Article Text

Abstract
Objective Obesity is paradoxically associated with enhanced survival in patients with established cardiovascular disease. We explored this paradox further by examining the influence of obesity on survival in patients with verified atherosclerotic heart disease.
Design and patients This retrospective registry based cohort study included all patients from the Western Denmark Heart Registry with coronary atherosclerosis confirmed by coronary angiography from January 2000 to December 2010. Patients were divided into eight groups according to body mass index (BMI) based on WHO BMI classification.
Setting Department of Cardiology, Copenhagen University Hospital Gentofte, Hellerup, Denmark.
Results The study included 37 573 patients (70.7% men) with a mean age of (66.3±11.1) years. During the 11 years of follow-up, 5866 (15.6%) patients died. Multivariable analysis confirmed that the risk of death was the lowest among the preobese patients (27.5≤BMI<30 kg/m2) with adjusted HR of 0.82 (95% CI 0.71 to 0.95; p=0.008) and increased with both low (BMI<18.50 kg/m2) and very high (BMI≥40 kg/m2) BMI, HR 2.04 (95% CI 1.63 to 2.57; p<0.001) and HR 1.35 (95% CI 1.05 to 1.72; p<0.01), respectively. Also the normal weight class I (18.5≤BMI<23 kg/m2) had a significant risk of mortality HR 1.28 (95% CI 1.13 to 1.45; p<0.001). Obese classes I and II did not differ from the reference group (23≤BMI<25 kg/m2).
Conclusions Overweight atherosclerotic heart disease patients have improved survival compared with normal weight patients. Underweight and severely obese patients have increased mortality. Our results lean more towards an overweight paradox than an obesity paradox.
Statistics from Altmetric.com
Introduction
While obesity is a major risk factor for cardiovascular disease, a range of studies have demonstrated that obesity paradoxically is associated with improved survival in patients with established cardiovascular disease.1–4 Further exploration of this paradox is relevant as current guidelines recommend weight loss for overweight and obese patients with cardiovascular disease.5
Obesity has been linked to better prognosis in dialysis patients in early 1980s but the obesity paradox phenomenon was first demonstrated in studies of patients with coronary artery disease where underweight and normal weight patients had higher death rate than obese patients.6 ,7 Subsequently, the obesity paradox has been found in patients with high age, hypertension, atrial fibrillation, kidney disease, rheumatoid arthritis, chronic obstructive lung disease and atherosclerotic cardiovascular disease.1 ,8–10
A meta-analysis of 40 studies with 250 152 patients with coronary heart disease and 3.8 years of follow-up showed that overweight and obese patients had reduced risk of death compared with underweight and normal weight patients.11 A more recent study could not confirm the existence of the obesity paradox in extremely obese patient with ST-segment elevation myocardial infarction (MI).3
The available contradictory data demonstrate a need for further studies including studies with longer follow-up. We therefore conducted a large retrospective study to explore the association between obesity and risk of death in patients with coronary atherosclerosis documented by coronary angiography.
Methods
All citizens in Denmark have a unique identification number which facilitates individual-level linkage between different registries. We combined data collected in relation to coronary angiography and subsequent hospitalisations and deaths. This retrospective study is based on information from several Danish registries.
The Western Denmark Heart Registry (WDHR) is a clinical database within the Danish healthcare system that includes all adult patients referred for cardiac intervention in western Denmark, a population of 3.3 million people.12 The Danish Civil Registry keeps complete information on vital status for all inhabitants.
We also used the Danish National Patient Registry which keeps records of all hospital admissions in Denmark since 1978 with one primary diagnosis and, if applicable, one or more secondary diagnoses, according to the International Classification of Diseases.13
The population
We included all patients in WDHR diagnosed with coronary atherosclerosis by coronary angiography from 1 January 2000 to 31 December 2010. If patients had more than one coronary angiography during the time period, we included the patients on the date of the first registered coronary angiography. All patients with one, several or diffuse vessel disease were included. Vessel disease was defined as presence of focal coronary artery lesions with diameter stenosis ≥50% or diffusely diseased vessels by visual assessment.
