Article Text

Abstract
Objective The association with B-type natriuretic peptide (BNP), disease progression and outcomes in patients with atrial fibrillation (AF) has not been thoroughly investigated.
Methods We evaluated the association between BNP levels and outcomes, including AF progression, composite outcome of major adverse cardiovascular or neurological events (MACNE) and major bleeding, via pooled logistic regression and Cox frailty models in Outcomes Registry for Better Informed Treatment of Atrial Fibrillation II registry. AF progression was defined as either paroxysmal becoming persistent or permanent, or persistent becoming permanent at any follow-up.
Results Among 13 375 patients with AF, 2797 with BNP values at baseline (median age (IQR), 72.0 (63.0–80.0) years; 43.0% women; median BNP, 238 (102–502) ng/L; 42.3% prior heart failure) were included in the models evaluating the association between BNP levels and MACNE or major bleeding. Of these, 1282 patients with paroxysmal or persistent AF at baseline were analysed in AF progression model. The likelihood of AF progression (adjusted OR, 1.11 for every 100 ng/mL; 95% CI 1.03 to 1.19) and MACNE (adjusted HR, 1.11 for every doubling in BNP values; 95% CI 1.01 to 1.22) increased with BNP concentration, while the elevated BNP values were not associated with increased risks of major bleeding. BNP values improved the risk prediction of AF progression and MACNE when added to conventional risk estimates.
Conclusions BNP levels are associated with increased risk of AF progression and cardiovascular outcomes in patients with AF. Further studies are required to assess whether biomarker-based risk stratification improves patient outcomes.
Clinical trial registration NCT01701817.
- atrial fibrillation
Statistics from Altmetric.com
Introduction
Risk stratification is an important step in the evaluation of patients with atrial fibrillation (AF). Current guideline-recommended risk prediction tools like the CHA2DS2-VASc score are limited by modest discriminatory power and focused application to the prediction of ischaemic stroke despite a preponderance of other adverse cardiovascular events that can impact patients with AF, including increased risks of heart failure (HF) and all-cause mortality.1–3
AF is both an electrical and a myocardial disorder in which electrical and structural remodelling facilitates its progression from paroxysmal to more persistent forms of AF.4 While most patients with AF require stroke prevention therapy, more persistent forms of AF are associated with even higher risks of stroke, HF and mortality after adjusting for the CHA2DS2-VASc score and other comorbidities.5–7 Therefore, predicting and preventing progression of AF may also be an important factor in the evaluation and management of AF, particularly patients who require rhythm control therapy.
In patients with HF, assessments of B-type natriuretic peptide (BNP) improve diagnosis, risk stratification, and may also facilitate treatment selection.8 Data from clinical trials suggest that elevated BNP values are associated with increased risks of stroke and mortality in patients with AF.9–11 It is not known if BNP predicts AF disease progression or clinical outcomes in daily practice outside of controlled clinical trials. Using the national, multicentre Outcomes Registry for Better Informed Treatment of Atrial Fibrillation II (ORBIT-AF II) registry, we sought to evaluate the association of BNP values with disease progression and clinical outcomes in patients with AF.
Methods
Data source and study population
The cohort for this analysis was derived from the ORBIT-AF II registry.12 Briefly, ORBIT-AF II is a prospective, multicentre nationwide registry of patients with AF from 244 US sites. ORBIT-AF II enrolled only patients who either have a new diagnosis of AF within the previous 6 months or were started on a non-vitamin K antagonist oral anticoagulant for AF within the previous 3 months. Moreover, eligible patients had to be able to adhere to local follow-up every 6 months. Patients with AF due to a reversible cause, solitary atrial flutter without AF or a life expectancy of less than 6 months were excluded. A web-based case report form was used to collect information on patient demographics, medical and surgical history, medications, vital signs, laboratory data and imaging and electrocardiographic parameters. Changes in pharmacotherapy, cardiac rhythm and subsequent cardiovascular events and procedures were identified through medical record review at study visits at approximately 6-month intervals.
For the purpose of this analysis, we included patients with BNP or N-terminal pro-BNP (NT-proBNP) values at the time of enrolment. The decision to evaluate BNP or NT-proBNP values was at the discretion of the treating physician, and blood samples were analysed according to the protocol of each institute.
