Article Text

Abstract
Objectives To evaluate emergency medical services (EMS) delays and their impact on time to treatment and mortality in patients with ST-elevation myocardial infarction (STEMI).
Method We collected data on EMS time intervals from published studies across five electronic databases. The primary EMS interval was the time in minutes between first medical contact and arrival at hospital door (FMC-to-door time). Secondary intervals were other components of EMS delay. Weighted means were measured using random-effects models. Meta-regression was used to identify factors associated with EMS delays and to assess the impact of EMS delay on the proportion of patients treated within90 min and mortality.
Results Two independent reviewers included 100 studies (125 343 patients) conducted in 20 countries. The weighted mean FMC-to-door time was 41 min (n=101 646; 95% CI 39 to 43, range 21–88). However, substantial heterogeneity was observed with each interval, which could be explained by region and urban classification, distance to hospital and method of ECG interpretation. In a meta-regression adjusted for door-to-balloon time, a 10 min increase in FMC-to-door time was associated with a 10.6% (95% CI 7.6% to 13.5%; p<0.001) reduction in the proportion of patients treated within 90 min. Shorter EMS delay was significantly associated with lower short-term mortality in patients receiving prehospital thrombolysis (p=0.018).
Conclusion EMS delays account for half of the total system delay in STEMI. There is a fourfold global variation in EMS delays, which are not completely explained by differences in system characteristics. Reducing unexplained variation could yield improvements in the time to treatment and outcome of STEMI patients.
PROSPERO registration number CRD42017074118.
- acute myocardial infarction
- healthcare delivery
- meta-analysis
- ECG/electrocardiogram
- global health
Statistics from Altmetric.com
Introduction
In ST-elevation myocardial infarction (STEMI), timely reperfusion of the occluded coronary artery is associated with a lower risk of mortality and adverse cardiovascular outcomes.1 2 Modern STEMI regional systems-of-care emphasise the importance of streamlining treatment pathways, including emergency medical services (EMS) and in-hospital care. In STEMI patients presenting to EMS, guidelines call for optimal reperfusion by primary percutaneous coronary intervention (PCI) within 90 min of STEMI diagnosis.3
While significant efforts have been made to reduce hospital-related system delays (ie, door-to-balloon time), comparatively little attention has been given to evaluate and improve EMS-related system delay in patients with STEMI. EMS has been widely acknowledged as a crucial component of the STEMI regional system-of-care for its contribution to early diagnosis, a reduction in the time to reperfusion and a reduction in mortality.4–6 However, previous studies show that 30%–50% of patients transported by EMS fail to meet optimal treatment targets (ie, first medical contact-to-balloon time), despite strategies to reduce door-to-balloon times.7 8 A reason for this may be related to performance variation between EMS systems. In addition, a number of potential factors such as variation in population characteristics, accessibility to healthcare, EMS system design and local guidelines could also contribute to variation in EMS delays.9 10 Importantly, there is currently a lack of synthesised data to help establish quality indicators and performance benchmarks for EMS delays in STEMI patients.
In this study, we systematically reviewed the literature to obtain global estimates of EMS delays in STEMI patients, assess EMS delay with respect to a number of system characteristics and describe the impact of EMS delay on time to treatment and short-term mortality.
Method
Search strategy and selection criteria
This review follows the reporting guidelines of the Preferred Reporting Items for systematic Reviews and Meta-Analyses.11 Our search strategy was implemented in five electronic databases including MEDLINE, Embase, Emcare, Cochrane Library and CINAHL, and was limited to English language peer-reviewed reports published between 1990 (the year when the feasibility of prehospital 12-lead ECG was first published in phase I of the FAST-MI study)12 and 10 August 2018. The search strategy was designed in consultation with a medical information librarian, and used a combination of medical subject headings and text terms relating to EMS, acute coronary syndrome and electrocardiography (online supplementary appendix table 1).
