Article Text

Abstract
There are important dissimilarities in clinical presentation, aggregation of comorbidities, cardiovascular risk factors and the quality of delivery of medical care among men and women with acute coronary syndrome (ACS). Compared with men, despite the well-known older age and more pronounced frailty, women with ACS present later from symptom onset and are at high bleeding risk after invasive procedures. In addition, autoimmune/inflammatory disease, fibromuscular dysplasia, polycystic ovary, early menopause and history of pre-eclampsia are risk factors preceding ACS among younger women. They more often experience myocardial infarction in the absence of obstructive coronary arteries (MINOCA), which makes diagnosis and treatment of ACS among women more challenging compared with men. Women and men do both benefit from guideline-recommended treatment, although, compared with men, women with ACS have a higher adjusted risk of early death, which equalises between both sexes within the first year. Young women with ACS suffer frequently of depression and present often with MINOCA. Compared with young men, they (young women) have a higher risk of death. Therefore, focusing on young patients with ACS, understanding the particular physiopathology of MINOCA and developing programmes targeting comorbidities and depression-related behavioural risk factors are urgently needed.
- acute coronary syndromes
- percutaneous coronary intervention
- acute myocardial infarction
Statistics from Altmetric.com
Patients presenting with suspected acute coronary syndrome (ACS) to the emergency departments are almost half as frequently to be women and the most frequent diagnosis among them is non-ST-segment elevation myocardial infarction (NSTEMI) and unstable angina.1 2 With wide embracement of clinical practice guidelines, diagnosis and treatment of ACS has drastically improved leading to increased survival.3 4 However, sex-related differences in mortality has been continually reported. Women with ACS have 20% higher adjusted mortality risk in short term after successful percutaneous coronary intervention (PCI) compared with men.2 5 6 The opposite happens more than 1 year after PCI, with risk of cardiac death similar and even lower among women.6 It is important to highlight that in female but not male patients with NSTEMI-ACS, the risk of dying of non-cardiovascular reasons overcomes that of cardiovascular death, 6 years after the index event.7
There are important dissimilarities in clinical presentation, aggregation of co-morbidities, cardiovascular risk factors and the quality of delivery of medical care among men and women with ACS (figure 1), which we summarise in this review.
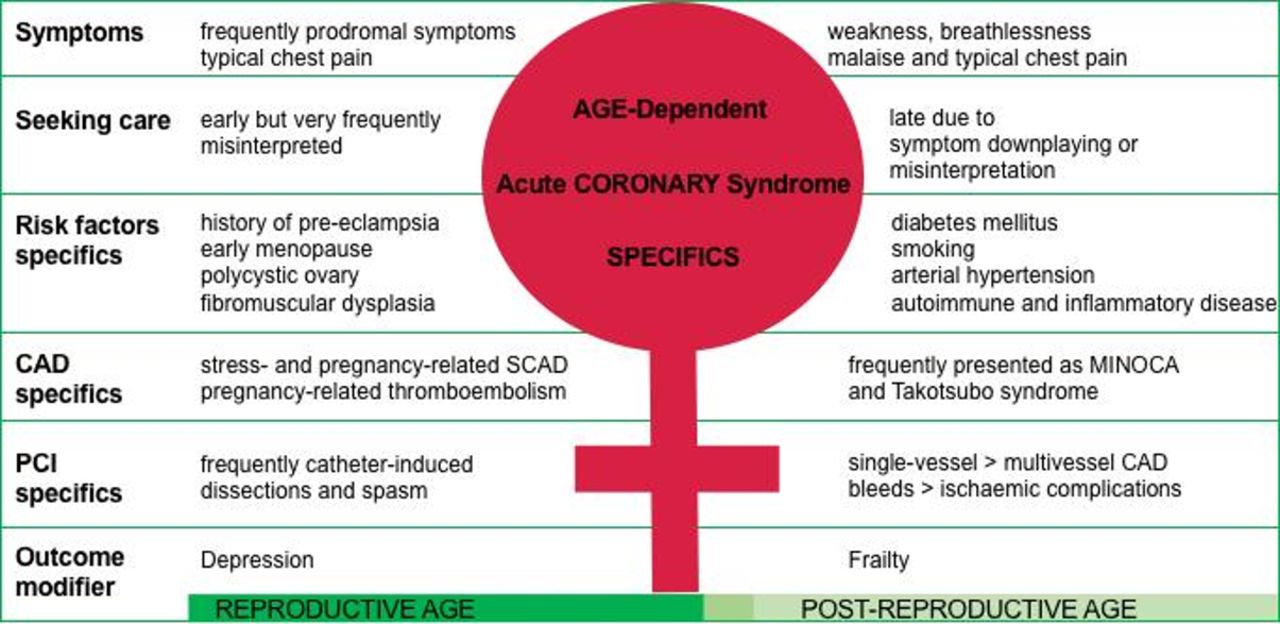
Age-dependent specifics of acute coronary syndrome in women. CAD, coronary artery disease; MINOCA, myocardial infarction in the absence of obstructive coronary arteries; SCAD, spontaneous coronary artery dissection; PCI, percutaneous coronary intervention.
