Article Text

Abstract
Objectives In the general population, planned caesarean section is thought to be safer in high-risk situations as it avoids the greater risk of an emergency caesarean section. Only limited data exist on the optimal mode of delivery in women with structural heart disease. We investigated the relationship between mode of delivery and pregnancy outcome in women with pre-existing heart disease.
Methods The Registry on Pregnancy and Cardiac Disease is an on-going, global, prospective observational registry of women with structural heart disease. We report on 1262 deliveries, between January 2007 and June 2011.
Results The caesarean section was planned in 393 women (31%): 172 (44%) for cardiac and 221 (56%) for obstetric reasons of whom 53 delivered by emergency caesarean section. Vaginal delivery was planned in 869 (69%) women, of whom 726 (84%) actually delivered vaginally and 143 (16%) had an emergency caesarean section. Perinatal mortality(1.1 vs 2.7, p=0.14) and low apgar score (11.9 vs 10.1, p=0.45) were not significantly different in women who had a caesarean section or vaginal delivery; gestational age(37 vs 38 weeks p=0.003) and birth weight (3073 vs 2870 g p<0.001) were lower in women delivered by caesarean section compared with women delivered by vaginal delivery. In those delivered by elective or emergency caesarean section, there was no difference in maternal mortality (1.8% vs 1.5%, p=1.0), postpartum heart failure (8.8% vs 8.2% p=0.79) or haemorrhage (6.2% vs 5.1% p=0.61).
Conclusions These data suggest that planned caesarean section does not confer any advantage over planned vaginal delivery, in terms of maternal outcome, but is associated with an adverse fetal outcome.
- VALVULAR DISEASE
- MYOCARDIAL ISCHAEMIA AND INFARCTION (IHD)
- MYOCARDIAL DISEASE
- CONGENITAL HEART DISEASE
Statistics from Altmetric.com
Introduction
The reported use of caesarean section in patients with heart disease varies from 21% to 55% in different registries and studies.1–7 Clinical (practice) guidelines are largely based on expert opinion, which broadly states that vaginal delivery is preferred in women with an adequate cardiac output, but caesarean section may be a better option in selected high-risk patients.8 European guidelines on pregnancy and heart disease recommend caesarean section in women on oral anticoagulants in preterm labour, patients with Marfan syndrome and an aortic diameter >45 mm, patients with acute or chronic aortic dissection and in those with acute intractable heart failure. Caesarean delivery may also be considered in patients with Marfan syndrome and with an aortic diameter larger than 40 mm.8 For all other patients, vaginal delivery with an effective epidural is the preferred method, as it is held to cause fewer and less dramatic changes in haemodynamic parameters and is known to be associated with lower risks of maternal complications such as haemorrhage, infection and thrombosis.9 Despite this, caesarean section rates are much higher in women with heart disease than in the normal population,1 ,2 probably because clinicians are worried about the greater risks of an emergency caesarean section. Indeed, the overall caesarean section rate in women without heart disease varies widely between different countries, suggesting that attitudes towards mode of delivery vary widely.10 We aimed to determine the relationship between mode of delivery and pregnancy outcome in women with pre-existing heart disease selected from various parts of the world.
Methods
Study design
In 2007, the European Registry on Pregnancy and Heart Disease was established as a part of the Euro Heart Survey Program of the European Society of Cardiology (now EURObservational Research Programme) which is an ongoing global registry. All patients with structural (valvular, congenital or cardiomyopathy) or ischaemic heart disease were eligible for enrolment. The prospective registry started in January 2008, but patients who were pregnant in 2007 could be included retrospectively, if the complete data of these patients were available. Data that were collected until 1 June 2011 served as the basis for this manuscript. A total of 60 hospitals in 28 countries enrolled 1321 pregnant women with structural heart disease. Data on the mode of delivery were available for 1262 (96%) patients.
Data
The study protocol and the first results of this registry were published previously.11 Information on delivery included place of delivery, intended mode of delivery (planned mode of delivery), performed mode of delivery, reason for caesarean section, start of labour, rupture of membranes and complications during delivery.
Endpoints for this study were maternal mortality, postpartum heart failure, postpartum haemorrhage (vaginal delivery>500 mL, caesarean section>1000 mL or requiring transfusion), perinatal mortality (all fetal death >22 weeks of gestation or >500 g, including death around delivery), neonatal mortality (all neonatal death <30 days postpartum), gestation length, the occurrence of premature labour (spontaneous onset of labour <37 weeks gestation) and birth weight.
