Article Text

Abstract
Objective To determine the nature of the association between renal dysfunction and outcomes following transcatheter aortic valve implantation (TAVI) in all cases performed in the UK between 2007 and 2012.
Methods The UK TAVI registry was established to report outcomes on all TAVI procedures performed within the UK. Data were collected prospectively on 3980 patients from 1 January 2007 until 31 December 2012.
Results In total, 205 patients (5.5%) died during their admission. Moderate to advanced chronic kidney disease (CKD) (estimated glomerular filtration rate (eGFR) <45 mL/min/1.73 m2) was significantly associated with increased mortality, even after adjustment for risk factors (OR 1.45, 95% CI 1.03 to 2.05; p=0.04). For every 10 mL/min/1.73 m2 decrease in eGFR, in-hospital mortality increased by 8.2% (95% CI 1.1% to 14.7%; p=0.03). In total 1119 patients (30.2%) died during the follow-up period (median 543 days). Moderate to advanced CKD (eGFR <45 mL/min/1.73 m2) was significantly associated with increased mortality, even after adjustment for risk factors (OR 1.36, 95% CI 1.17 to 1.58; p<0.001). For every 10 mL/min/1.73 m2 decrease in eGFR, cumulative mortality increased by 4.4% (95% CI 1.2% to 7.5%; p=0.007). Preoperative kidney function and the need for preoperative dialysis treatment discriminated between patients who died and survived. However, predictive power was poor with none of the c-statistics being >0.6.
Conclusions Pre-procedural renal dysfunction is associated, in a graded fashion independently of dialysis status, with worse outcomes, including mortality in patients undergoing TAVI.
Statistics from Altmetric.com
Introduction
Transcatheter aortic valve implantation (TAVI) is now established as an alternative treatment to surgical aortic valve replacement (SAVR) for patients with severe symptomatic aortic stenosis at high risk from a surgical intervention. Factors such as advanced age, frailty, or high comorbidity are used routinely to identify patients for TAVI rather than SAVR.1 Worldwide the use of TAVI is accelerating as registry and trial data indicate good medium term outcomes; over 100 000 procedures have now been performed.2 Refining the selection of patients for whom TAVI is the most appropriate procedure is therefore a matter of importance and much remains to be learnt about factors predictive of outcomes. To date, the main pre-procedural variables identified as independent predictors of medium term mortality include male sex, low body mass index, aortic valve gradient, LV dysfunction, pulmonary disease, and prior vascular surgery.1 ,3
Chronic kidney disease (CKD) is associated with adverse health outcomes in multiple populations4 and after a variety of surgical and invasive procedures, including percutaneous coronary intervention,5 coronary bypass surgery6 and SAVR.7 Large scale outcome data examining the impact of CKD on outcomes after TAVI are still lacking and studies to date have been inconsistent. While some studies have found a relationship between renal dysfunction and worse outcomes,8 others have not.9 ,10 A recent study demonstrated that although advanced CKD was an independent risk factor for mortality, earlier stage disease was not. The study group contained only 201 patients with advanced CKD of whom 67 were on dialysis.11
We have used the UK TAVI registry to determine the nature of the association between CKD and outcomes following TAVI in all cases performed in the UK between 2007 and 2012.
Methods
The database
The TAVI steering group established a national audit registry for all TAVI procedures performed in the UK (1 January 2007–31 December 2012).12 Peri-procedural and post-procedural complications are self-reported according to definitions within the national dataset.1 Reliance is placed on local data entry and clinical staff to ensure data accuracy. Overall mortality is tracked using data from the Office of National Statistics linked using each patient's unique National Health Service number. This number is only provided for patients from England and Wales, and so for the small number of patients from Scotland, Northern Ireland and overseas, mortality tracking was not available. All of these processes were performed in compliance with current UK Data Protection and Information Governance legislation. All patients provided signed, informed consent.
Measures of renal function
The pre-procedure estimated estimated glomerular filtration rate (eGFR) was calculated using the Modification of Diet in Renal Disease (MDRD) equation with serum creatinine recalibrated to be traceable to an isotope-derived mass spectroscopy method.13 Patients were divided into five groups defined by their eGFR: ≥60 (CKD stages 1–2); 45–59 (CKD stage 3a); 30–44 (CKD stage 3b); 15–29 (CKD stage 4) and <15 mL/min/1.73 m2 or on dialysis (CKD stage 5) based on the widely used clinical classification.14 For analyses, CKD stages were also grouped as moderate-advanced CKD (stages 3b–5) and advanced CKD (stages 4–5). Dialysis patients were included in the analyses unless specified.
