Article Text

Abstract
Background Many patients delay or interrupt dual antiplatelet therapy (DAT) after drug-eluting stent (DES) implantation, which increases the risk of stent thrombosis and death.
Objective To test the hypothesis that simple telephone contact made by nurses would improve adherence to and persistence of DAT.
Design Randomised controlled trial.
Patients and intervention A total of 300 patients (mean±SD 64±10 years, 73% male) were recruited immediately after DES implantation performed between June 2009 and June 2010. The last patient recruited reached the 1-year follow-up time point in June 2011. Patients were randomised to one of two groups: intervention, with four telephone follow-ups, versus a control group. In the intervention group, phone calls were made within 7 days of the DES implantation and at 1, 6 and 9 months to support drug adherence. Control patients were followed as per usual clinical practice. Pharmacy data were collected to assess drug prescription filling and refill.
Setting Tertiary care university cardiovascular centre and community.
Main outcome measures The primary end point was the proportion of days covered with aspirin and clopidogrel over the year after discharge as assessed by pharmacy refill data. Secondary outcome measures included persistence of aspirin and clopidogrel treatment, defined as no gaps longer than 14 days during follow-up.
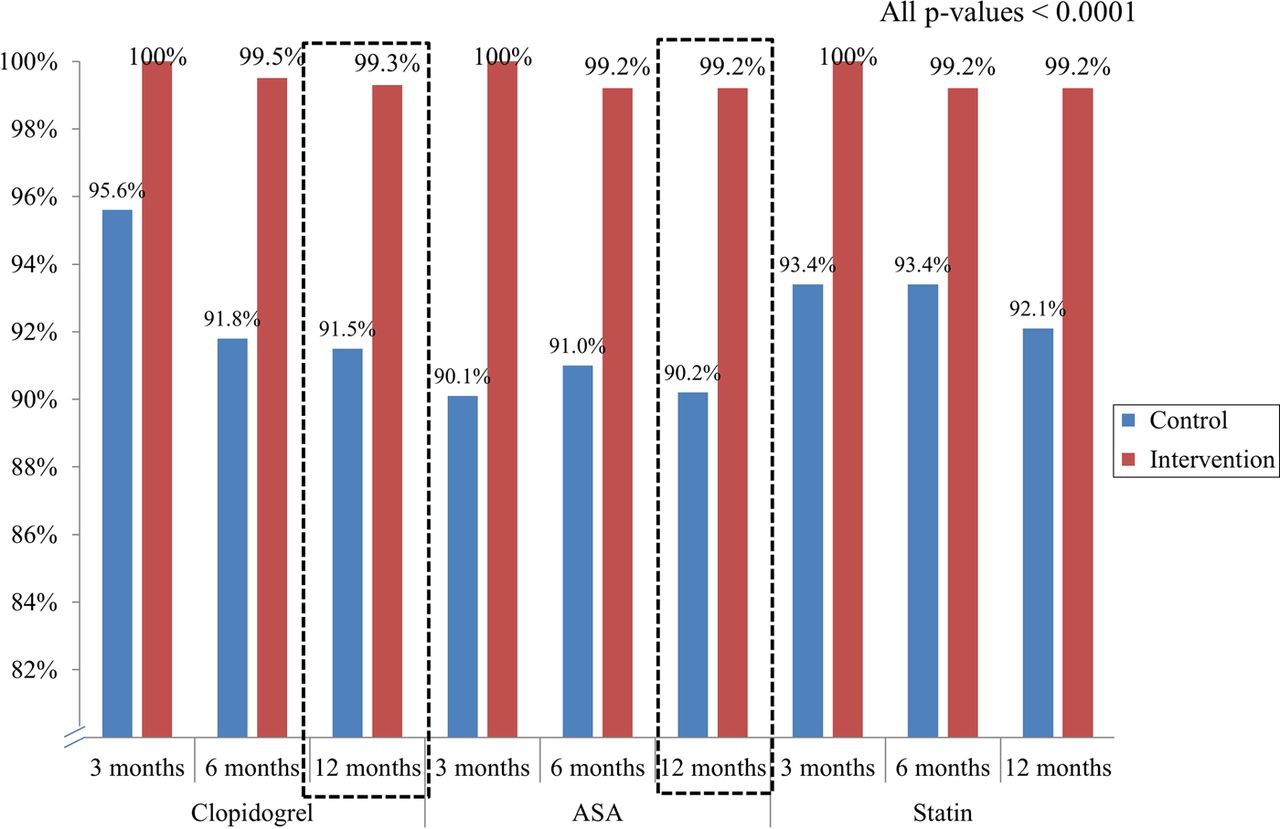
Results Most patients (73%) underwent DES implantation in the context of an acute coronary syndrome. All patients had drug insurance cover, either from the public plan (59%) or through private plans (41%). Complete pharmacy follow-up data were available for 96% of the cohort. At 12 months, median scores (25th–75th centile) for adherence to aspirin and clopidogrel were 99.2% (97.5–100%) and 99.3% (97.5–100%), respectively, in the intervention group compared with 90.2% (84.2–95.4%) and 91.5% (85.1–96.0%), respectively, in the control group (p<0.0001 for aspirin and clopidogrel). Patients in the intervention group were significantly more persistent in the aspirin and clopidogrel treatment than those in the control group. For clopidogrel, 87.2% of patients in the intervention group were still persistent at 12 months compared with only 43.1% in the control group (p<0.0001).