Supplementary file 1
Two reviewers (AA and ZN) independently identified clinical trials and observational studies reporting EMS time intervals for adult STEMI patients, who were identified in the prehospital setting using a 12-lead ECG and directly transported to the treating hospital (for thrombolysis or PCI) or received prehospital thrombolysis (PHT). Studies reporting data on secondary or inter-facility transfers were excluded. Disagreements between reviewers at any stage of study selection were resolved through consensus.
Data extraction and outcomes
For studies meeting the eligibility criteria, a standardised data extraction form was used to extract detailed information about study design and setting, EMS and STEMI system-of-care characteristics, patients demographic and selected EMS time intervals. When reported, we extracted in-hospital and total system delay, proportion of patients treated by PCI within 90 min from first medical contact (FMC) and short-term (prehospital, in-hospital and 30-day) all-cause mortality rate for all treatment strategies. If information was missing from the publication, we contacted the authors twice over a 2-month period for clarification.
Figure 1 illustrates the components of total ischaemic time focusing on EMS delay. The primary outcome or EMS interval was the time in minutes between FMC and arrival at hospital door (FMC-to-door time). This time interval was the most frequently reported interval and was considered to assess the impact of EMS delay on time to treatment and mortality. FMC was defined as the time that the ambulance arrived on scene or at patient’s side. The secondary time intervals were the time in minutes between (1) ECG acquisition and arrival at hospital door (ECG-to-door time), (2) the emergency call and arrival at hospital door (call-to-door time), (3) the emergency call and scene arrival (response time), (4) scene arrival to ECG acquisition (FMC-to-ECG time), (5) scene arrival to scene departure (scene time) and (6) scene departure to hospital arrival (transport time). For studies using PHT, we collected information on two additional intervals including the time in minutes between (1) FMC and the administration of PHT (FMC-to-PHT time) and (2) the emergency call and the administration of PHT (call-to-PHT time). Publication bias was assessed using a funnel plot and Egger’s test.13
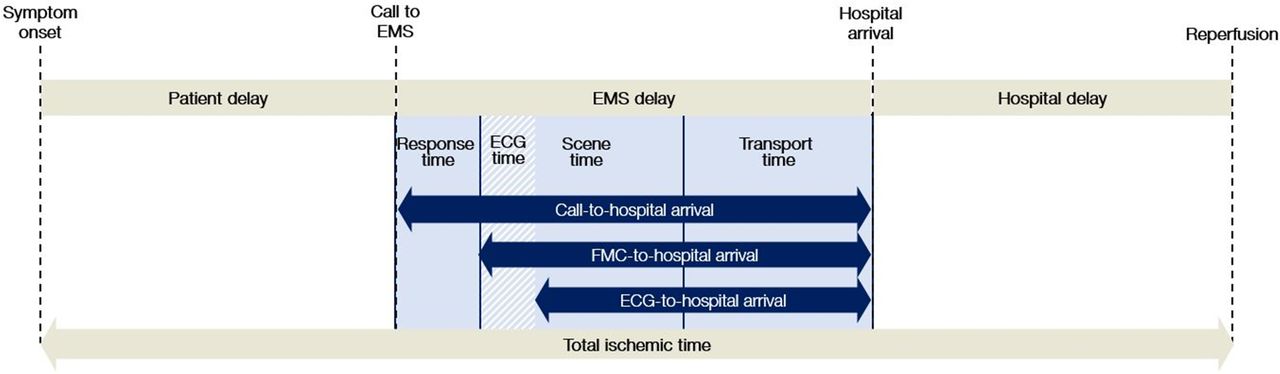
Depiction of total ischaemic time and EMS delay components. EMS, emergency medical services; FMC, first medical contact.
