Article Text

Abstract
Objective To evaluate the effect of heart rate reduction by ivabradine on coronary collateral function in patients with chronic stable coronary artery disease (CAD).
Methods This was a prospective randomised placebo-controlled monocentre trial in a university hospital setting. 46 patients with chronic stable CAD received placebo (n=23) or ivabradine (n=23) for the duration of 6 months. The main outcome measure was collateral flow index (CFI) as obtained during a 1 min coronary artery balloon occlusion at study inclusion (baseline) and at the 6-month follow-up examination. CFI is the ratio between simultaneously recorded mean coronary occlusive pressure divided by mean aortic pressure both subtracted by mean central venous pressure.
Results During follow-up, heart rate changed by +0.2±7.8 beats/min in the placebo group, and by –8.1±11.6 beats/min in the ivabradine group (p=0.0089). In the placebo group, CFI decreased from 0.140±0.097 at baseline to 0.109±0.067 at follow-up (p=0.12); it increased from 0.107±0.077 at baseline to 0.152±0.090 at follow-up in the ivabradine group (p=0.0461). The difference in CFI between the 6-month follow-up and baseline examination amounted to −0.031±0.090 in the placebo group and to +0.040±0.094 in the ivabradine group (p=0.0113).
Conclusions Heart rate reduction by ivabradine appears to have a positive effect on coronary collateral function in patients with chronic stable CAD.
ClinicalTrials.gov Identifier: NCT01039389.
Statistics from Altmetric.com
Introduction
In patients with coronary artery disease (CAD), the size of myocardial infarction is the main prognostic determinant after such an event. Hence, it is the primary strategy to reduce cardiovascular mortality by reducing infarct size which, in itself, is influenced by the duration of coronary occlusion, ischaemic area at risk for infarction, lack of collateral blood supply to the ischaemic zone, absence of ischaemic preconditioning before the infarct and myocardial oxygen consumption during the infarct.1 Aside from curtailing coronary occlusion time, the option of reducing infarct size by collateral artery growth promotion is appealing.2
It has been demonstrated in rabbits undergoing femoral artery occlusion with connection of the distal arterial stump to the adjacent vein, that tangential fluid shear stress is the major trigger of collateral growth (arteriogenesis).3 Lower-leg external counterpulsation (ECP) triggered to occur during diastole induces a flow velocity signal and, thus, tangential endothelial shear stress in addition to the flow signal related to cardiac stroke volume.4 ECP has been shown to effectively augment coronary collateral function in patients with CAD.4 ,5 Since one of the effects of exercise training is the development of bradycardia at rest, an element of the coronary arteriogenic action of exercise could be the extension of diastole with prolonged action of tangential shear force on the endothelium.6 In this context, a bradycardia-inducing drug without the coronary vasoconstricting action of β-blockers could, theoretically, have a positive effect on collateral function.7 Therefore, the present investigation in patients with chronic, stable CAD tested the hypothesis that ivabradine given for 6 months augments coronary collateral function intraindividually and in comparison with placebo.
Methods
Study design and patients
This was a prospective study in 46 patients with chronic stable CAD who were randomly allocated to placebo (n=23) or ivabradine (n=23) given in a single-blinded fashion for the duration of 6 months. The primary study endpoint was collateral flow index (CFI; calculation given below) as obtained during a 1 min coronary artery balloon occlusion at study inclusion (baseline), and at the 6-month follow-up examination. Secondary study endpoints were the quantitatively determined intracoronary ECG ST segment shift, and angina pectoris during the same 1 min coronary occlusion.
Coronary angiography was performed for diagnostic purposes because of chest pain. Criteria for study inclusion were age >18 years, written informed consent to participate in the study, and 1–3-vessel chronic stable CAD amenable for percutaneous coronary intervention (PCI). Exclusion criteria were acute coronary syndrome, CAD treated best by surgical coronary bypass, an important indication for β-blocker treatment, resting heart rate <50/min without any treatment, sick sinus syndrome, sinu-atrial block or >2nd-degree atrioventricular block, atrial fibrillation, long-QT syndrome, cardiac pacemaker, severe hepatic or renal failure (creatinine clearance <15 mL/min), hypersensitivity against ivabradine or adjuvants.