Definitions
Since patients may have had either BNP or NT-proBNP level obtained, for standardisation purpose of this study, NT-proBNP was converted to BNP using the following equation: log10(NT-proBNP)=1.1×log10(BNP)+0.570.13 The primary outcome measure was AF progression which was defined as either (A) paroxysmal AF at baseline becoming persistent or permanent AF at any follow-up, or (B) persistent AF at baseline becoming permanent at any follow-up. Paroxysmal AF was defined as recurrent AF episodes that terminated spontaneously within 7 days; persistent AF was defined as recurrent AF that was sustained for more than 7 days; permanent AF was defined as continuous AF in which the presence of the AF was accepted by the patient and physician.14 AF converted to sinus rhythm by cardioversion within 7 days was treated as persistent AF. Secondary outcomes included major adverse cardiovascular or neurological events (MACNE) and major bleeding. MACNE was defined as the occurrence of cardiovascular death, myocardial infarction, new-onset HF, stroke/non-central nervous system systemic embolism or transient ischaemic attack. Major bleeding was defined by the International Society of Thrombosis and Haemostasis criteria.15
Statistical analysis
Patients were categorised into tertiles on the basis of BNP values at enrolment, and demographics were compared among tertiles using the Kruskal-Wallis test for continuous variables and the Χ2 test for categorical variables. In the subgroup of patients with Holter monitor information, the association between tertiles of BNP values and AF burden detected by Holter monitor was evaluated using the Χ2 test. AF burden was expressed as per cent time in AF and categorised into three groups (AF≤1%, 1%<AF≤90%, AF >90%).
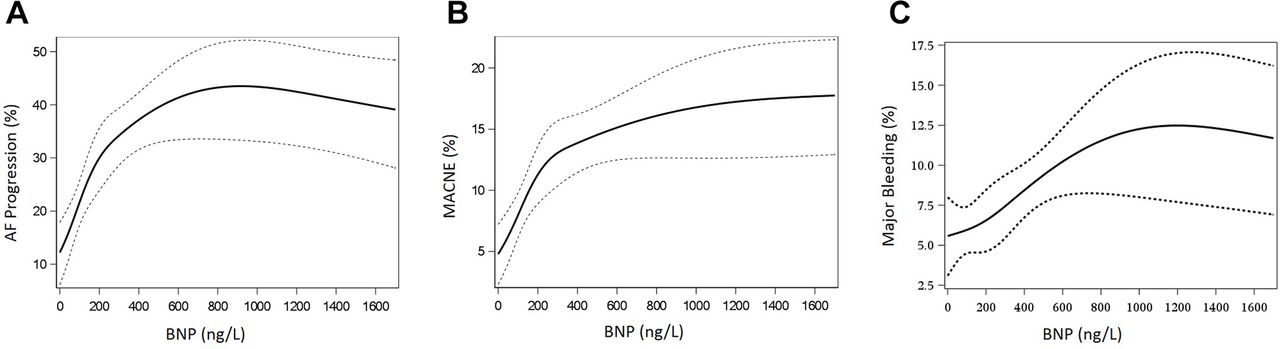
We assessed the association between continuous BNP values and AF progression in those with paroxysmal or persistent AF at baseline using pooled logistic regression to account for differential follow-up duration. The linearity assumption was violated between continuous BNP values and AF progression; therefore, linear splines with 1 knot at 800 ng/L were used (figure 1A). Patients within a site are likely to be treated more similarly than patients from a different site. Generalised estimating equations were used to account for this within-site source of variation. Previously identified risk factors for AF progression were adjusted in the model (online supplementary eAppendix 1).16–18 Adjusted association was displayed as odds ratio (OR) and 95% confidence intervals (CIs).
Supplemental material

Spline relationship between continuous BNP values and clinical outcomes (AF progression (A), MACNE (B) and major bleeding (C)). AF, atrial fibrillation; BNP, B-type natriuretic peptide; MACNE, major adverse cardiovascular or neurological event.