Year of procedure and non-transfemoral approach
A previous report from the UK TAVI Registry1 of cases performed between 2007 and 2009 highlighted that the early mortality rate was lower in patients undergoing TAVI in 2009 (4.3%) compared with the overall rate (7.1%), potentially as a result of the early learning curve. Because inclusion of cases in 2007–2008 could have skewed our results, the data were also analysed excluding these patients as a sensitivity analysis.
Studies have consistently shown that the transfemoral approach is associated with better outcomes than non-transfemoral approaches.15 Given that the decision-making process for the choice of approach is difficult to quantify objectively, mortality data were also analysed separately for patients who underwent a femoral or non-transfemoral approach.
Statistical analyses
All data were analysed using SPSS V.21.0 (SPSS Inc, Chicago, Illinois, USA). Continuous data are presented as median (IQR) and analysed using the Kruskal-Wallis test. Categorical data are presented as count (percentage) and analysed using the χ2 test. All the variables used in the analyses had <5% of the values missing and were therefore treated as missing completely at random with case-wise deletion. In multivariable analyses, all plausible confounders were entered into the model. Logistic regression analysis was used to assess the relationship between outcomes, including in-hospital mortality, and parameters under investigation and the results expressed as an OR with 95% CIs. Time-to-event data analysis for cumulative mortality was done using the Cox proportional hazards model and the results expressed as HR with 95% CI. The Kaplan-Meier survival curves were drawn to assess differences between groups for the time to an event data and comparisons made using the log-rank statistic. Receiver operating characteristic curve analysis was used to assess the ability of different CKD stages to discriminate between patients who died or survived over the duration of follow-up and is reported as the associated c-statistic. A value of p<0.05 was considered statistically significant.
Results
Patient characteristics
This study included 3980 patients who underwent TAVI between 1 January 2007 and 31 December 2012. Of these, 44 (1.1%) were excluded for not having dialysis status recorded preoperatively and 55 (1.4%) were excluded for not having a preoperative creatinine recorded but were documented as not being on dialysis. A further 217 (4.6%) patients were excluded for not having complete follow-up data, leaving 3696 (93%) patients included in the analysis. Of these, 1390 patients (37.6%) were classified as CKD stage 1–2, 1046 (28.3%) as CKD stage 3a, 846 (22.9%) as CKD stage 3b, 315 (8.5%) as CKD stage 4, and 99 (2.7%) as CKD stage 5, with 81 (2.2%) on dialysis. Analysing patients with CKD stages 1 and 2 separately made no appreciable difference to any of the results. The proportion of patients with advanced CKD in each year undergoing TAVI remained stable with 12.3% in 2007, 13.0% in 2008, 13.2% in 2009, 11.3% in 2010, 9.5% in 2011, and 11.1% in 2012 (p=0.3).
Baseline demographic characteristics and risk factors of the study population divided by CKD stages are presented in table 1. Patients with CKD stage 5 were younger, more likely to be male, more likely to have an LVEF <30%, and more likely to have an emergency or urgent TAVI procedure (p<0.001 for all). There was a graded relationship between worsening CKD stage and increasing risk profile as evaluated by the logistic EuroSCORE (European System for Cardiac Operative Risk Evaluation) (p<0.001).
Clinical and procedural characteristics of the study population according to preoperative renal function
In-hospital complications and mortality
The in-hospital outcomes for the cohort divided into CKD stages are shown in table 2. In total, 205 patients (5.5%) died before leaving hospital after the procedure. Patients with worse CKD stages were more likely to die in-hospital (p=0.001 for trend) and to require dialysis post-procedure (p<0.001 for trend). Patients with CKD stage 5 were more likely to require a platelet transfusion (7.1% vs 2.7%; p=0.02) and suffer a gastrointestinal bleed (5.1% vs 0.9%; p=0.003) than patients with better renal function.
In-hospital clinical outcomes and cumulative mortality in terms of preoperative renal function
The univariable and multivariable associations with in-hospital mortality are presented in table 3. CKD stage 4 was independently associated with in-hospital mortality. When CKD stages were grouped into moderate-advanced CKD and advanced CKD, both were independently associated with in-hospital mortality compared with the reference group of CKD stages 1–2. None of these associations was significantly affected by the exclusion of dialysis patients from the analyses. Lower eGFR as a continuous variable was associated with increased mortality, even after adjustment for risk factors. For every 10 mL/min/1.73 m2 decrease in eGFR, in-hospital mortality increased by 8.2% (95% CI 1.1% to 14.7%; p=0.03).