Cardiac catheterisation and coronary angiography
Patients underwent left heart catheterisation and coronary angiography for diagnostic purposes from the right femoral artery approach. Biplane left ventriculography was performed followed by coronary angiography. Coronary artery stenoses were determined quantitatively as percent diameter reduction using the guiding catheter for calibration. Aortic pressure was obtained via a 6F coronary artery guiding catheter. Central venous pressure (CVP) was measured via the right femoral vein.
Invasive coronary assessment
Primary study endpoint: Coronary occlusive collateral flow relative to normal antegrade flow through the non-occluded coronary artery (CFI) was determined using coronary pressure measurements. A 0.014 inch pressure-monitoring angioplasty guidewire (Pressure Wire, Radi, Uppsala, Sweden) was set at zero, calibrated, advanced through the guiding catheter, and positioned in the distal part of the vessel of interest. CFI was determined by simultaneous measurement of mean aortic pressure (Pao, mm Hg), the distal coronary artery pressure during balloon occlusion (Poccl, mm Hg), and the CVP (mm Hg; figure 1) as obtained during the last 10 s of the 1 min coronary balloon occlusion. CFI was calculated as (Poccl-CVP) divided by (Pao-CVP).8 The accuracy of pressure derived CFI measurements in comparison to ECG signs of myocardial ischaemia during occlusion and to absolute myocardial perfusion measurements has been documented previously.9–11
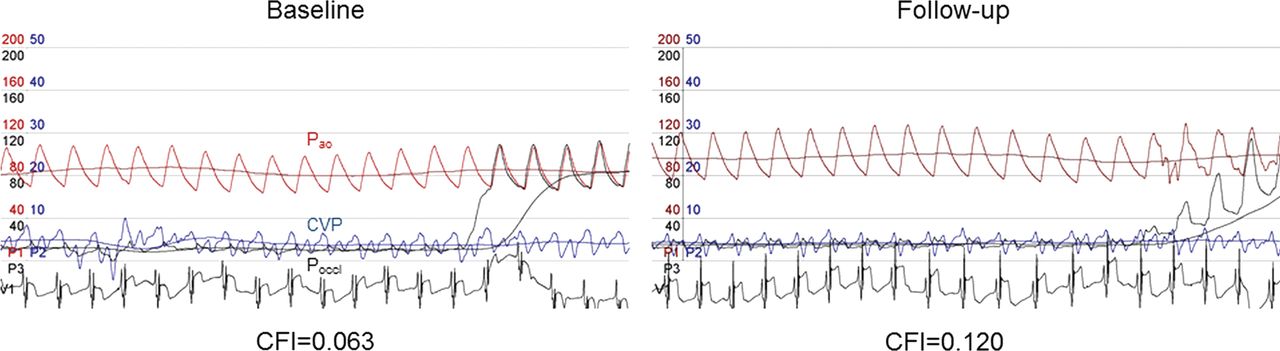
Coronary collateral flow index (CFI) measurement in a patient randomised to receive ivabradine at the baseline (left panel) and at the follow-up examination (right panel). On both panels, simultaneous recordings of phasic and mean aortic pressure (Pao, red line; scale: 200 mm Hg), distal coronary occlusive pressure (Poccl, black line; scale: 200 mm Hg) and central venous pressure (blue line; scale: 50 mm Hg) are shown; additionally, an intracoronary ECG tracing is depicted at the bottom.
Secondary study endpoints: Signs of myocardial ischaemia were assessed simultaneously with CFI measurement as quantitatively determined intracoronary ECG ST segment shift in mV normalised for the absolute R/S amplitude in mV of the same beats (figure 1); the intracoronary ECG lead was obtained from the angioplasty guidewire via a cross-clamp to lead V1.9 ,12 Myocardial ischaemia during the 1 min coronary occlusion was also characterised by the presence or absence of angina pectoris.