Data synthesis
All data were analysed using Stata V.15 (StataCorp.). A two-sided p value <0.05 was considered statistically significant for all analyses. EMS delay intervals were recorded in minutes and analysed as means and SD. When the study reported other measures of central tendency (52% of the included studies), means and SD were either obtained from authors or estimated from medians and IQR using Wan’s estimation method.14
To reduce heterogeneity in the reported EMS delay intervals, we stratified analyses by the type of reperfusion strategy, including in-hospital reperfusion (PCI or thrombolysis) and PHT. Weighted mean estimates with 95% CI were calculated for each time interval using DerSimonian and Laird random-effects models.15 Heterogeneity across studies was evaluated by calculating the I2 statistic. We performed stratification analyses using meta-regression to explore possible sources of heterogeneity and to identify system characteristics associated with EMS delay.16 We considered several factors, including year of publication, geographical location, urban classification, average distance to hospital, skill level of ambulance clinicians, method of ECG interpretation and other STEMI system strategies.
We also used random-effects models to pool the estimates of population characteristics, proportions and mortality. To evaluate the impact of EMS delay on the proportion of patients achieving a time to treatment (ie, FMC-to-balloon time) <90 min, we performed meta-regression adjusting for in-hospital delays (ie, door-to-balloon time). We also used this method to assess the impact of EMS delay on short-term all-cause mortality for patients treated with PCI and PHT, but not for patients treated with in-hospital thrombolysis (IHT) given the small number of studies.
Results
Study selection and characteristics
The search strategy retrieved 6949 studies, of which 452 underwent full-text screening based on the title and abstract search (figure 2). A total of 100 studies reporting 9 EMS time intervals were included. The agreement between two reviewers was fair (kappa=0.50) for the title and abstract screening, and excellent (kappa=0.89) for the full-text screening.

PRISMA flow diagram. EMS, emergency medical services, IHT, in-hospital thrombolysis; PCI, percutaneous coronary intervention; PHT, prehospital thrombolysis; PRISMA, Preferred Reporting Items for systematic Reviews and Meta-Analyses; STEMI, ST-elevation myocardial infarction.
Summary study characteristics are presented in table 1, and greater detail is presented in online supplementary appendix table 2. Fifteen studies were randomised controlled trials and 85 were observational. Forty studies were conducted in North America, 53 in Europe and seven in the Asia-Pacific region. Twenty studies were conducted in rural areas. Ambulances were most frequently staffed by advanced life support paramedics (67 studies).
Summary of study and patient characteristics by reperfusion strategy
The overall number of participants was 125 243 patients, of which 99.0% had a hospital-confirmed diagnosis of STEMI. Of these, 67 412 patients (59 studies) received PCI treatment, 34 862 patients (18 studies) received in-hospital thrombolysis and 8347 patients (36 studies) received PHT. Demographic data were missing in approximately one-third of the included studies representing >50% of the total population. Of those reported, the weighted mean age was 61.3 years and the weighted proportion of male sex was 73.8%.
Primary outcome in STEMI patients receiving in-hospital reperfusion
Fifty studies reported on FMC-to-door time for 101 646 patients. FMC-to-door time ranged between 21 and 88 min. The weighted mean FMC-to-door time was 41 min (95% CI 39 to 43; I2=100%). The results of the subgroup analysis are presented in figure 3. The factors significantly associated with FMC-to-door time were urban classification, continent, method of ECG interpretation and ED bypass. Figure 4 represents the variation in FMC-to-door time and other component of EMS delay between countries. It was shortest in the USA (32 min; 95% CI 31 to 33) and longest in Australia (48 min; 95% CI 42 to 54). There was substantial heterogeneity in FMC-to-door time, which is persistent across subgroups (I2 >95%). We found that for every 10 km increase in average distance to hospital, FMC-to-door time increases by 6 min (n=15 studies; 95% CI 3.5 to 8.5; p<0.001).

Stratified analysis of FMC-to-door time by study characteristics. Dashed line represents the weighted mean FMC-to-door time in the overall population. CCL, cardiac catheterisation laboratory; ED, emergency department; EMTs , emergency medical technicians; FMC, first medical contact; WM, weighted mean.