Logistic regression univariable and multivariable associations of in-hospital mortality
Overall cumulative mortality
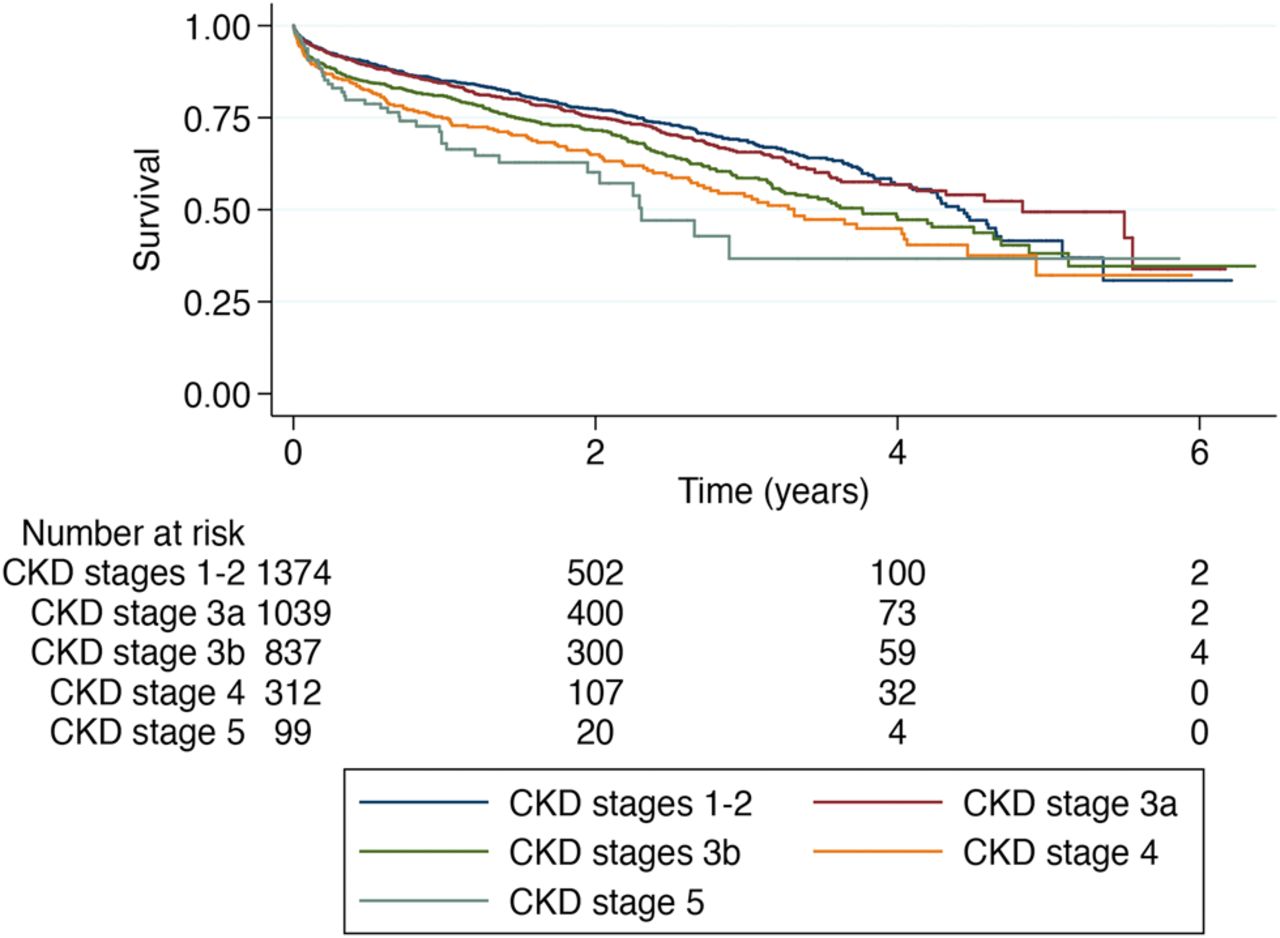
The median follow-up period was 543 (276–946) days. One thousand one hundred and nineteen patients (30.2%) died during the follow-up period. The proportion of patients dying during this period, as well as the 1–3 year mortality, increased with worsening CKD stage (table 2, figure 1).