Statistical methods
Categorical data are presented as frequencies (numbers) and percentages. One-sample Kolmogorov–Smirnov tests and histograms were used to check the normality of continuous data. Normally distributed continuous data are presented as mean values±one SD, whereas data that were not normally distributed were presented as medians with IQR. Differences in categorical data between independent patient groups were compared by χ2 tests. Fisher's exact tests were applied if any expected cell count was <5 (a Monte Carlo approximation was used if more than two independent groups were involved). Differences in continuous data between independent patient groups were compared by Student t tests.
We stratified the patients into four risk groups using a modified WHO risk classification for pregnancy in women with cardiac disease. In this risk stratification model, the patients are allocated to a score according to the diagnosis and severity of the disease. A WHO category 1 indicates low risk, WHO category 2 indicates intermediate risk, WHO category 3 indicates high risk and WHO category 4 indicates a contraindication for pregnancy.8 ,12 To calculate corrected birth weight and its association with mode of delivery, linear regression analysis was used. This analysis was adjusted for gestational age, smoking, fetal sex, maternal age, diabetes and pre-eclamptic toxaemia (PET), as these are known confounders from the literature.
Matching
Matched sample analysis with propensity scoring was performed to study the relationship between performed mode of delivery and adverse outcome. We selected factors including nulliparity, mechanical valves, medication use during pregnancy, WHO category and New York Heart Association (NYHA) class which were expected to influence pregnancy outcome and created a propensity score for women who delivered by vaginal delivery or by caesarean section. Women who had a vaginal delivery were than matched with women who delivered by caesarean section based on their propensity score in addition to specific diagnosis. We accepted a maximal difference of 0.30 points on a range of −1 to 1. We were able to define 447 matched pairs. We used these data to identify the adverse outcomes associated with a particular mode of delivery. The outcome in propensity matched patients was compared with paired analyses (such as the McNemar test and the paired student t test).
All statistical analyses were performed using SPSS V.21.0 (SPSS, Chicago, USA). Unless specified otherwise, p values <0.05 (two-sided test) were considered statistically significant.
Result
Baseline characteristics
Information on the mode of delivery was available in 1262 women. Median maternal age was 30 years (SD 5.6, range 16–53). Half of the women have had one or more previous pregnancies. The baseline characteristics are shown in table 1. At baseline, in the planned caesarean section group, fewer women were nulliparous, with lower rates of previous cardiac intervention and coronary heart disease, but higher rates of cardiomyopathy. Women taking anticoagulants were more, and overall, the planned caesarean section group had a worse NYHA score. The distribution of WHO categories varied widely between the planned modes of delivery as is shown in table 1. A larger number of high-risk patients were planned for a caesarean section (p<0.001, table 1), especially in patients planned for caesarean section for a cardiac reason who had the highest rate (WHO 3 was 11% in the cardiac caesarean section vs 2.3% in the obstetric caesarean section, p<0.010).
Baseline characteristics and outcome in patients with: (A) Planned vaginal delivery versus planned caesarean section; (B) Planned caesarean section for obstetric reasons versus planned caesarean section for cardiac reasons
Mode of delivery
Vaginal delivery was planned in 69% (869) and caesarean section was planned in 31% (393) as shown in figure 1. Of patients planned for caesarean section, 14% (53) delivered by emergency caesarean section of which 47% (25) were for cardiac reasons (heart failure, n=13; acute coronary syndrome, n=1; arrhythmia, n=5 and ischaemic cerebral event, n=1; specific indication not stated, n=5) and 53% (28) were for obstetric reasons. We had no information about the place of delivery in 7.5% (99 patients). Two-third (864 patients) of the patients delivered in a tertiary centre, 27% (361 patients) delivered in regional centres and 0.5% (7 patients) delivered at home.

Flowchart: Mode of delivery. CS, caesarean section.
Outcome related to planned mode of delivery
The outcomes of the planned vaginal delivery and planned caesarean section are shown in table 1A. In terms of outcome, the planned caesarean section group had higher rates of maternal death, 2% versus 0.6% (p=0.018), postpartum heart failure, 8.4% versus 3.9% (p<0.001) and PET, 5.9% versus 2.3% (p=0.001). Fetal outcome was better in the patients who had a planned vaginal delivery, with longer pregnancy duration (p<0.001) and higher birth weight (p<0.001; table 1) even after correction (p=0.013).