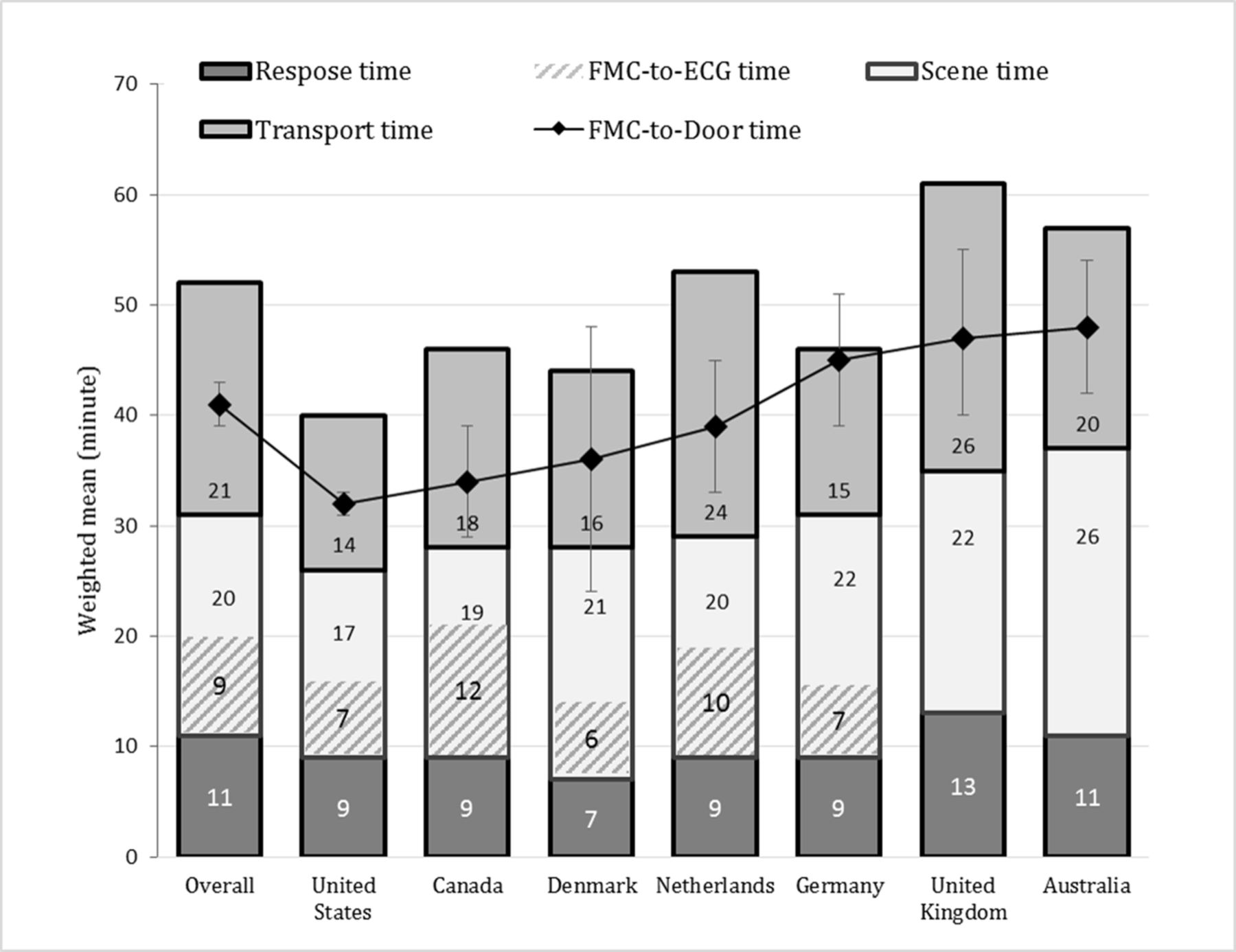
FMC-to-door time and other EMS components among countries. EMS, emergency medical services; FMC, first medical contact.