Data about degree of vessel disease, left ventricular ejection fraction (LVEF), prior MI and patient specific characteristics were registered in the WDHR database at the time of the coronary angiography. Patients with missing information about height, weight, degree of the vessel disease or without permanent residence in Denmark were excluded. We also excluded all patients with a history of prior cardiac surgery or percutaneous coronary intervention. A patient on antihypertensive or statin treatment was considered as hypertensive or hyperlipidaemic.
Body mass index (BMI) was calculated as weight in kilograms divided by square of height in metres (kg/m2). We used WHO BMI classification of underweight, normal weight, overweight/preobese and obesity including WHO additional cut-off points within each weight group (http://apps.who.int/bmi/index.jsp?introPage=intro_3.html) to allow detailed analysis. Patients were thus divided into eight groups according to BMI. The underweight group had a BMI<18.5 kg/m2; normal weight was divided into two classes, normal weight class I: 18.5≤BMI<23 kg/m2 and normal weight class II: 23≤BMI<25 kg/m2 (this group was selected as the reference group). The overweight/preobese patients were divided into two classes, class I: 25≤BMI<27.5 kg/m2 and class II: 27.50≤BMI<30 kg/m2. Finally, the obese patients were classified in three classes: obese class I: 30≤BMI<35 kg/m2, obese class II: 35≤BMI<40 kg/m2 and the severely obese patients in obese class III: BMI≥40 kg/m2.
Statistical analyses
Categorical variables are presented as numbers and percentages and continuous variables as means with SD. Time to event curve was generated by using Kaplan–Meier estimates.
We used survival analysis to estimate the difference in survival in the eight groups of BMI. Outcome was all-cause mortality. Follow-up started on the day of the coronary angiography and ended on 31 December 2010.
Cox proportional hazard models were used to estimate HR with 95% CI in the eight groups based on BMI. The models were adjusted for the following variables: age, sex, smoking, diabetes, degree of vessel disease, hypertension, hyperlipidaemia, serum creatine, LVEF, arrhythmia, periphery vascular disease, cerebral vascular disease, chronic obstructive lung disease, cancer and prior MI. Model assumptions were tested and found valid unless otherwise indicated. Further, we performed an interaction analysis between BMI groups and smoking groups in which we did not find any interaction (p=0.45).
All statistical analyses were performed with the SAS statistical software V.9.2 (SAS Institute Inc., Cary, North Carolina, USA) and Stata software V.11 (Statacorp, College st., Texas, USA).
The Danish Data Protection Agency approved the study, and data were made available to us in such a way that individuals could not be identified. Retrospective registry based studies do not require ethical approval in Denmark.
Results
A total of 100 128 patients underwent coronary angiography from 1 January 2000 to 31 December 2010 (figure 1). We excluded 29 583 (29.5%) patients due to missing information about BMI (there was no difference between the excluded patients and the included patients at baseline). Furthermore, we excluded 26 758 (26.7%) patients in whom coronary atherosclerotic disease was ruled out by angiography as well as 738 (0.7%) patients without permanent residence in Denmark and 5476 (5.5%) patients with a history of prior cardiac surgery or percutaneous coronary intervention. The final study population comprised 37 573 patients with coronary atherosclerotic disease.