Symptom experience and delay in seeking medical care
Typical chest pain remains the most common symptom among patients with ACS independent of the age of presentation.8 9 However, women, more frequently than men, complain of symptoms other than typical chest pain (weakness, breathlessness, malaise). Among more than 1 million of patients with ACS enrolled in the National Registry of Myocardial Infarction, odds for women versus men to present with atypical symptoms was 1.03, 95% CI 1.02 to 1.04 in patients aged 75–84 years and increased to 1.30, 95% CI 1.23 to 1.36 in patients younger than 45 years.8 On the other hand, compared with young men, young women have higher likelihood to experience prodromal syndromes before ACS presentation and seek medical attention.10 More recently, however, in large series of ACS in pregnancy, typical chest pain was present in 93% of the women at the emergency department and it was often not considered (41% treated only medically).11
Misinterpretation of symptoms because of lack of knowledge, taking time in order to avoid disturbing family members or to finish household work before going to general practitioner often lead to delay in seeking help. Women with ACS present at the emergency unit at least 1 hour later from symptom onset than men do.9 This results to a much longer door-to-balloon time interval among women particularly the one being younger than 65 years of age.5 12 Although triggered by a better symptom recognition and guideline recommendations, the proportion of men and women with ST-segment elevation myocardial infarction (STEMI) treated within the door-to-balloon time window of 90 min has continuously increased over the years (table 1), the sex-related gap particularly among younger patients with STEMI sill persists.5 13
Studies reporting age-specific and sex-specific performance parameters for patients with acute coronary syndrome published after 2010
Age at disease manifestation and risk profile
Age of women suffering from ACS is in mean 67–70 years, thus up to 10 years older than mean age of men.2 More than one-third of them has diabetes mellitus and its consequences including kidney disease.14 15 Moreover, a third of patients with ACS are frail and a quarter of those ≥75 years are severely frail.16 Female sex independently predicts frailty among elderly patients with ACS, and frail women are at high risk of death despite ACS treatment.17
Furthermore, while risk factors are the same for both sexes, the relative weight of them differs. In women, diabetes mellitus, smoking and hypertension impacts more than dyslipidaemia and by more than one risk factor, the CAD risk increases exponentially.18 Women suffer more frequently than men from autoimmune and inflammatory diseases like lupus or rheumatoid arthritis, which has been proven to double the cardiovascular risk. Furthermore, there are female sex-specific risk factors like polycystic ovary, early menopause and history of pre-eclampsia that should be taken into account in evaluating a suspect of ACS.18
Among younger patients with ACS (defined as either <55 years or <65 years of age) undergoing primary PCI, women have a higher risk of death compared with their male peers.14 19 Despite immense improvements done in diagnostic, medical therapy and revascularisation strategies of CAD, reduction of cardiovascular mortality in the course of 20 years, 1979–2011, shows a clear age-dependent and sex-dependent pattern. Among individuals older than 65 years, the reported estimated annual percentage of changing mortality was nearly identical, 3.1% vs 3.3%, while among individuals <55 years of age it was 2.8% in men and 1.9% in women.3 Late presentation, symptom misinterpretation, late diagnosis as well as CAD manifestation as myocardial infarction in the absence of non-obstructive coronary arteries (MINOCA) with or without spontaneous coronary artery dissection (SCAD) might partially explain this mortality.20