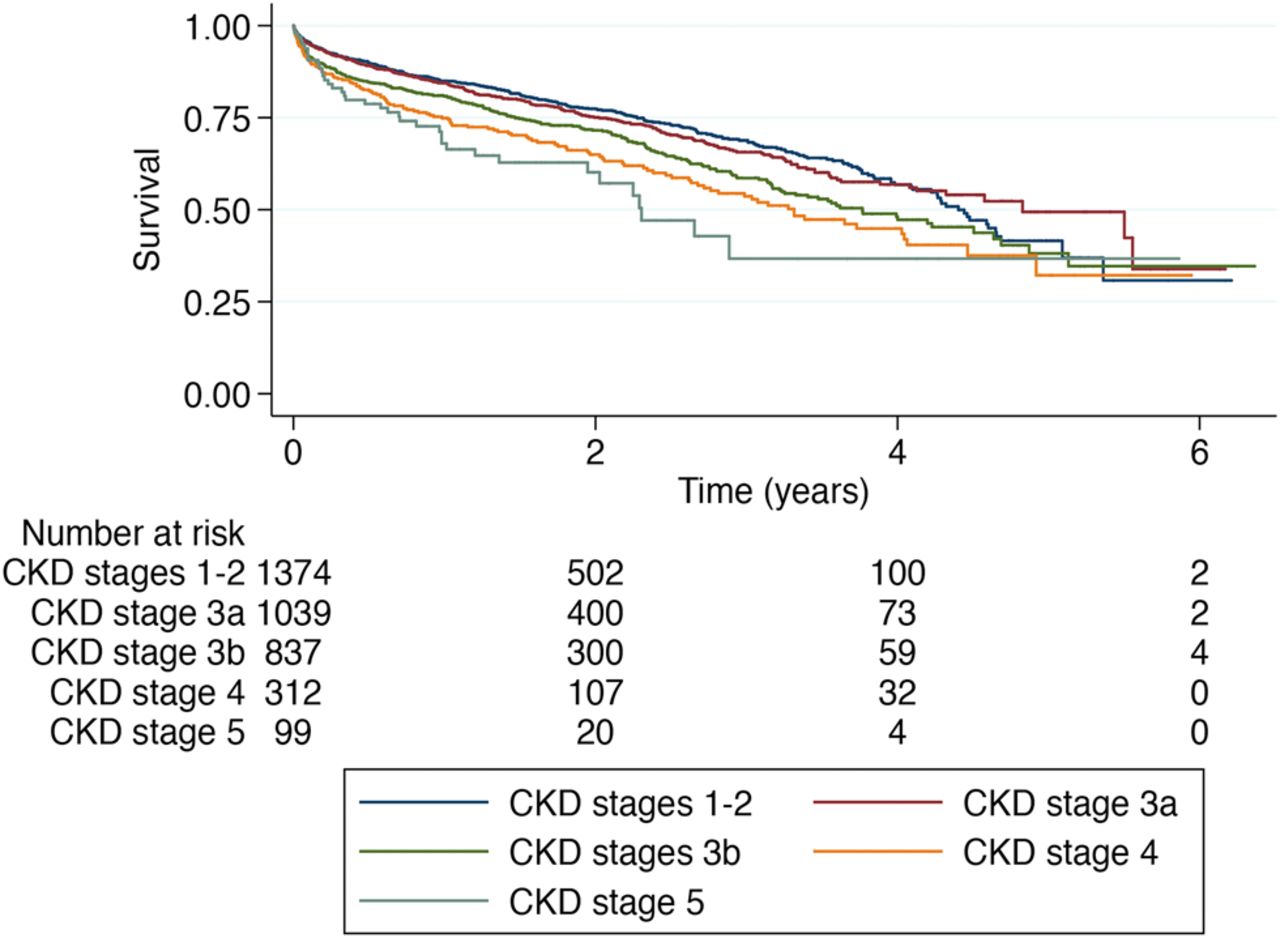
Kaplan-Meier curves for all-cause cumulative mortality. Study patients are divided according to the presence of chronic kidney disease (CKD) stages 1–2, 3a, 3b, 4 and 5.
