% CIs using smoothing splines.
Several other variables emerged as predictors of death (figure 3), including older age, higher ACHD complexity and higher functional class. Other biochemical parameters related to mortality included hyponatraemia and a high serum creatinine. In contrast, liver dysfunction was not predictive of outcome. On a bivariate analysis, including hypoalbuminaemia and hypoproteinaemia, only hypoalbuminaemia remained in the model, suggesting a stronger relationship of hypoalbuminaemia to outcome than hypoproteinaemia. On multivariable Cox regression analysis, including all univariable predictors, hypoalbuminaemia remained in the model with age, functional class, creatinine and sodium concentration (HR for hypoalbuminaemia 1.96, 95% CI 1.48 to 2.59, p<0.001). The same was true for albumin used as a continuous variable (HR 1.61 per 10 g/L decrease of albumin, 95% CI 1.33 to 1.95, p<0.001). As a sensitivity analysis, in order to exclude any effect of inflammation or haemodilution on the relation between albumin and mortality, all albumin values associated with a CRP >20 mg/dL or white blood cells count >107/mL as well as values measured within 2 weeks of surgery or percutaneous cardiac intervention were excluded and the multivariable analysis was repeated. Albumin remained a significant predictor of mortality (HR 1.96 per 10 g/L decrease of albumin, 95% CI 1.56 to 2.47, p<0.001). When the multivariable analysis was repeated considering each ACHD complexity subgroup separately, albumin was a significant independent predictor of death in patients with moderate or great ACHD complexity, while a trend was present for simple ACHD (p=0.063).
Predictors of hypoalbuminaemia
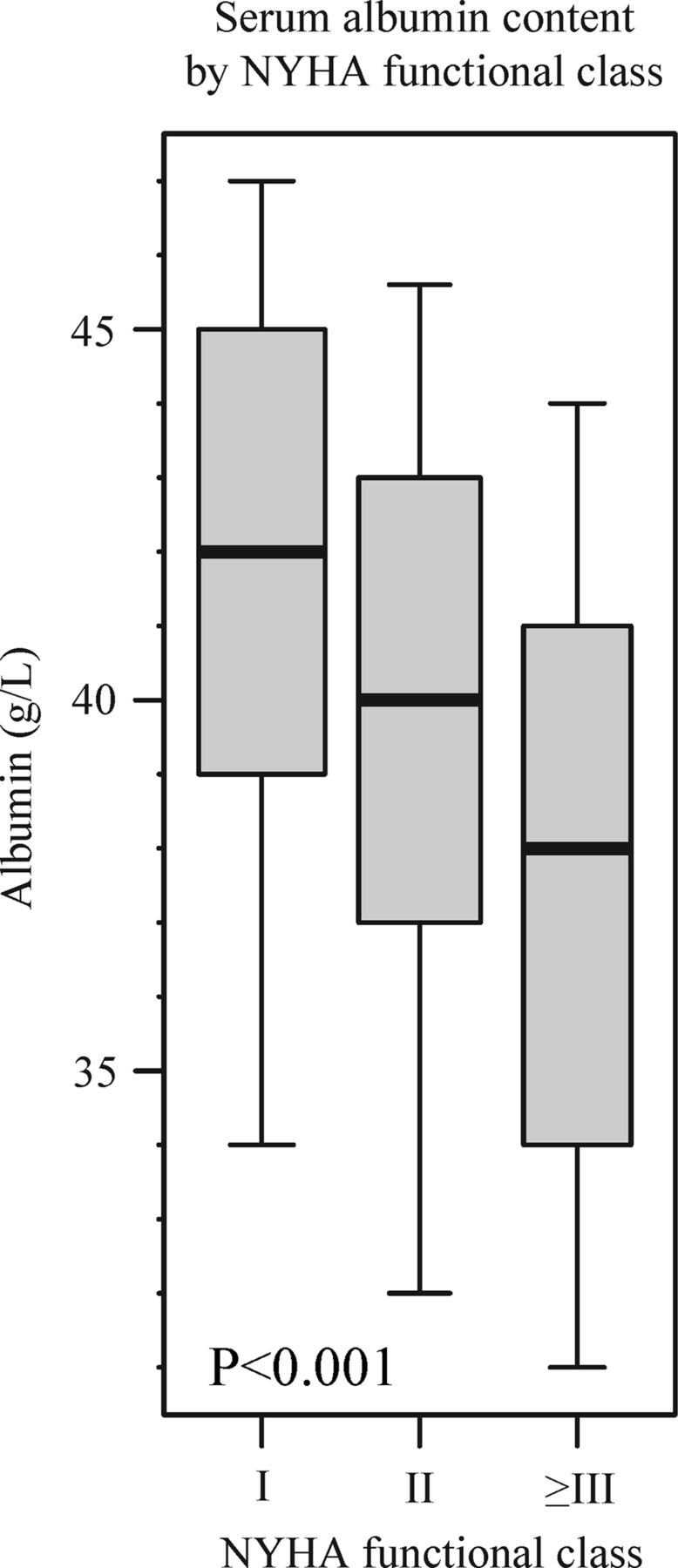
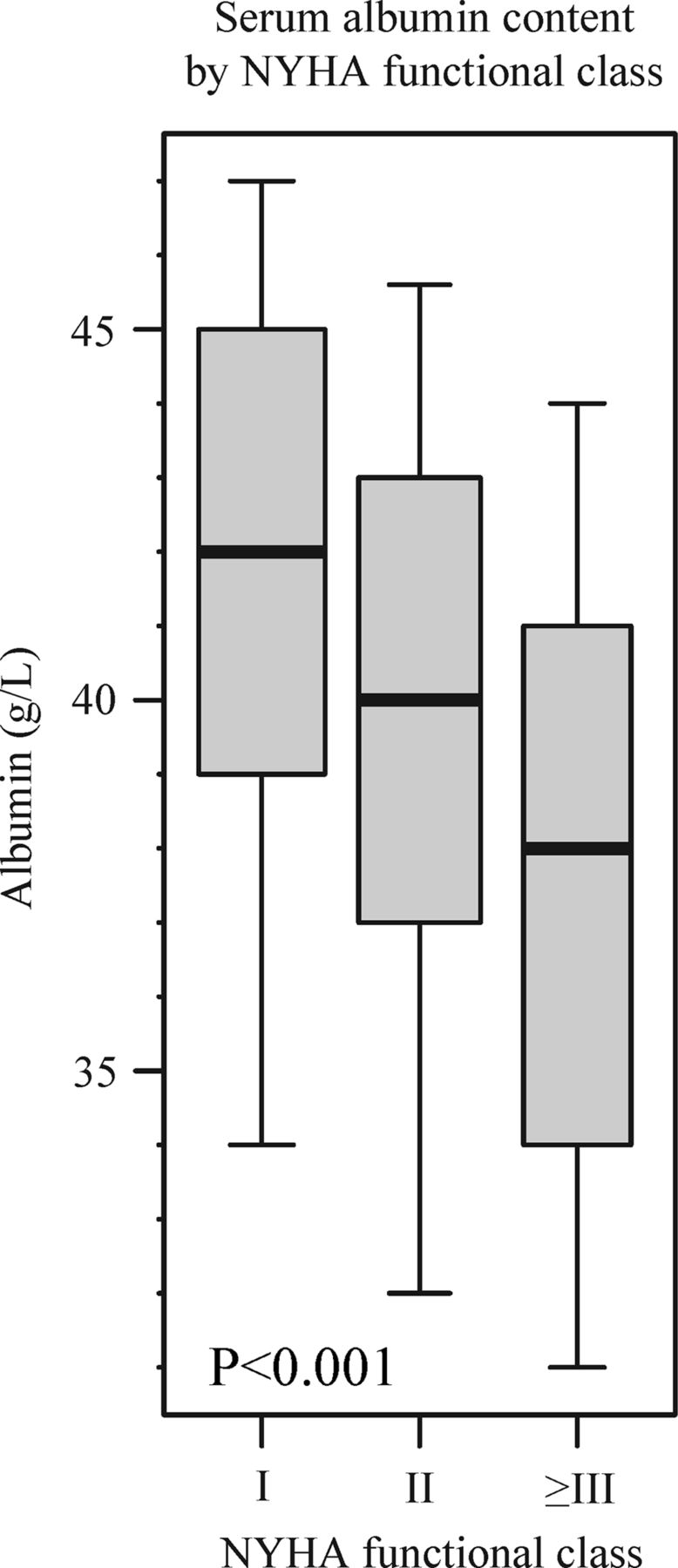
On univariable logistic regression analysis, several variables emerged as significant risk factors for hypoalbuminaemia (figure 5). These included age (OR 1.11 per 10 years, 95% CI 1.04 to 1.19, p=0.003), complex ACHD (OR 1.67, 95% CI 1.33 to 2.11, p<0.001) and functional class (OR 2.42 for patients in NYHA III/IV, 95% CI 1.68 to 3.48, p<0.001, figure 6). Liver dysfunction (defined as elevated AST or ALT, OR 2.41, 95% CI 1.79 to 3.26, p<0.001) and renal dysfunction (defined as creatinine >120 µmol/L, OR 3.82, 95% CI 2.60 to 5.61, p<0.001) were also predictors of hypoalbuminaemia. On multivariable logistic regression including all univariable predictors, only functional class and presence of liver or renal dysfunction remained in the model. The abstract with the main results has been presented at the European Society of Cardiology Congress 2014 in Barcelona and has been printed in the congress abstract book.