Thirty-five studies (n=45 125) reported on door-to-balloon time with a weighted mean of 57 min (95% CI 54 to 60). There was a significant relationship between FMC-to-door time and door-to-balloon, indicating a 0.5 min (95% CI 0.15 to 0.86; p=0.007) reduction in door-to-balloon time for every minute increase in FMC-to-door time.
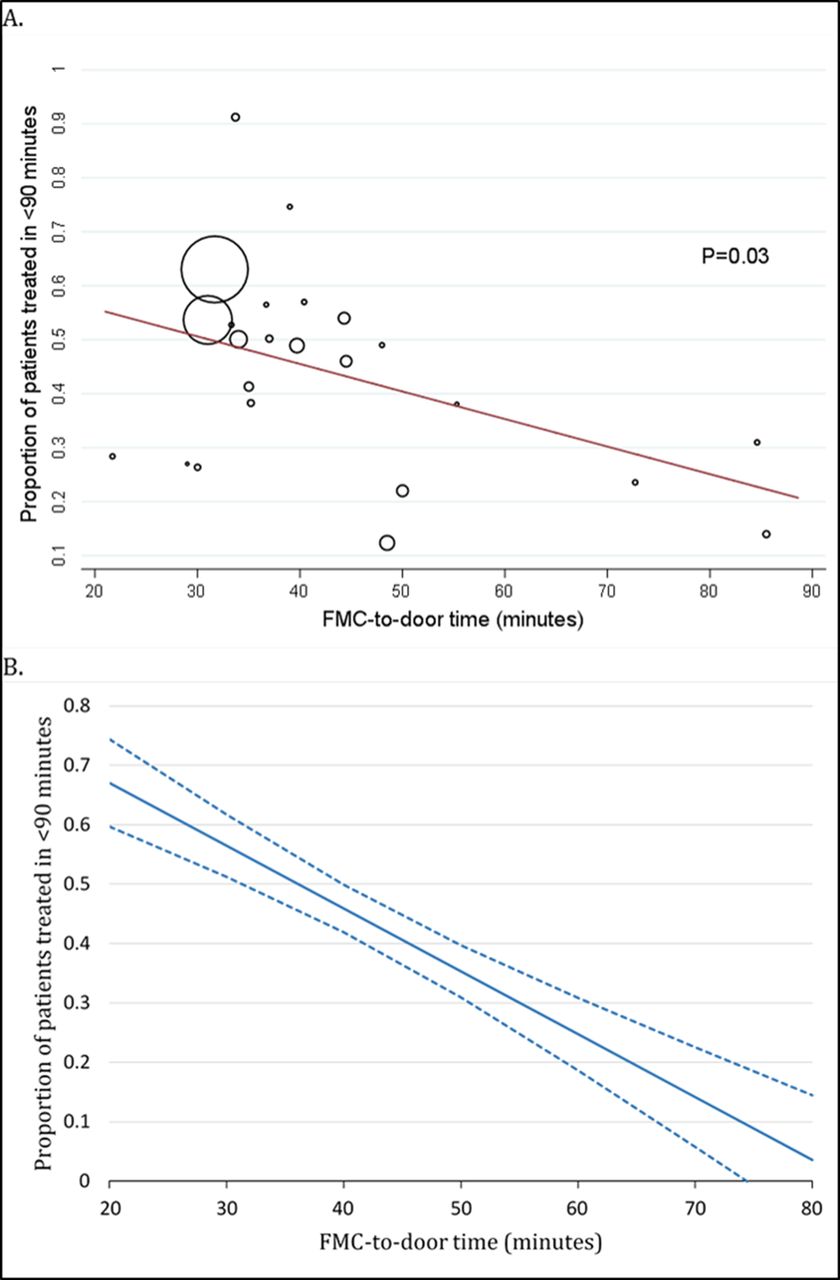
Thirty-seven studies reported on FMC-to-balloon time for 53 432 patients, and the weighted mean was 97 min (95% CI 94 to 100). The pooled proportion of patients with an FMC-to-balloon time within 90 min was 43.9% (22 studies; n=40 554; 95% CI 40 to 50, range 12%−91%). Figure 5 illustrates the impact of FMC-to-door time on the proportion of patients achieving an FMC-to-balloon time within 90 min. Every 10 min increase in FMC-to-door time was associated with a 5.1% (95% CI 0.6% to 9.5%, p=0.03) reduction in the mean proportion of patients treated within 90 min. After adjusting for door-to-balloon time, a 10- min increase in FMC-to-door time was associated with a 10.6% (95% CI 7.6% to 13.5%; p<0.001) reduction in the proportion of patients treated within 90 min.