Subsequently, to determine whether BNP values were independently associated with clinical outcomes, Cox frailty models were used. MACNE, its individual components and major bleeding were evaluated. Since non-linear relationship between continuous BNP and MACNE and major bleeding was observed (figure 1B,C), continuous BNP was included in the models as a log-transformed continuous variable. Models were adjusted for all covariates listed in the online supplementary eAppendix 2 that were identified by backward selection with a retention criterion of α=0.05 using candidate variables listed in the online supplementary eAppendix 3 as starting covariates in the previous study.19 Importantly, to account for HF status, systolic and diastolic blood pressure, heart rate, New York Heart Association class and left ventricular ejection fraction were included in the models. In addition, to account for the effect of medication on BNP and MACNE, beta-blocker, renin-angiotensin blockade therapy and loop diuretic were included in the model. Adjusted associations were reported as hazard ratio (HR) and 95% CIs.
As a sensitivity analysis, the analyses were replicated using tertiles of BNP values instead of continuous BNP values and when confined to patients whose natriuretic peptide values were measured by BNP.
Additionally, prespecified subgroup analyses were performed for the following: patients with versus without HF, with versus without chronic kidney disease (defined by an estimated glomerular filtration rate less than 60), with versus without advanced age (≥75 years), men versus women, lower CHA2DS2-VASc score (0–2) versus higher (≥3) and extent of left atrial enlargement (none or mild vs moderate vs severe). Finally, to determine whether the addition of BNP values to the models already containing existing risk scores (HATCH or CHA2DS2-VASc scores)16 20 would provide better predictability than those containing the current risk scores alone, a comparison of C-statistics with and without BNP values was performed.
All candidate variables had less than 1% of missingness except for functional class (8%). Data missing in the multivariable models were addressed using multiple imputations (online supplementary eAppendix 3). All continuous variables were tested for linearity, and appropriate non-linear relationships were applied. The deidentified, aggregate data were analysed by the Duke Clinical Research Institute using SAS software (V.9.3; SAS Institute).
Results
The ORBIT-AF II registry enrolled 13 375 patients with AF from February 2013 to July 2016 at 244 sites within the USA. Among them, 3352 patients had BNP or NT-proBNP values at the time of enrolment. After excluding patients with missing follow-up information (n=555), the remaining 2797 patients from 181 sites were analysed in this study (online supplementary eFigure 1). Median follow-up period was 360 (IQR 182–547) days.