In addition, a large body of scientific evidence demonstrates the negative impact of depressive symptoms on outcomes in patients with CAD and the presence of a sex/age interaction on adverse cardiovascular effects of depression.21 In a registry of 3237 patients enrolled before having coronary angiography across three Emory healthcare sites, young women with CAD (≤55 years) demonstrated the higher prevalence of moderate or higher severity depressive symptoms (27%) while men ≥65 years of age had the lowest prevalence (9%).21 There was a significant depression/sex/age interaction related to death. Young women and men aged ≥65 years with moderate/severe depression had increased risk of death compared with those with no/mild depression, HR 1.08, 95% CI 1.01 to 1.15 and HR 1.07, 95% CI 1.03 to 1.09, respectively.21
Coronary artery disease: obstructive atherosclerosis
Compared with men, women have less pronounced coronary atherosclerosis. Prevalence of subclinical coronary atherosclerosis among middle-aged individuals is lower among women compared with men, 10% vs 43%, p<0.001 for 50–54 years of age.22 Clinical coronary artery disease is less diffuse and complex among women, highlighted also by a lower proportion of women with ACS having a history of coronary artery bypass surgery or need for it.23 24 Among aged-matched women and men presenting with STEMI, no differences in culprit plaque morphology, composition of aspirated thrombus and immune and inflammatory serum biomarkers have been reported.25 Furthermore, despite having smaller coronary arteries and being more prone to dissection during PCI, the risk of repeat revascularisation and stent thrombosis is very low and shows no sex-related differences even at long-term follow-up.23
Coronary artery disease: non-obstructive atherosclerosis
Non-obstructive atherosclerosis is one of the pathophysiological causes of MINOCA. Among patients with ACS, MINOCA is observed at younger ages, between 59 and 66 years, compared with obstructive CAD ACS and is more common in women, 10.5% vs 3.4% in men (figure 2 and table 2).14 20 26 This entity is challenging to diagnose and puzzling to treat. The 4-year follow-up of 9136 MINOCA patients surviving the first 30 days in the Swedish Web-system for Enhancement and Development of Evidence-based care in Heart disease Evaluated According to Recommended Therapy registry demonstrated a significant reduction of major adverse cardiac events related to use of statins (HR 0.77, 95% CI 0.68 to 0.87) and ACE inhibitors/angiotensin receptor blockers (HR 0.82, 95% CI 0.73 to 0.93) as well as a statistical trend towards better outcomes with use of beta-blockers (HR 0.86, 95% CI 0.74 to 1.01). On the contrary, despite what we believe, 1-year use of dual antiplatelet therapy did not added any significant benefit (HR 0.90, 95% CI 0.74 to 1.08).26 Another challenge is progressively increasing mortality risk associated with the number of accompanying risk factors. In women suffering from myocardial ischaemia without obstructive CAD, 5-year cardiovascular mortality ranges between 10% with ≤1 risk factor and 25% with >3 risk factors.27

{kind=link}
{kind=link}
Sex-specific features of clinical and angiographic pattern of acute coronary syndrome. (N)STEMI, (non)ST-segment elevation myocardial infarction; SCAD, spontaneous coronary artery dissection.