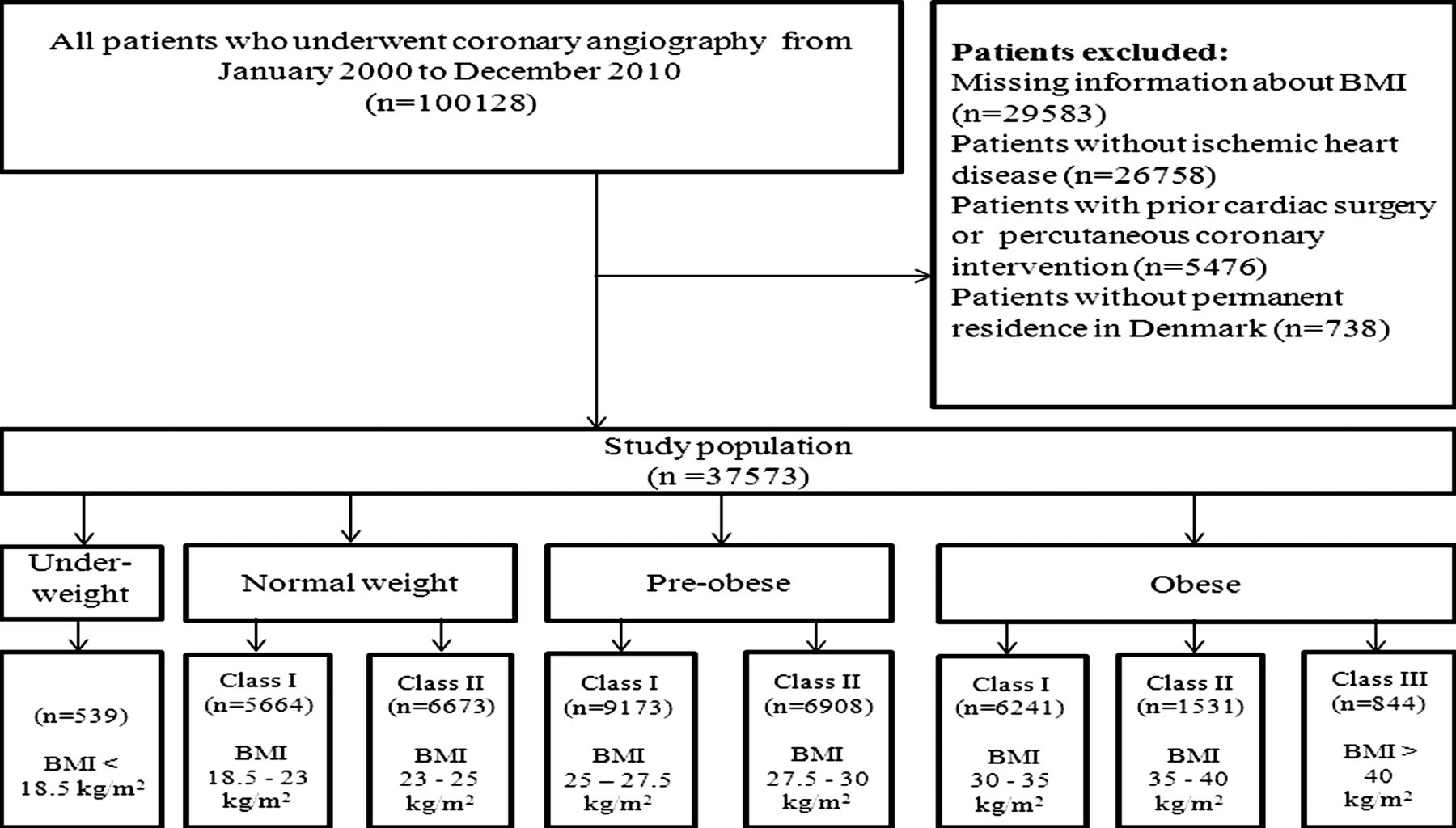
Flow diagram of the population. BMI, body mass index.
Baseline characteristics are presented in table 1. The mean age was 66.3 (±11) years and 26 540 (70.7%) were men. Patients in the obese groups were younger than patients in the other groups while the underweight group had the highest mean age. There were more male than female subjects in all groups except in the underweight group. Nearly a third of the population was current smokers and more than a third ex-smokers. As BMI increased, an increasing part of patients had prior MI or diabetes and an increasing number of patients were treated for dyslipidaemia or hypertension. Overall, underweight and severely obese patients (obese class III) had more comorbidity than the rest of the weight groups.