Meta-regression of the proportion of patients with an FMC-to-door <90 min. (A) Unadjusted meta-regression fitted line against FMC-to-door time. Circles represent proportion of each study and the size of circle varies by the weight of the study in the meta-regression analysis. (B) Predicted probability of the proportion of patients with an FMC-to-door time <90 min after adjusting for door-to-balloon time. FMC, first medical contact.
Mortality rate was reported in 41 studies for 58 740 patients treated by PCI. The pooled mortality rate was 4.1% (95% CI 3.6 to 4.6, I2=80%). The unadjusted meta-regression showed that mortality rate was not significantly associated with FMC-to-door time (figure 6A); a 10 min increase in FMC-to-door time was associated with a 0.8% (−0.4% to 2.0%; p=0.21) increase in mortality rate. Results remained similar when adjusting for door-to-balloon time.

Unadjusted meta-regression of short-term mortality fitted line against EMS delay. (A) FMC-to-door time. (B) FMC-to-PHT time; circles represent the short-term mortality of each study and the size of the circles varies by the weight of the study in the meta-regression analysis. EMS, emergency medical services; FMC, first medical contact; PHT, prehospital thrombolysis.
Secondary outcomes in STEMI patients receiving in-hospital reperfusion
Thirteen studies reported on ECG-to-door time for 6954 patients (online supplementary appendix figure 1). The overall weighted mean for ECG-to-door time was 30 min (95% CI 24 to 36; I2=100%; range 18–54). Thirty studies reported on call-to-hospital arrival time for 62 930 patients (online supplementary appendix figure 2). The overall weighted mean call-to-door time was 55 min (95% CI 52 to 58, I2=99%; range 34–124). In the subgroup analysis, both ECG-to-door time and call-to-door time were significantly associated with continent and urban classification.
Pooled estimates for response time, ECG time, scene time and transport time are shown in online supplementary appendix table 3. Forty-six studies reported on response time for 18 729 patients and the weighted mean was 11 min (95% CI 10 to 12, I2=100%; range 5–35). Eighteen studies reported on ECG time for 7234 patients and the weighted mean was 9 min (95% CI 8 to 10; I2=99%; range 6–16). Thirty studies reported on scene time in 5319 patients. The weighted mean scene time was 20 min (95% CI 19 to 22; I2=97%; range 14–31). Twenty-seven studies reported on transport time for 7613 patients. The weighted mean transport time was 21 min (95% CI 18 to 25; I2=100%; range 9–57). Response time and transport time were associated with urban classification while scene time and transport time were associated with region.
EMS delays in STEMI patients receiving PHT
Twenty-four studies reported on FMC-to-PHT time for 4955 patients. The overall weighted mean for FMC-to-PHT time was 29 min (95% CI 26 to 31; I2=99%; range 18–47). FMC-to-PHT time was significantly associated with continent and method of ECG interpretation (figure 7). Twelve studies reported on call-to-PHT time for 1425 patients (online supplementary appendix figure 3). The overall weighted mean for call-to-PHT time was 47 min (95% CI 41 to 53; I2=98%; range 28–73), and was significantly shorter in urban areas.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Stratification analysis of FMC-to-PHT time. Dashed line represents the weighted mean FMC-to-PHT time in the overall population. EMTs, emergency medical technicians; FMC, first medical contact; PHT, prehospital thrombolysis; WM, weighted mean.