Key differential features among obstructive and non-obstructive coronary artery diseases leading to clinical presentation of ACS
Coronary artery disease: spontaneous coronary artery dissection
SCAD is a rare cause of ACS, but 90% of the cases are reported in women (table 2).28 In large registries, SCAD is reported as the cause of acute myocardial infarction (AMI) in 1% of cases.29 This is most probably underestimated due to the diagnosis done by standard coronary angiography which cannot detect the dissection if it is only present as intramural haematoma occluding the lumen in the absence of dye fixation typical of intimal tear. When SCAD is not clearly identified in coronary angiogram, intravascular ultrasound or optical coherence tomography which enable more precise imaging of the arterial wall need to be more extensively used in women with ACS in order to improve the pathophysiological diagnosis.20 On the other hand, among women younger than 50 years of age the prevalence of SCAD has been reported in 10%–20% of AMI.30 Furthermore, SCAD accounts for 43% of all pregnancy-related myocardial ischaemia, in this case both oestrogen and progesterone can play a role in weakening the vessel wall.31 Emotional and physical stress has been identified as SCAD triggers in 40% and 25% of cases, respectively.32 Catecholamine surge may also here play a pathogenic role increasing cardiocirculatory shear stress and blood pressure. SCAD is often associated with fibromuscular dysplasia, a condition that leads to a disruption of smooth muscle cells, fibroblasts and surrounding connective tissue of the vessel wall in great and middle arteries particularly renal artery. This condition is much more prevalent in women around 50 years of age testifying a probable role of hormones in this disease.32
The left anterior descending artery and its branches are most commonly involved by SCAD (45%–61%) and multiple coronary artery dissections can occur (<10%). Evidence-based therapies are not well established, but a conservative approach for non-flow-limiting SCAD accompanied by beta-blocker and stringent blood pressure control lead to better long-term survival of these patients.29
The reasons of better outcomes with conservative approach are fast resorption of intramural haematoma and spontaneous dissection healing (within 1 month) as well as the limited success of percutaneous coronary intervention due to wire or catheter-induced dissection propagation. Interventional procedures supported by intracoronary imaging, however, have to be considered when coronary flow is impaired and recurrent ischaemia or haemodynamic instability is present.
In-hospital mortality is around 5%, while recurrences, usually presenting in a new vessel or location different from the originally dissected vessel, occur in 15% at 2 years and up to 25% at 5 years.33 Patients with pregnancy-related SCAD have a worst prognosis because of more proximal area of dissection and late presentation ending in larger infract areas.11
Coronary artery disease: macrovascular and microvascular dysfunction
Rest angina due to epicardial coronary arteries vasospasm (variant or Prinzmetal angina) responding to short-acting nitrate is more common in men at least in German and Japanese population,34 while the one due to coronary microvascular impairment is typical of women.35
Coronary microvascular dysfunction (CMVD) is present in presence of ischaemic ECG changes and angina without obstructive coronary artery disease. The causes of CMVD can be structural (atherosclerotic microembolisation); extravascular (hypertrophy-induced perivascular fibrosis or compression) or functional (enhanced microvascular constriction or attenuated dilatation due to impaired endothelium release of vasoactive substances like nitric oxide which are stimulated by oestrogens).36
Takotsubo syndrome
It is well known that Takotsubo syndrome (TTS) is characterised by acute left ventricular dysfunction clinically presenting as ACS triggered by emotional or physical stress.37 It is considered an ACS because of clinical and ECG presentation even if the increase in cardiac troponin level is usually mild while a Brain natriuretic peptide can be sharply increased.
A recent study found alterations in subnetworks of resting state functional connectivity.38 Structures such as limbic system amygdala, hippocampus, cingulated gyros in these subnetworks which control motivation and memory are involved in emotional process, which emphasises the causative role of the central nervous system in TTS.
In TTS, 80% of patients are postmenopausal women having an emotional trigger. It is known that sympathetic nervous activity is increasing with age and more so in women causing greater cardiac stimulation.39 There is still debate if a direct catecholamine-induced myocardial toxicity is the way that adrenoreceptor activation mediates myocardial dysfunction or if microvascular spasm causes myocardial stunning.