Baseline characteristics
Among 2797 patients, the median BNP level was 238 ng/L (IQR 102–502). Over two-thirds of patients with AF have BNP levels >100 ng/L. Tertiles of BNP levels were ≤143, 144–383 and ≥384 ng/L. Baseline characteristics of the cohort (n=2797) according to tertiles of BNP values are shown in table 1. Patients with higher BNP values were older and more likely to have anaemia, chronic kidney disease, HF, reduced left ventricular ejection fraction and larger left atrial diameter.
Baseline characteristics stratified by BNP tertiles
BNP and AF burden
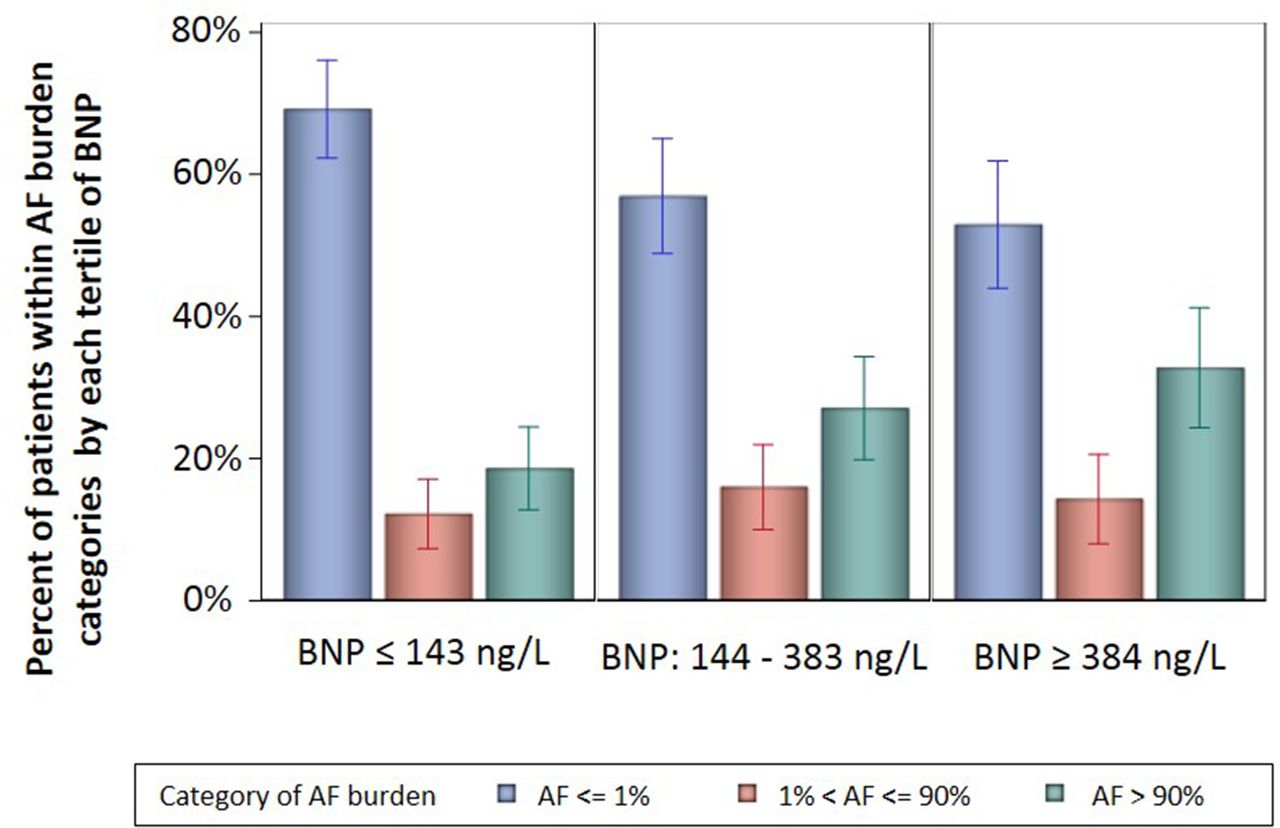
Among the analysis cohort, 537 (19.2%) patients also had Holter monitor data (online supplementary eFigure 1). AF burden on 24-hour Holter monitor according to tertiles of BNP is illustrated in figure 2. Among patients in the highest BNP tertile, 32.8% had AF >90% of the time during monitoring as compared with 18.6% in the lowest tertile (p=0.037). This association was consistent when considering BNP as a continuous variable (p=0.021).

Association between tertiles of BNP values and AF burden detected by Holter monitor AF burden was expressed as per cent time in AF and classified into three categories (AF burden ≤1% vs 1%<AF burden≤90% vs AF burden >90%) based on the distribution of AF burden. Since most patients had AF burden ≤1% or >90%, the intermediate range needed to be broad (1%<AF burden≤90%). X-axis has three segments, representing tertiles of BNP (BNP ≤143 ng/L vs BNP 144–383 ng/L vs BNP ≥384 ng/L), and in each BNP tertile, there are three bars corresponding to categories of AF burden (blue: AF burden ≤1%; red: 1%<AF burden≤90%; green: AF burden >90%). Y-axis indicates the per cent of patients within AF burden categories by each BNP tertile. Time difference between BNP measurement and Holter monitor was median 1 day (IQR: 0–23 days). AF, atrial fibrillation; BNP, B-type natriuretic peptide.
BNP and AF progression
After excluding patients with permanent AF or those with atrioventricular nodal ablation (n=1515), we identified 1282 patients with paroxysmal or persistent AF at baseline (online supplementary eFigure 1). Among them, 252 patients (19.7%) had AF progression during follow-up. The relationship between continuous BNP and AF progression is shown in figure 1A. While the risk of AF progression was greater with increasing BNP values up to 800 ng/L, an inverse association was observed when BNP was greater than 800 ng/L. AF progression increased with increasing BNP when BNP values were ≤800 ng/L and decreased as BNP increased when BNP values were >800 ng/L. This trend was consistent in all prespecified subgroups, and interactions of continuous BNP and HF were not recognised (P for interaction of HF=0.443) (table 2).