Outcome related to indication for caesarean section
The outcomes of the cardiac and obstetric planned caesarean sections are shown in table 1B. At baseline, in the cardiac planned caesarean section, there are more cases of valvular heart disease, and cardiomyopathy, with worse overall NYHA score and greater anticoagulant use. In terms of outcome, the cardiac indicated caesarean section had greater maternal mortality (4.7% vs 0% (p<0.001)), but similar rates of postpartum heart failure and haemorrhage. Perinatal and neonatal mortality and birth weight were similar, but gestational age at delivery was greater in patients who had a planned caesarean section for obstetric reasons (p=0.020).
Outcome related to type of caesarean section performed: emergency versus elective caesarean section
We compared the outcome of elective and emergency caesarean section in all patients and the subgroups with patient with obstetric caesarean section or the patients with cardiac caesarean section as shown in table 2. Of all groups, anticoagulation use was higher in the elective caesarean section group. Maternal outcome, including postpartum haemorrhage, was comparable. In terms of fetal outcome, pregnancy duration was shorter in the elective caesarean section group, but there was no difference in the corrected birth weight.
Both maternal and fetal outcomes compared between patients who had an elective caesarean section or an emergency caesarean section. (A) The group of patients who had a caesarean section; (B) patients who had a caesarean section for obstetric reasons and (C) patients who had a caesarean section for cardiac reasons
In the obstetric elective caesarean section group, there was a higher rate of PET. There was no difference in maternal outcome, but again pregnancy duration was shorter. More number of babies had a low Apgar score in the obstetric emergency caesarean section group than the obstetric elective caesarean section group.
In the cardiac group, the anticoagulation use was more in the elective caesarean section group, although this was not significant. There was no difference in maternal outcome, but in contrast to the obstetric elective caesarean section group, more number of babies had a low Apgar score in the cardiac elective caesarean section group.
In addition, we compared patients in the planned vaginal delivery group, who actually delivered by an emergency caesarean section, and patients who had a planned and performed elective caesarean section (table 3). There was no difference in the maternal and fetal outcomes. The difference in birth weight was lost after correction for confounders.
Both maternal and fetal outcomes compared between patients in the planned vaginal delivery group but delivered by emergency caesarean section and patients who had elective planned and performed caesarean section
Propensity matching (performed) caesarean section versus vaginal delivery
We were able to match 894 patients; all pairs had the same diagnosis and comparable propensity scores. The only difference in baseline variables was age 30 (caesarean section) versus 29 (vaginal delivery) years (p=0.004) and PET was more frequent in patients with caesarean section (5.6% in caesarean section vs 2.2% in vaginal delivery p=0.017). In addition, we found higher rates of postpartum heart failure rate in the caesarean section group (7.8% vs 4.3% p=0.023). There was a non-significant difference with higher perinatal mortality in women with vaginal delivery (1.1% in women who had a caesarean section vs 2.7% in women who had a vaginal delivery p=0.14). Neonatal outcome was worse in women who had a caesarean section, with lower birth weight (2879 vs 3073 g, p<0.001) and greater rates of preterm birth (23.3% in caesarean section vs 12.8% in vaginal delivery p<0.001, table 4).
Propensity matched analysis of performed vaginal delivery versus performed caesarean section
Variation in mode of delivery in different populations
There were large differences in mode of delivery for patients with heart disease between countries. For example, the rate of caesarean section was 56% for patients in Italy and 20% in the Netherlands. The results are displayed in figure 2. Overall, for women with heart disease, the caesarean section rate was 160% of the expected caesarean section rate in women without heart disease. In a univariate analysis, the caesarean section rate in women with heart disease appeared to be independent of the normal population caesarean section rate (r2=0.13 p=0.12, figure 3A), but depended on the proportion of patients with WHO category >2 (figure 3B). Using a multivariate analysis, we found that both normal caesarean section rate for the general population (p=0.015) and the proportion of patients with high WHO category (p=0.003) were predictors for caesarean section rate (with a combined r2=0.501 and p=0.004).