Baseline characteristics
During the 11 years, 5866 (15.6%) patients died. Median follow-up time was 3.2 years (IQR 1.4–5.3). The underweight patients (BMI<18.50 kg/m2) had the highest incidence rate of death: 133 (95% CI 115.3 to 153.1) per 1000 patient-years while the preobese patients (overweight class II, 27.5≤BMI<30 kg/m2) had the lowest incidence rate: 33 (95% CI 31.0 to 35.5) per 1000 patient-years (table 2).
Death rate stratified by BMI class per 1000 patient- years
The Kaplan–Meier estimates (figure 2) show the survival in the eight BMI groups. The underweight group (BMI<18.5 kg/m2) had the highest mortality while the preobese (class II, 27.5≤BMI<30 kg/m2) had the lowest mortality. After 8 years, 70% of the normal weight patients (class II, 23≤BMI<25 kg/m2) and 75% of the preobese (class II: 27.50≤BMI<30 kg/m2) patients were still alive, while only 40% of the underweight patients and less than 70% of the severely obese (obese class III BMI≥40 kg/m2) patients were alive.

Kaplan–Meier analysis of risk of all-cause death by body mass index (BMI) groups. This figure is only reproduced in colour in the online version.
Multivariable analysis
Figure 3 shows the results of the Cox proportional hazards regression analysis of all-cause death for each BMI group. There was a 2.04 (95% CI 1.63 to 2.57; p<0.001) times risk of death for the underweight group (BMI<18.5 kg/m2) compared with the reference group of normal weight class II (23≤BMI<25 kg/m2). The preobese (27.50≤BMI<30 kg/m2) had a decreased risk with an HR of 0.82 (95% CI 0.71 to 0.95; p=0.008). The normal weight (class I: 18.5≤BMI<23 kg/m2) had notable risk of death HR 1.28 (95% CI 1.13 to 1.45; p<0.001). The severely obese (obese class III: BMI≥40 kg/m2) patients had an increased HR of 1.35 (95% CI 1.05 to 1.72; p=0.016).

{kind=link}
{kind=link}
{kind=link}
Association between body mass index (BMI) and risk of all-cause death. Adjusted for: age, sex, smoking, diabetes, degree of vessel disease, hypertension, hyperlipidaemia, serum creatine, left ventricle ejection fraction, arrhythmia, periphery vascular disease, cerebral vascular disease, chronic obstructive lung disease, malignancy, cancer and prior myocardial infarction.
Discussion
In this long term follow-up study on patients with documented coronary arteriosclerotic disease, we demonstrated that preobese patients (overweight) (27.5≤BMI<30 kg/m2) had significantly better survival compared with patients with high-end normal weight (class II: 23≤BMI<25 kg/ m2), whereas low-end normal weight (class I: 18.5≤BMI<23 kg/m2) and severely obese patients (obese class III: BMI>40) had increased risk of death compared with the high-end normal weight (class II: 23≤BMI<25 kg/m2) during up to 11 years of follow-up. The results indicated a ‘J’ shaped risk curve pointing more towards an overweight paradox than obesity paradox, as the extremely obese had increased risk. Similar results have been reported in other studies by Romero-Corral et al and recently by Angeras et al14 and Romero-Corral et al who found a ‘J’-shaped risk curve of cardiovascular mortality, while their results for total mortality in all subgroups including patients with MI, percutaneous coronary intervention and coronary artery bypass grafting were insignificantly ‘J’-shaped.11
The association between obesity and mortality in patients with cardiovascular disease was first described in the late 1990s. But already in 1980s, the obesity was linked to improved survival in dialysis patients.6 ,7 Horwich et al15 investigated the role of obesity in 1203 heart failure patients between 16 and 82 years of age and found that obese patients had improved survival.