Adjusted association of the continuous BNP and AF progression
BNP and clinical outcomes
The relationship between continuous BNP and MACNE is shown in figure 1B, demonstrating the risk of MACNE was greater with increasing BNP values. Cox frailty models revealed that BNP was significantly associated with MACNE even after accounting for baseline differences, which was consistent in all prespecified subgroups, and a significant interaction of HF with continuous BNP was not found (P for interaction=0.50) (table 3). By contrast, the risk of major bleeding seemed to increase as BNP values increased (figure 1C); however, its relationship was no longer significant after the adjustment for the measured confounders (online supplementary eTable 1).
Adjusted association of the continuous BNP and MACNE
Sensitivity analyses
Sensitivity analyses when confined to patients whose natriuretic peptide values were measured by BNP allied with the main analyses (online supplementary eTables 2 and 3 and eFigure 2). In addition, when treating BNP as tertiles, the association between BNP values and clinical outcomes was consistent, and higher BNP levels were associated with increased risk of AF progression and MACNE (figure 3 and table 4).

{kind=link}
{kind=link}
{kind=link}
Cumulative incidence curves for MACNE stratified by tertiles of BNP values. BNP, B-type natriuretic peptide; MACNE, major adverse cardiovascular or neurological event.
Sensitivity analyses by treating BNP values as tertiles
Additive impact of BNP values on discrimination performance
Table 5 displays the discrimination performance of BNP alone, conventional risk scores alone and BNP paired with conventional risk scores. The discrimination performance of full predictive models for AF progression or MACNE alone, and BNP paired with full predictive models is also shown. Addition of BNP values to conventional risk scores improved model discrimination. BNP values also improved the risk prediction, even when added to full predictive models for AF progression or MACNE, although the incremental predictive value of BNP may be limited, given the slight increase in C-statistics.
Incremental predictive value of BNP values over pre-existing risk scores
Discussion
In this analysis between the association of BNP levels and disease progression and outcomes in patients with AF, there are four main findings. First, elevations in BNP were associated with the amount of AF on ambulatory monitoring. Second, BNP concentrations were associated with a greater likelihood of progression to more persistent or permanent forms of AF. Third, and perhaps most importantly, higher BNP values were associated with a higher risk for adverse outcomes including MACNE. Finally, our findings expand the notion that biomarker-based risk scores have better predictive performance than conventional risk scores in a less selected population.
Prior cohort substudies in randomised trials found that NT-proBNP levels were associated with increased risks for stroke and mortality even after adjusting for CHA2DS2-VASc risk factors.9 10 Furthermore, results from several clinical trials have suggested that biomarker-based risk scores in general have superior discrimination and performance for the prediction of stroke or death compared with traditional risk stratification scores.11 21–23 However, there are few data on the role of BNP in risk stratification outside of randomised trials. Our analyses extend and confirm these results in a nationwide registry recruited from community practices. In addition, there are no current data available about the association of BNP values and clinical outcomes other than stroke or death, such as AF progression and new-onset HF. Our findings provide further support for these associations and suggest that BNP values may become a useful tool for decision-making when considering interventions aimed at preventing and treating symptomatic HF in patients with known AF. Given the recent publication of the Catheter Ablation versus Standard Conventional Therapy in Patients with Left Ventricular Dysfunction and Atrial Fibrillation trial,24 the role of BNP will be highlighted for managing patients with AF.
In our observational cohort, patients with elevated BNP values had higher adjusted risk for AF progression. Most prior work has focused on the association between BNP concentrations and newly incident AF25 or postablation AF recurrence,26 while fewer studies have investigated BNP and AF progression. Ascertaining risk of AF progression may assume increased importance in patients with AF given the apparent decreased benefit of beta-blocker therapy in patients with AF and sustained AF.27 Previously, we have shown that AF on the baseline ECG, advanced age and higher heart rate were correlated independently with AF progression.17 The Euro Heart Survey on AF developed the HATCH score to evaluate future risk of AF progression. The HATCH score uses demographic and medical history and exhibits modest discrimination.16 Our data suggest that the addition of BNP values may aid in stratifying patient at risk for AF progression.