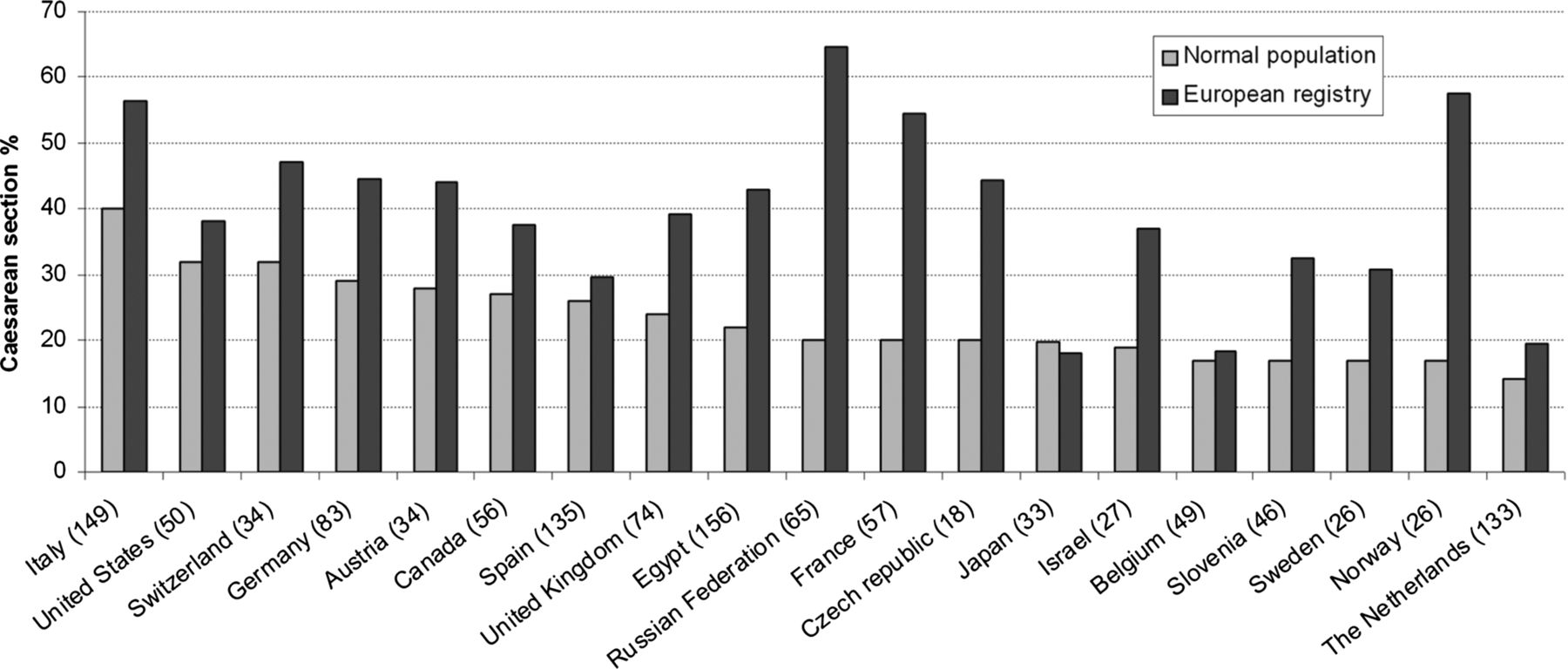
Percentage of caesarean sections performed in each country in the normal population (light bars) and those included in the Registry of Pregnancy and Cardiac disease (ROPAC) (dark bars). The numbers provided in parenthesis with the names of the countries indicate the number of patients included in the ROPAC registry in each country.

{kind=link}
{kind=link}
{kind=link}
Distribution of the number of caesarean sections performed in countries with their rates in the background population and in high risk patients. Every point represents a country; the size of the points corresponds to the number of subjects included. (A) Distribution of expected (normal) caesarean section rate against caesarean section rate in the Registry of Pregnancy and Cardiac disease (ROPAC). (B) Distribution of caesarean section rate (caesarean section rate in women included in the ROPAC registry divided by the caesarean section rate in the background population) compared with percentage of patients with WHO category 3 or WHO category 4.