Mortality rate was reported in 16 studies for 4329 patients treated by PHT. The pooled mortality rate was 5.1% (95% CI 4.2 to 5.9, I2=49%). The unadjusted meta-regression showed that mortality rate was significantly associated with FMC-to-PHT time (figure 6B), indicating a 10 min increase in FMC-to-PHT time was associated with a 1.9% (95% CI 0.4% to 3.5%; p=0.018) increase in mortality rate.
Publication bias
Publication bias were not detected in the primary outcome neither by funnel plot nor by Egger’s test. However, it was detected in transport time, FMC-to-ECG time and call-to-PHT time.
Discussion
The present meta-analysis of 100 studies involving more than 125 000 STEMI patients provides an important insight into EMS delays in contemporary STEMI regional systems-of-care. We pooled EMS delays and observed striking variations in all EMS intervals, which were partly explained by a number of system factors. A second point of interest in the present study was to verify whether time-to-treatment and patient outcome were influenced by EMS delay. When adjusted for hospital delay, our meta-regression shows that longer FMC-to-door time is associated with a lower proportion of patients receiving PCI reperfusion treatment within 90 min of FMC. The impact of EMS delay on mortality reached statistical significance only for patients receiving PHT.
For STEMI patients presenting directly to a PCI centre by EMS, the ideal system delay for PCI treatment is ≤90 min from FMC.2 However, our findings suggest that relatively few emergency systems would meet this benchmark performance. The weighted mean door-to-balloon time across 35 studies in our review was almost 60 min, inferring that EMS systems should target delays ≤30 min between FMC and hospital arrival. However, only 20% of the studies included in this review reported EMS delays ≤30 min. Indeed, only 10% of studies reported scene delays ≤15 min, which has previously been recommended to meet benchmark performance.17 18 Although measures such as response time and transport time are often impacted by factors outside of the control of EMS personnel (eg, travel distance and hospital bypass), it is difficult to explain why scene times varied more than twofold across studies included in this review. Our findings therefore suggest that EMS systems could play an important role in reducing unnecessary system delays through close performance monitoring and improvements in clinical and operational processes.
Travel time is a major reason behind the variation in EMS delay among systems. There was a sixfold variation in transport time, which was associated with the average driving distance to hospital. An explanation for the observed variations between and within countries could be the geographic accessibility to a PCI centre. For example, in the USA, where the shortest EMS delays have been observed, it was estimated that about 80% of the population lived within 60 min of a PCI facility in 2000,19 whereas similar estimates were found to be lower in Russia (50%, in 2015),20 Canada (64%, in 2006)21 and Australia (68%, in 2006).22 Introducing new PCI centres in underserved regions may help to improve accessibility and reduce transport time.23
Scene time made up the largest proportion of total EMS delays, particularly in urban systems. However, scene time also had least amount of variation compared with other EMS time intervals (twofold variation), and it was associated with region. This variation is likely related to the disparity in prehospital clinical practice and compliance with protocols.24 25 We found that longer scene time (≥20 min) was associated with systems that involve physician or intensive care mobile unit who have more extensive prehospital treatment guidelines that consume additional time to accomplish; such systems are located in Germany, France, Denmark and Australia. However, higher skilled practitioners were associated with high compliance with STEMI guidelines.26 27 In contrast, other systems are in favour of using ‘scoop and run’ strategy soon after STEMI recognition.
Time to PHT also varied widely among studies. FMC-to-PHT time was associated with continent and method of 12-lead ECG interpretation. Europe had quicker PHT performance than other regions, which could be associated with the rare utilisation of the transmission method because a physician was frequently available on scene. According to current guidelines, PHT should be provided within 20 min of FMC (10 min to diagnosis plus 10 min to needle).3 Only 20% (four studies) achieved average FMC-to-PHT time within <20 min of FMC. The importance of minimising this delay has been clearly shown by its association with lower mortality rate.