The magnitude of BNP elevation was also directly associated with AF burden over 24 hours as assessed by ambulatory monitoring. There are several potential mechanisms to account for the association between increased AF burden and BNP levels. While BNP is secreted predominantly from ventricular myocytes in patients with HF, prior work suggests that BNP release from the atrium occurs in patients with AF as a response to atrial stretch.28 29 Elevated BNP levels in AF may also reflect increased left atrial pressure and impaired left ventricular filling, independent of ventricular secretion of BNP. Since increased mechanical atrial stretch itself promotes atrial arrhythmia30 and maladaptive atrial remodelling,4 it would follow that BNP might predict both the frequency of arrhythmia and the propensity for disease progression. No significant interactions of BNP values and HF in our analysis support this hypothesis.
The influence of BNP values on the risk of AF progression and clinical outcomes could vary according to its baseline concentration. While the risk of AF progression was greater with increasing BNP values up to 800 ng/L, paradoxically when BNP was greater than 800 ng/L, there was an association with lower risk of progression. Similarly, the association of BNP values with MACNE was blunted in patients with higher BNP values. There are two potential explanations. As stated above, BNP release from the atrium occurs in patients with AF as a response to atrial stretch. However, patients with higher BNP values are more likely to have symptomatic HF (online supplementary eTable 4) and in these patients, BNP is predominantly secreted from ventricular myocytes. Although no significant interaction between BNP levels and HF status was confirmed in our analysis, the incremental contribution of BNPs secreted from atrium may be attenuated in patients with HF and may not necessarily reflect atrial remodelling and dysfunction. Furthermore, competing risk of death may reduce the risk of AF progression in patients with high BNP values. Given the strong association between elevated BNP and increased risk of death, patients with high BNP values are more likely to die before AF progress, resulting in the reduction in AF progression in this population.
Limitations
Our findings should be interpreted in the context of several potential limitations. First, BNP or NT-proBNP values were not available for about three-fourths of patients enrolled in the ORBIT-AF II registry. In our registry, the decision to evaluate BNP values was at the discretion of the treating physician. As a result, reflecting the current practice pattern of BNP testing, patients who had BNP levels drawn had higher CHA2DS2-VASc scores, more frequently had a history of HF than those without BNP values (online supplementary eTable 5). Therefore, our study population could be a biased sample, but, given the lack of real-world evidence, our observational findings will provide an important clinical insight that BNP testing could be useful for risk stratification in a daily clinical practice. Second, blood samples were not analysed by a unified protocol or kit, and at the core laboratory. Furthermore, NT-proBNP was converted to BNP using a previously published method and the conversion may lead to some variability.13 However, sensitivity analyses when confined to patients whose natriuretic peptide values were measured by BNP also demonstrated consistent findings, which supports the robustness of our findings (online supplementary eTables 2 and 3 and eFigure 2). Third, despite our use of a large number of characteristics to adjust for potential confounding, residual and/or unmeasured confounding may exist. Finally, statistical power might be insufficient, especially in the analyses evaluating the association between BNP and individual component of MACNE (table 4). Given the consistent trends to the previous works from the randomised trials,9 10 the lack of statistical significance may be due to the relatively small sample size and short follow-up period.
Conclusions
In this contemporary nationwide AF cohort, increased BNP was associated with increased AF burden, risk of AF progression and adverse clinical outcomes, especially cardiovascular death. The addition of BNP values improved the discrimination performance of current risk stratification systems in a less selected population. Further studies are required to assess whether biomarker-based risk stratification improves patient clinical outcomes.
Key messages
What is already known on this subject?
In clinical trials, elevated B-type natriuretic peptide (BNP) values are associated with increased risks of stroke and mortality in patients with atrial fibrillation (AF).
What might this study add?
BNP predicts clinical outcomes in daily practice outside of controlled clinical trials among patients with AF.
In patients with AF, elevated BNP values are associated with disease burden and progression as well as increased risk of adverse cardiovascular event.
The addition of BNP values to conventional risk scores, such as the HATCH and CHA2DS2-VASc scores, improves risk stratification.
How might this impact on clinical practice?