Discussion
This is the first study, which investigates the relationship between the mode of delivery and pregnancy outcome in patients with cardiac abnormalities. Maternal outcome was similar when patients delivered by emergency caesarean section were compared with those delivered by elective caesarean section. These data suggest that a planned caesarean section confers no advantage in terms of maternal outcome, over a planned vaginal delivery in women with heart disease. A planned vaginal delivery was associated with a better neonatal outcome. These data suggests that in women with no specific indication for caesarean section, a trial of vaginal delivery is reasonable.
Study design
This study is primarily a hypothesis, as performing a randomised trial in this heterogeneous population may be very difficult and ethically challenging. Performing a prospective observational registry with matched patients is currently the best way to draw conclusions about the preferred mode of delivery. To date, the published observational studies have been relatively small or retrospective. Stangl et al13 showed a higher rate of caesarean section (55%) in high-risk patients in a single-centre study of 93 pregnancies. Other studies on pregnancy and heart disease, published by Ouyang (112 pregnancies), Khairy (90 pregnancies), Siu (302 pregnancies), Jastrow (312 pregnancies) and Drenthen (1301 pregnancies but mode of delivery was not reported), focused on risk stratification mainly.2–4 ,14 ,15 Jastrow and Khairy reported a caesarean section rate of around 23%. In the study of Siu et al, the caesarean section rate was higher in women with heart disease compared with healthy women (29% vs 23%).2 These studies did not focus on the association between the mode of delivery and maternal morbidity and mortality.1–4 ,13–15 In the current study, we gathered information on both the planned and performed mode of deliveries, the underlying reason for the decision (obstetric or cardiac) and outcome related to the mode of delivery. However, since caesarean section is chosen as the mode of delivery in selected patients who are severely ill, major bias is present with respect to baseline characteristics of the patients.
Maternal outcome
We found higher rates of postpartum heart failure in patients delivered by caesarean section (both planned and performed, tables 1 and 4). These patients had higher rates of PET, which increases the risk of heart failure,16 and is perhaps the cause of the higher rates of heart failure in this group. Furthermore, more women delivered by caesarean section were preterm and may have been given antenatal steroids to mature the fetal lungs, resulting in fluid retention and the development of pulmonary oedema.17
A greater proportion of women with high-risk factors had a cardiac caesarean section, which may explain the higher maternal mortality rate in patients who had a planned caesarean section, especially considering that no difference was found after matching patients in the analysis of performed caesarean section. Within the cardiac caesarean section group there was a trend towards higher rates of postpartum heart failure in emergency versus elective caesarean section. This may be because the decision for emergency caesarean section was made on the basis of deterioration in cardiac function.
Postpartum haemorrhage was similar across all groups in the analyses. This was a counter to our expectation as caesarean section is associated with an increased risk of postpartum haemorrhage.18 ,19 Furthermore, patients with anticoagulation use were planned for caesarean section more often, especially for cardiac reasons. An explanation may be found in the definition of significant blood loss, which differed between caesarean section (>1000 mL) and vaginal delivery (>500 mL). Additionally haemorrhage is assessed visually, which can be inaccurate.
Elective versus emergency
In the general population, caesarean section is associated with an increased risk of complications, such as venous thromboembolism, infection, peripartum haemorrhage and the risk of general anaesthesia.13 ,17–24 These risks are held to be greater in emergency as compared with the elective caesarean section.25 Indeed, the greater risk with emergency caesarean section is often the stated rationale for choosing an elective caesarean section over attempting a vaginal delivery in women at high-risk of an emergency caesarean section. However, we found that in women with cardiac disease there was no difference in the maternal outcome in any of the groups when we compared emergency versus elective caesarean section. In the analysis of patients in the planned vaginal delivery group but delivered by emergency caesarean section and patients who had a planned and performed elective caesarean section, we did not find differences in the maternal outcome. This is an important finding, since this suggests that planning a caesarean section does not lower the risk of adverse maternal outcome. Therefore, there was no benefit of planned caesarean section over trial vaginal delivery in pregnant patients with cardiac disease. However, our study is not a randomised controlled trial and consequently the data have to be interpreted with caution.
Fetal outcome
Pregnancy duration was shorter and birth weight was lower in planned caesarean section (table 1) and in performed caesarean section (table 3). This implies that vaginal delivery has neonatal benefits in terms of a later delivery and greater birth weight. Alternatively, caesarean section for fetal distress may be performed more often in the context of intrauterine growth retardation, linking low birth weight with caesarean section. Similar results were found in a study by Robertson et al21 including 559 patients, where rate of caesarean section was comparable with controls. In this study, caesarean section was related with adverse neonatal outcome. However, birth weight differed by only 72 g and whether this might have consequences later in life is not clear.