Study protocol
Patient study inclusion occurred 5 days prior to the baseline invasive exam, because tapering and stop of the treatment with β-blockers had to take place. At the start of both baseline and follow-up invasive procedures, all patients received 5000 units of heparin intravenously. Following diagnostic exams, two puffs of oral isosorbidedinitrate were given. The coronary artery regarded to be the culprit lesion responsible for the patient's symptoms was selected for CFI measurements. This vessel would undergo PCI following the 6-month study protocol, provided that fractional flow reserve (FFR) at baseline ≥0.75. If FFR was <0.75, the stenotic lesion was treated by PCI at baseline. FFR was obtained prior to CFI. FFR was determined with the pressure guidewire positioned distally in the non-occluded vessel of interest using an intracoronary bolus of 30–40 μg adenosine for hyperaemia induction: FFR=distal coronary pressure divided by Pao. For CFI measurement, an adequately sized angioplasty balloon catheter (20 mm in length, diameter ranging from 2.5–4 mm) was positioned in the proximal or mid part of the vessel while the pressure guidewire remained distally, and balloon inflation occurred at a pressure of 1–2 atmospheres. During this vessel occlusion, simultaneous Poccl, Pao and CVP were obtained for the calculation of CFI. During the entire procedure, the intracoronary ECG obtained from the guidewire was recorded. Immediately after CFI measurement, the patient was asked about the occurrence of angina pectoris during the 1 min coronary artery balloon occlusion.
The initial invasive procedure was followed by the 6-month treatment period initiated by a 1-week placebo run-in phase in all patients. For the determination of resting heart rate at baseline, a 24 h ECG monitoring was performed the day after the invasive procedure. At the start of week 2, the study drug was started as randomly selected. The study drug was begun at a lower dose (5 mg/day for ivabradine, an identically looking tablet for placebo) and increased to a higher dose with the aim to reduce resting heart rate to 60/min (maximum dose for ivabradine of 7.5 mg per day or an identically looking tablet for placebo). Seven telephone interviews at the start of weeks 2, 3, 4 and months 3, 4, 5 and at the end of month 5 were performed, whereby dose adjustments, the history of general condition, episodes of angina pectoris, use of short-acting nitrates and side effects were addressed. After the first month, a clinical visit with examination of the patient took place. Prior to follow-up, another 24 h ECG was performed. The invasive follow-up examination immediately after the treatment period consisted of intracoronary measurements identical to those described above. PCI of the stenotic lesion initially deferred was performed immediately after the follow-up measurements.
Statistical analysis
Intraindividual comparison of CFI and heart rate obtained at follow-up versus baseline examination was performed by a paired Student t test. Between-group comparison of continuous demographic, clinical, angiographic, haemodynamic and CFI data was performed by a 2-sided unpaired Student t test. A χ2 test (2×2 table) was used for comparison of categorical variables among the study groups. Linear regression analysis was used for assessing the relation between heart rate change as the independent variable and CFI change during follow-up.
Results
Patient characteristics and clinical data at baseline
There were no statistically significant differences between the groups in regard to age, gender, occurrence of cardiovascular risk factors and intake of cardiovascular drugs (table 1).
Patient characteristics and clinical data at baseline
Coronary angiographic and haemodynamic data at baseline
The coronary arteries undergoing CFI measurement and the number of vessels with CAD were similarly distributed among the groups (table 2). Percent diameter reduction at the site of stenosis was higher and FFR was lower in the vessel of interest among patients later receiving placebo as compared with ivabradine (table 2). In 16 patients of the placebo group and in 17 of the ivabradine group, PCI was deferred according to baseline FFR until immediately after the follow-up CFI measurement (p=0.58).
Coronary angiographic data at baseline
Resting heart rate as obtained during the baseline 24 h ECG monitoring was similar between the study groups (table 3). There was no difference between the groups in systemic blood pressure, left ventricular EF and left ventricular end diastolic pressure (table 3). Invasively obtained coronary, aortic and CVP constituents for the calculation of CFI, as well as CFI itself, did not differ at baseline among the study groups (table 3). The intracoronary ECG ST segment shift normalised for R/S amplitude (mV/mV) at baseline did not differ between the groups. The prevalence of angina pectoris during the 1 min coronary artery balloon occlusion at baseline was similar between the groups.
Haemodynamic and coronary collateral circulation data at baseline
Treatment-related changes of study endpoints
Primary study endpoint: In the placebo group, CFI decreased from 0.140±0.097 at baseline to 0.109±0.067 at follow-up (p=0.12, figure 2); it increased from 0.111±0.078 at baseline to 0.156±0.089 at follow-up in the ivabradine group (p=0.0461). The difference in CFI between the 6-month follow-up and baseline examination amounted to −0.031±0.090 in the placebo group, and to +0.040±0.091 in the ivabradine group (p=0.0113; figure 3).