Our analysis showed a strong association between EMS delay and the proportion of patients treated by PCI within 90 min of FMC. In addition, our meta-regression analysis, adjusted for door-to-balloon time, showed that a target of >50% of STEMI patients treated within 90 min of FMC could be achieved only when EMS delay is <40 min. Two previous single-centre observational studies have shown similar results that shorter scene time and transport time to hospital or to cardiac catheterisation laboratory were associated with higher probability to achieve timely reperfusion.18 28
A key factor determining patient outcome in STEMI is total ischaemic time.1 The ischaemic time elapsed during the EMS phase varies widely among systems, and about 50% of the studies had call-to-door time >50 min. For patients who received a PCI reperfusion strategy, shorter EMS delays were not significantly associated with lower mortality. Lack of mortality benefit in this study may be due to a number of reasons including an inability to control for risk factors without individual-level data and the limited number and quality of studies reporting the impact of EMS delay on mortality. However, the impact of EMS delay on mortality may be elucidated by the benefit of early presentation to PCI centres.29 30 Consistently with patient delay and hospital delay, reduction in EMS delay may eventually reduce total ischaemic time and translate into better patient outcomes.31
Limitations
This study has a number of limitations. The means and SDs of many studies were estimated assuming a normal distribution. Modest skewness was observed in a number of studies, which is unlikely to impact the results of the meta-analysis with such a large population. Furthermore, there were no significant differences in the weighted mean FMC-to-door time between studies that reported mean and studies that reported median (n=20; weighted mean 39.8; 95% CI 34.2 to 45.3 vs n=29; weighted mean 42.1; 95% CI 39.6 to 44.5; p=0.7).
We did not perform quality assessment of the included studies because EMS intervals were rarely reported as the primary outcome of the study. In addition, quality assessment typically compares exposure and control groups with respect to patient selection, risk of bias and comparability,32 which are not relevant in our review. Our estimates were derived mainly from observational studies, and data of EMS intervals are subject to reporting bias because they were mainly self-reported by ambulance clinicians. Finally, the study was limited to published English-language studies, and therefore, our global estimates may be subject to publication bias.
Conclusion
Many STEMI patients remain in the EMS phase for extended time, approximately the first half of the total system delay. There are global and regional variations in EMS delays in STEMI patients that can be explained, in part, by a few factors. EMS delay is likely to be associated with time to treatment, and accordingly it may translate into poorer patient outcomes.
Several regions and systems have an unexplained longer EMS delay and treatment times, suggesting that there continue to be opportunities for improvement. Further quality improvement interventions are likely required to minimise EMS delay to meet standards of care. Our study provides several insights and time measures that may be useful in future initiatives aimed at quality improvement.
Key messages
What is already known on this subject?
Many patients with ST-elevation myocardial infarction (STEMI) who present to emergency medical services (EMS) fail to meet optimal time-to-treatment targets.
While significant efforts have been made to reduce hospital-related system delays (ie, door-to-balloon time), comparatively little attention has been given to evaluate and improve EMS system delays in patients with STEMI.
What might this study add?
This meta-analysis involving 100 studies from 20 countries shows that EMS delays in STEMI vary substantially around the world, and are partly associated with a number of system characteristics.
Longer EMS delays are associated with a significant reduction in the proportion of patients treated within 90 min of first medical contact.
Shorter EMS delays to prehospital thrombolysis were associated with lower short-term mortality.
How might this impact on clinical practice?
EMS agencies could play an important role in reducing unnecessary system delays in STEMI, which could yield improvements in patient outcome.
References
Footnotes
Contributors AA, ZN and DS conceived the study. AA and ZN designed the search strategy and performed the study selection and data extraction. AA conducted the meta-analysis. The manuscript was drafted by AA and all authors made revisions for intellectual property.
Funding ZN is supported by a National Health and Medical Research Council (NHMRC) Early Career Fellowship (#1146809). DS is supported by NHF fellowship and viertel foundation award.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Not required.