Results of univariable logistic regression analysis for the presence of hypoalbuminaemia. Liver dysfunction is defined as elevated serum aspartate transaminase (>34 U/L) or alanine transaminase (>40 U/L); renal dysfunction is defined as serum creatinine >120 µmol/L. NYHA, New York Heart Association.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Distribution of serum albumin concentration by New York Heart Association (NYHA) functional class group. The box and whiskers represent the 10th, 25th, 50th, 75th and the 90th centile of serum albumin content. There is a significant difference in serum albumin concentration between groups (analysis of variance p<0.0001).
Discussion
Our study demonstrates for the first time that hypoalbuminaemia is common across the spectrum of ACHD and is a strong independent predictor of mortality. Increased awareness of this simple, often neglected risk factor may help to improve risk assessment in this expanding population of patients. Hypoalbuminaemia appeared to be a stronger predictor of outcome in patients with moderate to complex ACHD, who are at risk of adverse events and, thus, are more likely to benefit from accurate risk stratification algorithms.
The pathogenesis of hypoalbuminaemia in patients with ACHD
The aetiology of hypoalbuminaemia in ACHD is likely to be multifactorial. Hypoalbuminaemia has previously been reported in patients with both acute and chronic heart failure due to systolic or diastolic LV dysfunction, in the setting of acquired heart disease.9 ,10 Venous congestion is known to contribute to an increased transcapillary escape rate of albumin (TER), that is, the fraction of intravascular mass of albumin that passes to the extravascular space per unit of time. TER is significantly increased in patients with congestive heart failure and a raised central venous pressure, and the same is likely to be true in patients with ACHD.11 In fact, evidence of raised central venous pressure has been reported in various ACHD cohorts, including patients with Eisenmenger syndrome, Fontan circulation and tetralogy of Fallot.12 ,13 Surprisingly in our cohort, patients with a Fontan-type circulation, in whom central venous hypertension is the norm, had a relatively low prevalence of hypoalbuminaemia, suggesting that other mechanisms, beyond a high central venous pressure, are promoting hypoalbuminaemia.
Recent studies have shown that chronic systemic inflammation and endothelial dysfunction play an even more important role than venous congestion in promoting albumin loss to the extravascular space in acquired heart failure.14 Inflammation and endothelial dysfunction have been reported in various ACHD groups, including patients with repaired aortic coarctation, tetralogy of Fallot and single-ventricle physiology.15–17 In patients with Eisenmenger syndrome, the group with the highest prevalence of hypoalbuminaemia in our cohort, evidence of significant endothelial dysfunction and chronic, subclinical inflammation with CRP activation has been described recently and is likely to be contributing to increased vascular permeability with enhanced albumin catabolism.18 ,19
The association between hypoalbuminaemia and raised liver enzymes in our cohort also suggests a role for decreased albumin synthesis rates in its pathogenesis. However, the vast majority (82.5%) of patients presenting with hypoalbuminaemia had no evidence of liver dysfunction. In fact, primary liver dysfunction is rarely the sole reason for hypoalbuminaemia in the general population.20 Furthermore, patients with Fontan circulation, in whom both an increased hydrostatic venous pressure and an increased incidence of liver dysfunction are present,21 the prevalence of hypoalbuminaemia in our series was relatively low (9.1%) compared with other ACHD subgroups. This may suggest that endothelial dysfunction and chronic inflammation are stronger drivers for hypoalbuminaemia in the ACHD cohort than hepatic dysfunction or raised hydrostatic pressure.
Finally, hypoalbuminaemia may also be caused by albuminuria. A high prevalence of renal dysfunction has been described previously in patients with ACHD, especially those with more complex disease and those with Eisenmenger syndrome, in whom there is also a high prevalence of hypoalbuminaemia.2 Moreover, renal dysfunction was a strong independent predictor of hypoalbuminaemia in our cohort.
The association between hypoalbuminaemia and outcome
Hypoalbuminaemia likely relates to mortality in the ACHD population through various mechanisms. Preoperative hypoalbuminaemia is a recognised risk factor for perioperative mortality, infection, ventilator dependency and long-term mortality, both for cardiac and non-cardiac surgery.22–25 Many patients with ACHD require one or more surgeries during their lifetime, and hypoalbuminaemia contributes to perioperative morbidity and mortality. It has been proposed that this effect may be, at least in part, related to the high antioxidative properties of albumin.26 ,27 Moreover, hypoalbuminaemia is directly related to lower serum osmotic pressure28 and can promote peripheral and pulmonary congestion, which can be potentially lethal. However, it is more likely that hypoalbuminaemia is an indicator of multiorgan derangement, including cardiac, renal and liver disease, which are associated with a higher likelihood of adverse outcome. Moreover, low albumin levels may reflect generalised endothelial dysfunction, inflammation and possibly neurohormonal activation, which again adversely affect survival. Hypoalbuminaemia was a predictor of mortality independent of creatinine levels and sodium concentration, suggesting that it carries prognostic information beyond renal dysfunction or neurohormonal activation (an established driver for hyponatraemia in heart failure).