It is interesting to note that out of the women with TTS caused by some form of shock, only 5% have pleasant preceding events while 95% of patients present following a negative emotional stress such as death of relatives, fear, anger (broken-heart syndrome!).40 Because positive emotions modulate the autonomic nervous system response to a similar degree as do negative emotion, this could simply mean that postmenopausal women are much more exposed to negative than positive events. Long-term outcome in patients with TTS is similar to age-matched and sex-matched patients with ACS of other aetiology, however, a left ventricular ejection fraction <35% at acute phase is associated with poor acute and long-term outcomes.41
ACS in pregnancy
AMI during pregnancy is a rare event occurring in 1 in 20 000–30 000 deliveries mainly during the third trimester or in the peripartum or puerperal period.42 Coronary atherosclerotic lesions are present in 20%–43% of the patients with risk factors similar to the one in the general CAD population and the age of the mother is more advanced than in the other aetiology.42 SCAD is present in up to 43% of the cases mostly in young, otherwise healthy women and occur in late pregnancy or within 3 months post partum.31 The arterial wall changes under hormonal influence associated with haemodynamic changes are the bases of pathogenesis of aortic as well as coronary dissection. Often clinical presentation is severe with haemodynamic instability and more frequent adverse events. Thrombus/emboli in the coronary bed which is an extremely rare cause of AMI in the general population can be an important cause of ACS during pregnancy up to 30% in recent series.43 This is the result of profound alterations in the coagulation and fibrinolytic system. Thrombus can be formed in situ or be the result of emboli coming from different sources such as left atrial appendage, mitral valve stenosis, left ventricle in peripartum cardiomyopathy or more often by venous thrombus passing across a patent foramen ovale (pregnancy is associated with fourfold increase in venous thrombosis!).
The problem is that often these patients arrive late due to mistaken interpretation of symptoms and signs of ACS for normal manifestation of pregnancy. The consequences are large myocardial ischaemia with rapidly irreversible myocardial damage due to lack of preconditioning. Thus, avoidance of treatment delay is the most important objective in young pregnant women with ACS.
Delivery of medical care
Women receive less frequently guideline-directed medical therapy and undergo less often evidence-based and guideline-recommended diagnostic and revascularisation pathways compared with men.9 12 24 44 45 The risk of being withheld primary PCI seems to be higher among women particularly the younger ones compared with men younger than 65 years.12 This partially explains the higher mortality risk at short-term after primary PCI for women with STEMI compared with men.5 8 15 19 Despite adjustment for sex-related baseline differences, this risk remains high particularly among among younger women with ACS (table 3).
Studies reporting age-specific and sex-specific mortality for patients with acute coronary syndrome published after 2010
Women are more prone to spontaneous and procedure-related bleeds compared with men.2 23 46 Intersex dissimilarities in the physiology of haemostasis as well as drug overdose and frailty, both more frequently observed in women, have been suggested possible predisposing factors.16 46 However, women and men do both benefit from different bleeding-avoidance strategies such as de-escalation of peri-interventional and maintenance antithrombotic therapy regimens and the preferred use of radial artery access.23 46 47 Therefore at long-term, after adjustment for age and comorbidities, no sex-related differences in mortality and other adverse cardiovascular outcomes have been reported.48
Conclusion
Compared with men, women with ACS have additional female sex-specific risk factors, present much more frequently with non-atherosclerotic involvement of coronary arteries and undergo less frequently use of evidence-based and guideline-recommended diagnostic and revascularisation pathways. Although both women and men with ACS benefit from PCI, the younger women remain at higher risk of death despite use of evidence-based ACS treatment. Better understanding of the disease and its associating comorbidities, use of novel diagnostic and therapeutic tools as well as addressing comorbidities and depression-related behavioural risk factors are urgently needed to improve the outcomes of women with ACS.
References
Footnotes
Contributors Both authors contributed significantly to the conception, initial drafting and significant revision of the manuscript. JM is responsible for the overall content of it. JM wrote the first draft of the paper, PP revised it critically for important intellectual content.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests JM: institutional grant funding from Boston Scientific, lecture fees from AstraZeneca, Bristol-Myers Squib, Edwards Lifesciences, Medtronic, Boston Scientific, Siemens.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; internally peer reviewed.