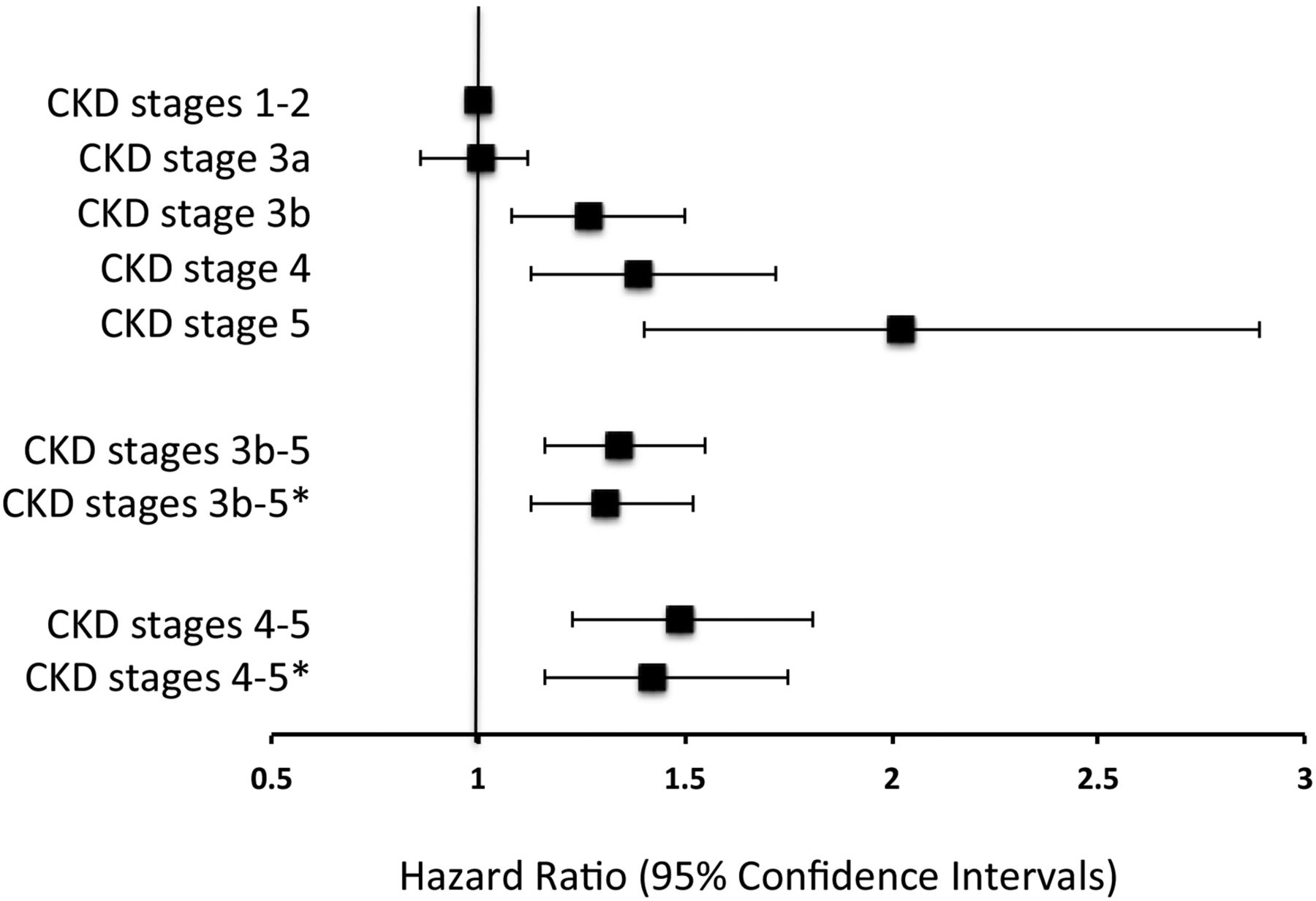
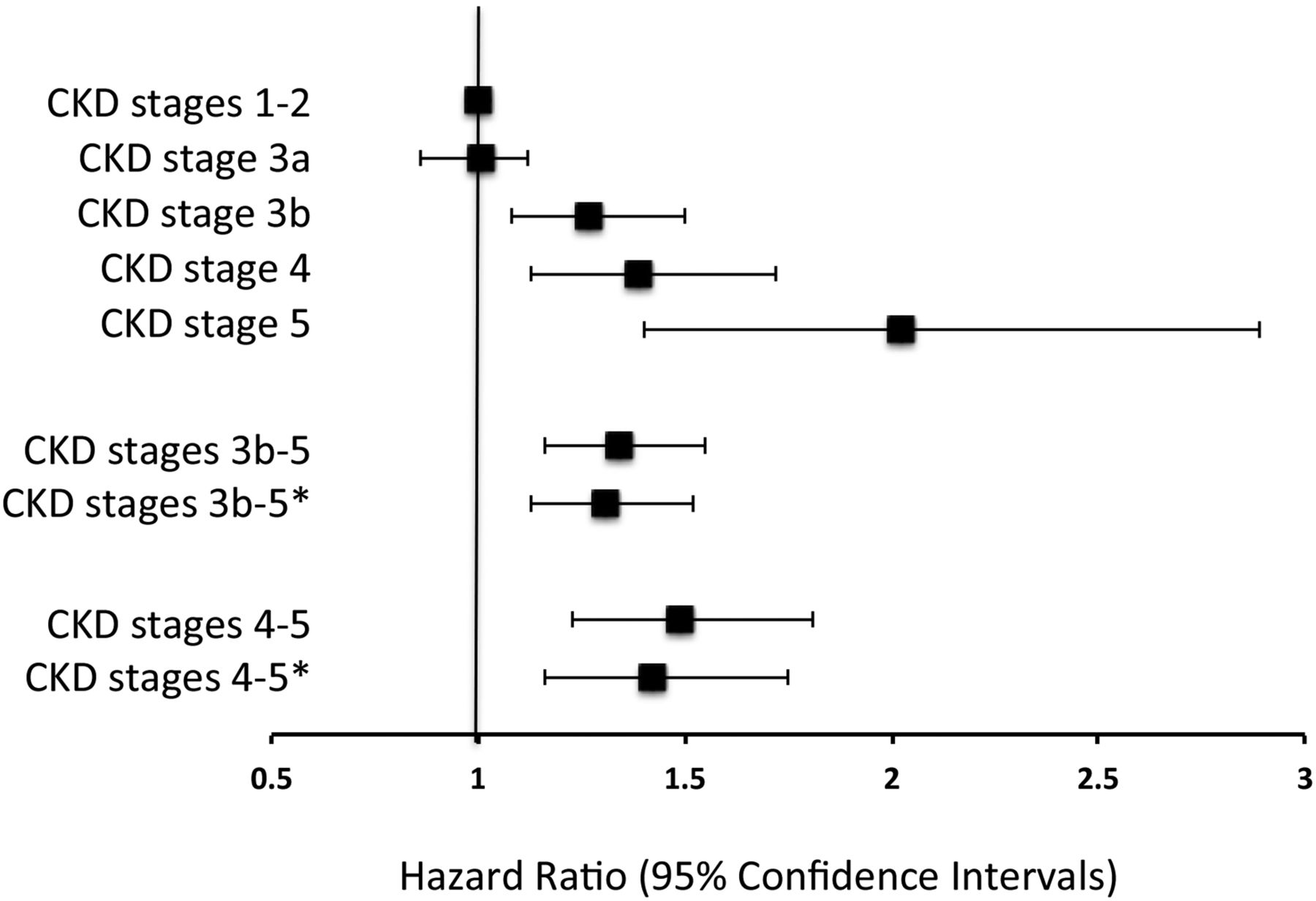
The univariable and multivariable associations with cumulative mortality are presented in table 4 and figure 2. CKD stage 3b, stage 4 and stage 5 were all independently associated with cumulative mortality. When CKD stages were grouped into moderate-advanced CKD and advanced CKD, both were independently associated with in-hospital mortality compared with the reference group of CKD stages 1–2. None of these associations was significantly affected by the exclusion of dialysis patients from the analyses. Lower eGFR as a continuous variable was associated with increased mortality, even after adjustment for risk factors. For every 10 mL/min/1.73 m2 decrease in eGFR, cumulative mortality increased by 4.4% (95% CI 1.2% to 7.5%; p=0.007). Censoring at 1, 2 or 3 years did not materially affect the results (see online supplementary tables S1–S3).
Cox regression univariable and multivariable associations with cumulative mortality
{kind=link}
{kind=link}
Adjusted HRs with 95% CIs for cumulative mortality according to chronic kidney disease (CKD) stages. *Dialysis patients excluded from the analysis. Values adjusted for gender, diabetes mellitus, chronic obstructive pulmonary disease, extracardiac arteriopathy, atrial fibrillation, previous cardiac surgery, body mass index, LVEF <30%, no coronary vessel with >50% stenosis, procedure urgency, aortic valve gradient, non-transfemoral approach, successful valve deployment.
Excluding patients who underwent TAVI before 2009 (see online supplementary table S4) a femoral or non-transfemoral approach separately did not significantly affect the results (see online supplementary tables S5 and S6).
Utility of CKD to identify likelihood of survival post-TAVI
Receiver-operating characteristic curves were constructed using the prospectively defined CKD stages and the results are presented in table 5. CKD stage cut-offs of 3a or worse, 3b or worse, and 4 or worse discriminated between patients who died and survived. However, they performed very poorly as predictors of mortality with neither the c-statistic nor the 95% CI being >0.6. These results were not significantly affected by the exclusion of dialysis patients or by censoring outcomes at 1, 2 or 3 years (see online supplementary tables S7–S9).