Recently, a study of Lancefield and colleagues based on patients undergoing percutaneous coronary intervention (PCI) found improved survival in a group of obese patients after 1 year follow-up.4 In contrast, Kadakia and colleagues2 reported significantly lower risk of cardiovascular death after 30 days, but not after 1 year in obese patients with acute coronary syndrome. In our study, with a median follow-up of 3.2 years, the preobese (class II: 27.5≤BMI<30 kg/m2) had better survival compared with high-end normal weight (class II, 23≤BMI<25 kg/m2). Similar to our results, a meta-analysis from 2006 including 250 152 patients with coronary artery disease showed that underweight patients had an increased relative risk of total mortality (1.37 95% CI 1.32 to 1.43) as well as the overweight (BMI 25–29.9 kg/m2) had decreased total mortality (0.87 95% CI 0.81 to 0.94).11 Unfortunately, several of the included studies did not provide information of whether the obesity paradox was consistent over time.
In our analysis, we divided our participants in eight BMI groups according to the classification provided by WHO, that is, underweight, normal weight, overweight and obesity and including WHO subdivision in groups. This approach gave us the possibility of a more differentiated analysis of the risk in the different BMI classes. Therefore, we could demonstrate that patients with low-end normal weight (class I: 18.5≤BMI<23 kg/ m2) as well as the underweight patients (BMI<18.5 kg/m2) had decreased survival compared with patients with high-end normal weight (class II, 23≤BMI<25 kg/m2). This might be explained by the fact that these patient groups might have undiagnosed comorbidity not captured by the registries at baseline such as cancer, arrhythmia, peripheral or cerebral vascular disease, chronic obstructive lung disease and heart failure. It is possible that these groups were in a phase of weight loss because of severe disease. Individuals with 18.5≤BMI<25 kg/m2 are considered to have a normal weight. Here, we demonstrated that patients with 23≤BMI<25 kg/m2 had better prognosis than patients with 18.5≤BMI<23 kg/m2. This also supports our assumption that this group of patients was the correct reference group in our study.
Also, we found that the severely obese patients (obese class III, BMI≥40 kg/m2) had an HR 1.35 increase in risk of death whereas obese class II (35≤BMI<40 kg/m2) had no significantly increased risk of death and obese class I (30≤BMI<35 kg/m2) had an insignificantly reduced risk of death.
Das and colleagues found similar results among patients with ST-segment elevation MI, where the obese class III patients had higher mortality odds than normal weight and obese class I patients.16 Different studies explored the obesity paradox by other measurement for fatness like waist circumference (WC), body fatness and lean mass index BMI and demonstrated the existence of an obesity paradox. In contrast, our results rejected the obesity paradox and showed advanced risk of death in obese class III with BMI>40 kg/m2.17–19 Thus, our results indicate that we may face an overweight/preobese paradox in patients with ischaemic heart disease rather than the more extreme obesity paradox with ever declining mortality as obesity increases. A recent Swedish paper on the obesity paradox reported better survival for overweight and obese patient, but their choice of reference group differed from ours, as we used our normal weight group with BMI between 23 and 25 as our reference contrasting to theirs with BMI between 21 and 23.5.14 We assumed that the most ‘healthy’ patient group might be patients with BMI between 23 and 25, but even with this group as reference the overweight/preobese group had lower risk. This may reflect that patients with cardiovascular disease are healthier, when the BMI is between 25 and 30 kg/m2. This is highly relevant since European guidelines on cardiovascular disease prevention state that weight reduction is recommend for obese patients and should be considered for those who are overweight (25≤BMI<30 kg/m2).5 The assumption that weight reduction in this group of patients would lead to better prognosis is not based on evidence.