Individual values of collateral flow index (CFI; vertical axis) at the baseline and follow-up examination in the placebo group (left) and in the ivabradine group (right).

Individual differences between the follow-up minus the baseline values of collateral flow index (δ CFI, upper panel) and average heart rate as determined during 24-h ECG monitoring (δ heart rate, lower panel) in the placebo and ivabradine group.
During the same period, heart rate changed by +0.2±7.8 beats/min in the placebo group, and by –8.1±11.6 beats/min in the ivabradine group (p=0.0089; figure 3).
Secondary study endpoints: Intracoronary ECG ST segment shift normalised for R/S amplitude changed from 0.241±0.324 at baseline to 0.291±0.303 at follow-up in the placebo group (p=13; figure 4); it decreased from 0.353±0.279 at baseline to 0.181±0.163 at follow-up in the ivabradine group (p=0.0196; figure 4). Heart rate as obtained simultaneously to the 1 min coronary occlusion for CFI measurement changed from 69±12 at baseline to 70±12 at follow-up in the placebo group (p=0.78), and it changed from 69±17 at baseline to 65±12 at follow-up in the ivabradine group (p=0.13; figure 4). In comparison, heart rate as measured during 24 h monitoring changed from 76±10 at baseline to 75±10 at follow-up in the placebo group (p=0.91), and it decreased from 73±9 at baseline to 64±10 at follow-up in the ivabradine group (p=0.0035).

Individual values at the baseline and follow-up examination of intracoronary ECG ST segment shifts normalised for R/S amplitude in mV/mV (upper panel) as obtained during coronary occlusion (simultaneous to collateral flow index measurement; see figure 2), and of the simultaneously determined heart rate (lower panel) in both the placebo and ivabradine group.
The occurrence of angina pectoris during coronary occlusion changed from 15 to 18 out of 23 cases in the placebo group, and it changed from 17 to 18 cases in the ivabradine group (p=0.44 for the intergroup comparison).
There was an inverse relation between the change in heart rate during follow-up and the change in CFI (figure 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Correlation between the individual, follow-up-induced differences in heart rate (δ heart rate, horizontal axis) and in collateral flow index (δ CFI, vertical axis).
Discussion
This first-time clinical, placebo-controlled randomised study found ivabradine to be efficacious on coronary collateral function, and this was accompanied by diminished ECG signs of ischaemia.
Bradycardia and coronary collateral function
The main finding of this study is plausible, and the concept of a coronary arteriogenic effect of bradycardia is supported by data from the literature. Bradycardia has been shown to be associated with augmented angiographic collaterals in humans with CAD,13 and to promote collateral growth in experimental models of coronary occlusion following atrioventricular node ablation.14 ,15 A study in 106 patients without CAD undergoing quantitative CFI measurements has further identified non-β-blocker-induced low heart rate as an independent predictor of augmented collateral function.16 The theory behind the result is that of a prolonged diastolic action of a physical pro-arteriogenic force, tangential fluid shear force, at the endothelial cell layer. Tangential shear force τ (in dyne/cm2) is the product of blood viscosity (0.03 dyne s/cm2) and shear rate (s−1), that is, the spatial rate of velocity change between different fluid layers or between the fluid layer adjacent to the endothelium and the endothelium itself (=4× spatial mean velocity×vessel radius). Since diastolic prolongation during low heart rate in the absence of vasoactive substances is probably not associated with a change in vessel calibre or with altered coronary flow velocity, and blood viscosity is not affected either by bradycardia, the physical trigger for arteriogenesis is acting longer when compared with a shorter diastole. Alternatively, enhanced cyclic vascular stretch during bradycardia may have a pro-arteriogenic effect.17 In dogs, β-blockers have been described to exert a vasoconstrictive effect on the coronary circulation,18 the fact of which has been related to the absence of a bradycardia-induced coronary arteriogenic effect in the presence of β blocker-induced bradycardia.16 In the present study, the potential vasoconstrictive effect was the main reason for interrupting treatment with β blockers aside from their effect on ventricular contractility and on ventricular afterload. Ventricular afterload reduction is related to an augmented coronary flow in the context of an improved early diastolic coronary suction wave.19 Conversely, the If-channel inhibitor, ivabradine, lowers heart rate by inhibiting sinus node activity, leaving myocardial contractility and ventricular afterload unaffected.