Significant differences in perinatal and neonatal death rates were not found in any of the analyses. But the trend towards higher perinatal mortality in the vaginal delivery group may be partially explained by the inclusion of antepartum stillbirths, for which vaginal delivery is the mode of choice.
When we compared emergency caesarean section versus elective caesarean section in the obstetric group, pregnancy duration was shorter, which explained the trend towards lower birth weight. In this group, the APGAR score was lower in the emergency group, which may indicate that there was fetal distress as a reason for the emergency caesarean section (table 2).
Distribution around the world
We observed marked differences between different countries in this cohort of women with heart disease. Large differences between countries exist in caesarean section rates in healthy women.10 We thought that the variation in the caesarean section rates between countries might explain the differences we observed, but in our initial analysis there was no relationship between the caesarean section rate in the background population of each country and the observed rate in our study. However, when we corrected for the caesarean section rate in the background population, we found a relationship between the caesarean section rate and the proportion of women with more severe heart disease, supporting the idea that the severity of the heart disease in combination with the caesarean section rate in the background population determined the caesarean section rate. A further variation is likely to be introduced by the experience of the attending specialist (either cardiologist or gynaecologist).
Limitations
Given the heterogeneity of the population studied with a multitude of different underlying cardiac diagnoses, collected from 60 different hospitals, conclusions should be drawn with caution. As in every registry, some data (4%) were missing, especially on obstetric complications. In addition, some information was not collected in the case report form of this registry, for instance, the type of anaesthesia used during caesarean section. As participation to the registry was voluntary, there may be differences between sites that agreed to participate and those that did not.
Conclusion
A high proportion of women with cardiac disease deliver by caesarean section, with rates 160% higher than in the general population, as complication rates were similar in elective and emergency caesarean section. Attempting vaginal delivery had neonatal benefits in terms of a later delivery and greater birth weight. Therefore, we suggest that vaginal birth, where it is not contraindicated for an obstetric reason, is a good option for women with heart disease.
Key messages
-
What is already known on this subject?
-
The reported use of caesarean section in patients with heart disease varies from 21% to 55% in different registries and studies. Other studies in pregnant women with heart disease focused primarily on risk stratification. In these studies, caesarean section rates were higher in women with heart disease than in the normal population.
What might this study add?
-
This is the first study to investigate the relationship between mode of delivery and pregnancy outcome in women with heart disease. Maternal outcomes were similar whether delivery was achieved after planned caesarean section or planned vaginal delivery and fetal outcomes were better after a planned vaginal delivery. Therefore, we suggest that where there is no obstetric or cardiac contraindication, a planned vaginal delivery is a better option for women with heart disease.
How might this impact on clinical practice?
-
This study should encourage both obstetricians and cardiologists to consider a planned vaginal delivery in women with heart disease.
Acknowledgments
The authors thank the EORP team for their excellent support: Elin Folkesson Lefrancq, Cecile Laroche, Charles Taylor, Gerard Gracia, Viviane Missiamenou, Marème Konte, Maryna Andarala, Emanuela Fiorucci, Patti-Ann McNeill, Myriam Glémot and Malika Manini. The investigators who participated in the ROPAC on 1 June 2011 are listed in the online supplementary appendix.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Contributors All authors have made significant contributions to the design, execution, analysis and writing of this paper. All the authors have read, revised and approved of the manuscript and share responsibility for published material.
-
Funding The ROPAC is included in the EurObservational Research Programme (EORP) of the European Society of Cardiology. The EurObservational Research Programme (EORP) was sponsored by the following companies: Abbott Vascular, Amgen, Bayer Pharma, Bristol Myers Squibb, Boehringer Ingelheim, Boston Scientific, Daiichi Sankyo, Menarini, Merck & Co. (MSD), Novartis, Pfizer, Servier.
-
Competing interests None.
-
Ethics approval When warranted, ethical approval or Institutional Review Board (IRB approval) was obtained (eg, Germany, USA, Canada, Belgium). However, in many countries the procedure to obtain ethical approval was waived because of the anonymised and untraceable nature of the data.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement Data from each centre will be shared with all investigators in the ROPAC.