Discrimination C statistic of chronic kidney disease (CKD) stage cut-offs for cumulative mortality
Factors associated with increased mortality in patients with advanced CKD undergoing TAVI
After adjustment, only lower body mass index (HR 0.96, 95% CI 0.92 to 0.99; p=0.03) and higher logistic EuroSCOREs (HR 1.02, 95% CI 1.01 to 1.03; p<0.001) were associated with increased cumulative mortality (see online supplementary table S10). The results were very similar when outcome was censored at 1, 2 or 3 years (see online supplementary tables S11–S13), with the logistic EuroSCORE being the only factor associated with increased mortality in all the analyses. The top quartile of the logistic EuroSCORE discriminated between patients who died or survived overall (c-statistic 0.599, 95% CI 0.514 to 0.684; p=0.03) with similar values at 1, 2 and 3 year follow-up. Preoperative atrial fibrillation was not associated with mortality in any of the analyses and the need for pre-procedural dialysis was only associated with mortality at 3 years follow-up (HR 2.092, 95% CI 1.363 to 3.209; p=0.006).
Discussion
These data show that there is a graded inverse relationship between eGFR and both in-hospital and overall cumulative mortality in patients after TAVI that is independent of other risk factors. Despite this clear association, the presence of CKD performed poorly as a predictor of outcome with c-statistics of only a little over 0.5. This may be explained by the high prevalence of traditional cardiovascular risk factors among individuals with CKD and the already very high mortality risk of a predominantly elderly group of patients. This is perhaps already reflected in clinical practice. It is notable that patients undergoing TAVI with advanced CKD were younger and more likely to undergo an urgent or emergency operation, reflecting possible current reluctance to offer TAVI to elderly frail patients with advanced CKD, particularly if dialysis dependent. Data from the UK Renal Registry show that the median survival of patients aged over 75 years starting dialysis is 2.4 years.16
Our results illustrate well the current problems that clinicians encounter when attempting to select patients for TAVI, a life prolonging but moderately risky and invasive procedure. Many patients who undergo assessment are elderly with multiple comorbid conditions, and knowledge of predictors of positive outcomes, or equally of futility, is urgently required. Currently, there are no accurate predictors of an adverse outcome and our data indicate that the use of eGFR or dialysis status—important markers of risk in many conditions—may be useful aids in these situations but should not be used in isolation.
Renal dysfunction and survival post-procedure in other studies
Data on renal function before SAVR are extensive but have been examined in less detail, with some studies showing decreased survival with advanced CKD9 ,17 and others suggesting renal function has little effect on mortality.7 ,18 However, a recent systematic review has highlighted that both in-hospital and longer term mortality is very high among dialysis patients undergoing any type of surgical valve replacement.19 Previous studies looking at outcomes after TAVI with respect to renal function have produced inconsistent results. Studies with limited power have found no independent association between eGFR and short term outcomes.8 ,9 More recently, a study from two French centres showed that in 642 patients undergoing TAVI, CKD stage 4 was independently associated with an increased risk of 30 day mortality and stages 3b and 4 with increased mortality at 1 year.20 Patients with stage 5 CKD were excluded from the analysis. Close examination of the data from this study, however, suggests a graded inverse association between eGFR and risk, not dissimilar to the findings of the present study.
A recent report by Allende et al11 of 2075 TAVI procedures performed over 7 years in nine centres between 2005 and 2012 described the association between baseline eGFR and outcomes. Patients with advanced CKD had higher rates of mortality mainly due to increased cardiovascular mortality in the CKD stage 4 group and non-cardiovascular mortality in the CKD stage 5 group which included dialysis dependent patients. Advanced CKD was independently associated with 30 day bleeding rates and late mortality. The results of this study are broadly in agreement with the results reported here, including the increased risk of bleeding postoperatively in patients with advanced CKD for potential reasons recently reviewed.21 However, there are a few notable differences. While we found that the highest rates of in-hospital and overall cumulative mortality were in patients with advanced CKD, we have demonstrated that patients with CKD stage 3b also have an increased mortality. Furthermore, the association between mortality and CKD stages in our study persisted even after exclusion of dialysis patients, with little change in the OR or HRs. The analysis by Allende et al did not examine the relationship between eGFR as a continuous variable and outcomes, and did not examine the utility of eGFR as an independent predictor of mortality, but their data do not exclude a graded relationship at all stages of CKD as we have found. The report by Allende et al also suggested that the combination of preoperative dialysis and atrial fibrillation in patients with advanced CKD was associated with very poor outcomes after TAVI, with all patients with this combination being dead at 2 years post-procedure. However, there were only 17 patients in this group. We could not replicate these findings in our larger study. The reasons for this are not immediately obvious but may reflect different patient selection procedures as well as chance, given the low numbers involved.