Clinical implications
ACHD physicians have in the past focused their attention on hypoalbuminaemia mainly in the setting of protein losing enteropathy in patients with a failing Fontan circulation.29 ,30 In the light of the present study, screening for hypoalbuminaemia should be included in the routine blood test panel of all patients with ACHD, not only those with more complex defects or significant symptoms. Patients with hypoalbuminaemia should be deemed at increased risk of death, and potential causes of hypoalbuminaemia should be examined. Hypoalbuminaemia in this setting is a robust, unifying parameter with sound pathophysiological background and should be an integral part of the decision making in this complex group of patients.
Limitations
This is a retrospective study performed in a single, large, tertiary adult congenital heart centre. The prevalence of hypoalbuminaemia in our study reflects the case-mix of patients with ACHD seen in a tertiary centre such as ours, with a high proportion of patients with moderate or severe lesions. Moreover, prevalence estimates are likely to be influenced by a referral bias, as not all patients with ACHD over the study period underwent blood sampling.
In fact, patients in whom albumin had not been assessed during the study period were less likely to present with hypoalbuminaemia, but also had lower mortality. This suggests that even though referral bias may have affected our estimates of the prevalence of hypoalbuminaemia, especially in patients with simple forms of ACHD, it is unlikely to have affected the strong prognostic value of hypoalbuminaemia reported in our study.
Neither ALT nor AST are optimal markers of liver dysfunction and liver imaging, or in selected cases biopsy, provide better insight into hepatic function.
Future, larger prospective studies are clearly warranted to further investigate the mechanisms linking hypoalbuminaemia to outcome in ACHD and its place in a holistic risk assessment algorithm in this unique and challenging group of patients.
Conclusions
Hypoalbuminaemia is common in patients with ACHD and is a strong, independent predictor of mortality associated with an over threefold increased risk of death. Plasma albumin concentration should be a part of the routine assessment of patients with ACHD, and unexplained hypoalbuminaemia, even in clinically stable and oligosymptomatic patients, should trigger appropriate measures to identify underlying causes of serum albumin imbalance, but more importantly lead to closer monitoring and measures aimed at improving prognosis.
Key messages
-
What is already known on this subject?
-
Risk stratification is essential in the management of adult patients with congenital heart disease (ACHD), and identification of parameters related to outcome is crucial. Hypoalbuminaemia has been reported in subgroups of patients with ACHD, but its prevalence and relation to mortality across the spectrum of patients with ACHD was unknown.
What might this study add?
-
Our study demonstrates that hypoalbuminaemia is common in patients with ACHD. The prevalence of hypoalbuminaemia is highest in patients with Eisenmenger syndrome (27%) and complex ACHD (19%). Surprisingly, however, the prevalence of hypoalbuminaemia in patients with Fontan circulation in our cohort was relatively low (9%). Hypoalbuminaemia was a strong predictor of mortality associated with a threefold increased risk of death, also after adjustment for disease complexity, functional class and other risk factors.
How might this impact on clinical practice?
-
This study facilitates interpretation of serum albumin status and risk stratification in patients with CHD. Patients identified with hypoalbuminaemia are at increased risk of death. They require, therefore, additional investigations to identify the reason for decreased serum albumin and, potentially, may benefit from intensified treatment to modulate their increased risk of mortality.
References
Footnotes
-
Contributors All authors have read and approved the manuscript. All authors have sufficiently contributed to conception and design of the study, analysis and interpretation of data, and drafting of the manuscript and revising it to justify authorship.
-
Funding AK has received unrestricted educational grant support from Actelion Global. MAG and the Adult Congenital Heart Centre and National Centre for Pulmonary Hypertension have received support from the British Heart Foundation. This project was supported by the NIHR Cardiovascular Biomedical Research Unit of Royal Brompton and Harefield NHS Foundation Trust and Imperial College London. This report is independent research by the National Institute for Health Research Biomedical Research Unit Funding Scheme.
-
Disclaimer The views expressed in this publication are those of the author(s) and not necessarily those of the NHS, the National Institute for Health Research or the Department of Health.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval This study was approved by the local research and development review board.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement We may provide, on request, additional analyses of our data.