The addition of BNP values to current risk stratification systems may improve clinical decision-making and the BNP-based clinical decision-making could improve the clinical outcomes in patients with AF.
Acknowledgments
The authors acknowledge DaJuanicia N Holmes, MS (Duke Clinical Research Institute) for her statistical contributions.
References
Footnotes
Contributors TI and JPP had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. Study concept and design: TI, KP and JPP. Acquisition, analysis or interpretation of data: TI, SK, KP, RGB, LAA, GCF, BJG, MDE, PRK, JAR, GVN, PSC, KWM, DES, JVF, BAS, EDP and JPP. Drafting of the manuscript: TI, SK, KP and JPP. Critical revision of the manuscript for important intellectual content: SK, KP, RGB, LAA, GCF, BJG, MDE, PRK, JAR, GVN, PSC, KWM, DES, JVF, BAS, EDP and JPP. Statistical analysis: SK and KP. Obtained funding: JPP. Administrative, technical or material support: RGB and JPP. Study supervision: KP, EDP and JPP.
Funding This project was supported in part by cooperative agreement 1U19 HS021092 from the Agency of Healthcare Research and Quality, and JSPS Overseas Research Fellowship. The Outcomes Registry for Better Informed Treatment of Atrial Fibrillation is sponsored by Janssen Scientific Affairs. With the exception of Janssen Scientific Affairs, the funders had no role in the design and conduct of the study; collection, management, analysis and interpretation of data; preparation, review or approval of the manuscript; and decision to submit the manuscript for publication.
Competing interests TI: research grant from JSPS Overseas Research Fellowship and Boston Scientific. LAA: contract with Janssen and Novartis. GCF: consultant/advisory board support from Janssen Pharmaceutical. BJG: member of a Data Safety Monitoring Board for Mount Sinai St Lukes, Boston Scientific, Teva Pharmaceutical Industries, St Jude Medical, Janssen Research & Development, Baxter Healthcare and Cardiovascular Research Foundation; consultant/advisory board for Janssen Scientific Affairs, Cipla, Armetheon and Medtronic. MDE: consultant/advisory board for Boehringer Ingelheim, Diachi Sanko, Pfizer, Bristol-Myers Squibb and Janssen Scientific Affairs. PRK: consultant for Johnson & Johnson. JAR: research grant from Janssen Pharmaceuticals; research support from Boehringer Ingelheim Pharmaceuticals and GlaxoSmithKline; consultancies with Sanofi, Gilead Sciences, CV Therapeutics, GlaxoSmithKline, Merck & Co, Cardiome Pharma, Boehringer Ingelheim Pharmaceuticals and Medtronic; speakers’ bureau income from Sanofi and Boehringer Ingelheim Pharmaceuticals. GVN: research grant from Janssen; consultant/advisory board for Janssen and Daiichi Sankyo. PSC: employee of Janssen; consultant for Optum Rx and Johnson & Johnson. KWM: financial disclosures can be viewed at http://med.stanford.edu/profiles/kenneth-mahaffey. DES: consultant/advisory board for Boehringer Ingelheim, Bristol-Myers Squibb, Merck, Johnson & Johnson, Pfizer and Medtronic; research grants from Boehringer Ingelheim and Bristol-Myers Squibb. JVF: consultant/advisory board for Janssen Scientific. BAS: research support from Boston Scientific and Janssen; consult for Janssen; speakers’ bureau income from Biosense Webster. EDP: research grant from Janssen Pharmaceuticals and Eli Lilly; consultant for Janssen Pharmaceuticals and Boehringer Ingelheim. JPP: research grant from Agency for Healthcare Research and Quality, ARCA Biopharma, Boston Scientific, Gilead Sciences, Janssen Pharmaceuticals, Johnson & Johnson, ResMed, Spectranetics and St Jude Medical; consultant/advisory board for BMS/Pfizer, GlaxoSmithKline, Janssen Pharmaceuticals, Johnson & Johnson, Medtronic and Spectranetics. SK, KP, and RGB have no relationship(s) to disclose.
Patient consent Not required.
Ethics approval The study was approved by the institutional review board at Duke University (the coordinating centre) and each participating centre obtained local institutional review board approval.
Provenance and peer review Not commissioned; externally peer reviewed.