Arteriogenic effect of ivabradine: experimental data from the literature
So far, there has been only one experimental study investigating the effect of ivabradine on collateral flow to the supply area of the ligated femoral artery in wild-type and apolipoprotein E knock-out mice.7 Schirmer et al found that adaptive collateral artery growth in the wild-type mice restored microsphere perfusion to 62% of the ligated versus unligated hindlimb. Natural perfusion restoration was hampered in apolipoprotein E knock-out mice. Six weeks of treatment with ivabradine remained without effect in the wild-type mice (55%), but restored perfusion to the level of wild-type mice in apolipoprotein E knock-out mice, that is, to 60% ligated versus unligated hindlimb. The latter relative perfusion parameter is directly comparable with the primary efficacy endpoint of the present study, that is, CFI, which expresses coronary pressure-derived collateral flow relative to normal antegrade coronary flow. However, the magnitude of ivabradine-induced increase in relative collateral flow was approximately 5% points in ours versus 20% points in the experimental study, whereby the absolute level of restorable collateral function following arterial ligation was 4 times higher than the average CFI in our study. Despite the fact that all our patients suffered from dyslipidemia, the apolipoprotein E knock-out mouse model represents a much more coherent and more severe dysfunction of lipid metabolism than that found in the common CAD patient. Conversely, the ‘wild-type’, 60-year-old CAD patient does not correspond in whatever feature to the young wild-type mouse.
Arteriogenic versus anti-ischaemic effect of ivabradine
Initially, ivabradine was designed to prevent myocardial ischaemia by an improvement of coronary blood flow through a prolongation of diastolic duration.20 However, in the BEAUTIFUL trial, heart rate reduction with ivabradine did not improve cardiac outcomes in all patients with stable CAD, but only in those who had heart rates of 70 beats/min or greater.21 In our study, ivabradine had a beneficial effect on collateral function, and this was reflected by the simultaneously and quantitatively obtained intracoronary ECG ST segment shift, which was reduced during the follow-up examination. The mitigated ECG signs of ischaemia during occlusion appeared to be influenced predominantly by the augmented collateral function and not so much by reduced heart rate with lowered oxygen demand, because it showed only a trend to lower values under ivabradine as opposed to the significant negative chronotropic effect during the 24 h ECG monitoring.
Study limitations
The prevalence of angina pectoris during the 1 min coronary occlusion was not lowered in response to ivabradine. This indicates that for this qualitative secondary endpoint, the study was not sufficiently powered to detect changes.
A similar number in each group underwent PCI at baseline due to a haemodynamically relevant stenosis. Thus, in the patients with ad hoc PCI, the effect of the study drug on collateral function was not separable from that of stenosis removal, that is, the most relevant determinant of collateral function.22 The CFI-lowering effect of stenosis removal at baseline may have masked the overall positive effect of ivabradine and, as such, would have had a conservative effect on the null hypothesis of the study (ie, no effect of ivabradine on collateral function).
Key message
What is already known on this subject
-
One study in the experimental animal model showing a pro-arteriogenic effect of ivabradine in the ischaemic hindlimb.
What this study adds
-
Proof of concept of the arteriogenic potential in regard to the human coronary collateral circulation.
References
Footnotes
SG and TT contributed equally.
-
Contributors SG: data acquisition, data analysis, review of manuscript draft. TT: data acquisition, data analysis, review of manuscript draft. MS: data acquisition, review of manuscript draft. DS: data acquisition. HS: data acquisition. AK: data acquisition. RV: data acquisition. CS: concept of the study, data acquisition, data analysis, writing the manuscript.
-
Funding CS has received grant support from the Swiss National Science Foundation for research (grant #3200B_141030/1) and from the Swiss Heart Foundation.
-
Competing interests None.
-
Ethics approval The study was approved by the ethics committee of the Kantonale Ethikkommission of Bern, Switzerland.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.