Several explanations for the obesity paradox phenomena have been suggested. In a number of studies, obesity has been pointed out as the most important risk factor for hypertension, coronary heart disease, diabetes mellitus, dyslipidaemia, metabolic syndrome and sleep apnoea.1 ,3 ,20 Therefore, obese individuals may have relations to the health system earlier and benefit from preventive treatment. Other suggested explanations for the obesity paradox include whether BMI is an accurate measure of adiposity. We used BMI as measurement for adiposity, while Kadakia and colleagues2 used both BMI and WC in their analysis and described similar outcomes in BMI and WC groups. A similar study has been performed in a heart failure cohort by Clark et al,17 who examined all-cause mortality in relation to BMI and WC. They reported better survival in both high WC and high BMI groups; furthermore, the combination of high BMI–high WC showed low risk compared with normal BMI–WC.17 A meta-analysis reported that waist to height ratio is a better measurement than BMI for obesity-related cardiometabolic risk.21 A recent study on the association of different measures of obesity and mortality reported that high BMI is not directly associated with mortality and suggest that WC and waist to height ratio is a more reliable mortality risk parameter in coronary artery disease.22
However, BMI is a widely available, simple and practical obesity measurement and numerous studies have used BMI as proxy for adiposity.3 ,11 ,23 ,24
Strengths and limitations
The strengths of this study include that we used a large sample size of a population of unselected patients with atherosclerotic cardiovascular disease confirmed by coronary angiography. Our cohort was from WDHR which includes procedure data for all interventions in western Denmark and thus we minimised the risk of selections bias by not including specific hospitals, age groups or health insurance systems. We furthermore included a wide range of comorbidities in our analysis which gave us more reliable risk estimates. Another strength is the high accuracy of a diagnosis of ischaemic heart disease which in this study was based on a coronary angiography.
There are several limitations of our study, including that our study was conducted in a primarily Caucasian population and generalisation of results to other racial and ethnic groups should be done with caution. We were also missing information about LVEF and serum creatine in respectively 47% and 20% of our population, which limited the analysis including those variables. However, the missing values of LVEF were equally distributed between different BMI groups. We unfortunately did not have information about alcohol intake. Another limitation of our study is lack of information on fitness or physical activity level. This may be an important confounder since a recent study reported that obese patients with coronary artery disease and low cardiorespiratory fitness are associated with increased mortality.25
Conclusions
Patients with documented atherosclerotic heart disease who are overweight/preobese have improved survival compared with patients with normal BMI. Severely obese and underweight patients have increased mortality. If there is a weight paradox for this group of patients, it is an overweight paradox rather than an obesity paradox.
Another analysis
Subgroups of obese class III
We divided our obese class III in two groups (40≤BMI<45 kg/m2 and BMI>45 kg/m2) to allow further analyses. Our finding was that the group with BMI between 40 and 45 kg/m2 had higher risk HR 1.49 (95% CI 1.00 to 2.24; p=0.048) compared with the reference group. For patients with BMI over 45 kg/m2, we found an HR of 1.28 (95% CI 0.95 to 1.72; p=0.095).
To explore the underweight group of patients further, we performed an analysis where we excluded patients who died during the first 2 years of follow-up, as those patients might suffer from severe pre-existing health problems. The multivariate analyses showed that the underweight group had significant risk of death HR 2.05 (95% CI 1.37 to 3.07; p<0.001), and the preobese group (27.5≤BMI<30 kg/m2) had a non-significant decreased risk HR 0.86 (95% CI 0.69 to 1.06; p=0.17). Our obese groups had insignificantly increased risk.
Goel et al25 found that low fitness was associated with a high risk of death and higher fitness level insignificantly related to better prognosis. McAuley and colleagues also excluded those patients who died during the first 2 years of follow-up period. Their results did not differ from their main findings. Furthermore, they reported that high fitness level was associated with better survival within each BMI group and that overweight patients with high fitness levels had the lowest risk of death.26
References
Footnotes
-
Contributors All authors contribution to the study conception, design and interpretation. LT, LOJ, PT, JR, H-HT and JFL contributed to data collection. AA had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. AA made the primary contribution to interpretation of results and writing of the manuscript. All authors contributed to interpretation of results, revising the manuscript critically for important intellectual content and all approved the final manuscript.
-
Funding This work was supported by the Department of Cardiology, Copenhagen University Hospital Gentofte.
-
Competing interests None.
-
Ethics approval In Denmark, registry based studies do not require approval from Ethics Committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.