Why is renal dysfunction associated with worse outcomes?
The reasons for the association of CKD with adverse outcomes after invasive and surgical procedures are not fully understood. In the general population, eGFR is independently associated with cardiovascular risk and mortality.4 However, while CKD is associated with a clustering of conventional risk factors for atheromatous disease (hypertension, diabetes, inflammation), epidemiological information obtained from studies of patients with advanced CKD suggests that most of the associated cardiovascular mortality is due to sudden cardiac death and heart failure rather than occlusive coronary events such as myocardial infarction.22 Combined with the near universal prevalence of LV fibrosis (and hypertrophy in late stage disease) this has led to the widespread belief that the increased cardiovascular mortality in CKD is predominantly a result of myocardial disease rather than atherosclerotic vascular disease.22 Thus, reduced LV systolic and diastolic function are both factors worthy of further study. Further research is required in patients after TAVI to define the precise causes of the excess mortality in patients with CKD. At the moment, it is unclear whether the increased death rates are due to cardiovascular disease or to other factors associated with CKD. Unfortunately, data on the causes of death are currently not available for this cohort.
Study strengths and weaknesses
The main strengths of this study are the inclusion of all consecutive patients treated in the UK. The UK TAVI Registry is unique in that it has captured every TAVI performed within the UK, and thus includes the entire ‘learning curve’ and early experience of adopting centres without any publication bias that might be induced by centre selection. Interestingly, excluding the first 2 years of data made no appreciable difference to the results, suggesting the association of renal function and outcomes is not affected by the ‘learning curve’. Equally, the association between renal function and outcome is independent of the chosen procedure approach. This data collection shares the weaknesses of other national registry programmes. There is a balance between the size of the dataset and the ability and/or willingness to collect it accurately. Also—apart from data on mortality, and later clinical and quality-of-life, including geriatric functional parameters—follow-up is limited. However, by using the Office of National Statistics to record mortality we ensured that all deaths, whether in or out of hospital, were captured. We investigated estimated rather than measured GFR in this study, and while this was (and will likely remain) a practical necessity we acknowledge the imperfection of the estimated measure. The use of other measures of eGFR, such as those based on cystatin C, may be helpful in future work. Like in all observational studies, it is possible that residual confounding by unmeasured variables exists.
Conclusions
Pre-procedural renal dysfunction is associated with worse outcomes, including mortality, in patients undergoing TAVI. The relationship between eGFR and outcomes is graded and present at all stages of CKD, independent of dialysis status. We were unable to define a clear cut-off for renal dysfunction at which worse outcomes could be predicted. Our data do not support the use of any CKD stage as a reliable discriminator to help select patients for TAVI, but do support taking eGFR into account in the selection procedure.
Key messages
-
What is already known on this subject?
-
Transcatheter aortic valve implantation (TAVI) is now an established treatment for high risk patients with severe symptomatic aortic stenosis. Outcome data examining the impact of renal dysfunction on outcomes after TAVI have been inconsistent. While some studies have found a relationship between renal dysfunction and worse outcomes, others have not.
What might this study add?
-
Lower estimated glomerular filtration rate (eGFR) is associated with adverse outcomes after TAVI, even after adjustment for other risk factors. For every 10 mL/min/1.73 m2 decrease in eGFR, in-hospital mortality increased by 8.2% (95% CI 1.1% to 14.7%; p=0.03) and overall cumulative mortality increased by 4.4% (95% CI 1.2% to 7.5%; p=0.007).
How might this impact on clinical practice?
-
Our data do not support the use of any cut-off of renal function as a reliable discriminator to help select patients for TAVI, but do support taking renal function into account in the selection procedure.
Acknowledgments
We gratefully acknowledge all of the hospital teams that have complied with the national audit programme and collected data on their patients. We also acknowledge the contributions made by the members of the UK TAVI Steering Group, Data Management Group, Dataset Group, and Clinical Research Group.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Contributors CJF, PL and JNT conceived and designed the study. CJF and CDC analysed the data. CJF and JNT drafted the first manuscript. All authors critically revised the manuscript and have approved the final version.
-
Funding This work is produced by CJF under the terms of a National Institute for Health Research training fellowship issued by the National Institute for Health Research.
-
Competing interests NM is a proctor and consultant to Medtronic. JNT has received educational support and training from Edwards.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Patient consent Obtained.