Conclusions A simple approach of four telephone calls to patients after DES implantation significantly improved 1-year drug adherence to near-perfect scores. Persistence of DAT was also significantly improved by the intervention.
Statistics from Altmetric.com
Introduction
Premature discontinuation of dual antiplatelet therapy (DAT) is common and the strongest risk factor for stent thrombosis and mortality in patients who receive a drug-eluting stent (DES).1 ,2 Delaying initiation, or even temporary discontinuation, of DAT after discharge after a percutaneous coronary intervention (PCI) also increases the risk of adverse cardiac events.3 ,4 Even a temporary discontinuation of DAT in the year after DES implantation can have harmful consequences.5 Thus continuous and uninterrupted DAT for at least 1 year has been strongly recommended.6 ,7
However, this approach relies solely on the patient's adherence, transferring all the responsibility to the patient, and may overlook several reasons why the patient might terminate the treatment or delay its onset. Indeed, with the increased incentive for early discharge after PCI, many patients are released on the day of the intervention8–10 or even the second day after primary PCI,11 reducing the time spent in hospital. Therefore, patients are less likely to receive adequate education or understand the serious nature of their disease, which may in turn increase the risk of drug non-adherence.12 To our knowledge, although there are studies that have shown the feasibility of remote home support programmes in other conditions,13 no study has to date tested interventions aimed at improving patient follow-up after discharge after DES implantation, to ensure optimal drug adherence and persistence. While adherence pertains to the qualitative and quantitative concept of how well the patient follows a physician's prescription over a certain period of time, persistence refers to the patient still taking the drug or not, as a binary variable, at a given time.14–16
We therefore designed the EArly discharge after transradial Stenting of coronary arterY-IMProving Adherence to Clopidogrel Trial (EASY-IMPACT) to test the hypothesis that a simple case management approach involving close follow-up by telephone would help identify barriers to optimal antiplatelet therapy and result in better aspirin and clopidogrel adherence after DES implantation, compared with the usual approach without telephone follow-up.
Methods
Trial design
The EASY-IMPACT Study (ClinicalTrials.gov Identifier NCT01134679) was a single-centre, open-label randomised controlled trial that used a 1:1 allocation ratio. This article follows the recommendations of the CONSORT (CONsolidated Standards of Reporting Trials) statement.17
Study population
Patients were eligible for the study if they underwent DES implantation during the day of randomisation, between June 2009 and June 2010, and if they were prescribed aspirin and clopidogrel (75 mg daily). Patients were deemed not eligible if they were purchasing their medication in several different pharmacies, which would preclude adequate monitoring of drug adherence. Data management was performed at the Institut universitaire de cardiologie et de pneumologie de Québec (IUCPQ, Quebec Heart and Lung Institute, Laval University) Research Center.
Ethical aspects
The study was approved by the institution research and ethics committee, and all patients provided written informed consent. Patients provided consent for the study team to contact their pharmacists to obtain detailed pharmacy data on the dates of prescription filling and the number of pills received for aspirin, clopidogrel and also the statin agent used.
Randomisation
A randomisation sequence was generated by the principal investigator, using permuted blocks of 4, and 300 sealed envelopes with the patient number were prepared before recruitment. Research assistants opened envelopes in sequence, after obtaining signed informed consent.
Interventions
Patients were randomised on a 1:1 ratio to one of the two study groups. The intervention group received physician and hospital pharmacist counselling on the importance of DAT after DES, but also received phone calls within 7 days and at 1 month, 6 months and 9 months after PCI. During these 5–10 min calls, adherence to DAT was assessed, and the importance of optimal drug compliance reinforced; patients were told that a clot could form in their stent if DAT was delayed, skipped or stopped, and this could cause major heart problems including myocardial infarction (MI) and potentially death. Factors associated with premature discontinuation of DAT were discussed, including bleeding, non-cardiac procedures and financial problems. Research assistants or nurses conducted the phone calls. They were trained to provide efficient counselling on the importance of DAT and the risk of any interruption and support to ensure optimal drug adherence. Patients in the control group received counselling before discharge as per usual clinical practice in our institution, but did not receive phone calls.
Outcomes
The primary outcome measure was the number of days with available aspirin and clopidogrel (from pharmacy records), at 1 year, expressed as a continuous refill-adherence score (number of pills divided by 365 days).14 ,15 Secondary outcome measures included aspirin and clopidogrel refill-adherence scores at 3 and 6 months and statin refill-adherence scores at 3, 6 and 12 months. From a persistence perspective (being on a drug or not at a given time point),16 the proportion of patients who delayed filling of the clopidogrel prescription for more than 1 day after hospital discharge, persistence of aspirin and clopidogrel treatment up to 12 months (using a refill ‘gap’ of 14 days; when reached, a patient was considered non-persistent), and binary persistence at 6 and 12 months (being on the medication or not at the time of assessment, allowing an adherence score of >0.50 over the 7 days before assessment, irrespective of earlier filling history) were all assessed. Other secondary end points included persistence of aspirin and clopidogrel treatment as self-reported by patients at 6 months and 1 year, and clinical outcomes, including mortality, stent thrombosis, MI, major bleeding episodes and repeat revascularisation procedures.
Outcome assessment
Pharmacy data were gathered through telephone contact with individual pharmacists filling prescriptions of study patients, by requesting that refill data on aspirin or acetylsalicylic acid (ASA), clopidogrel and statin therapy be sent on a periodic basis to the research coordination centre. All medication data were entered in a dedicated dataset, and a full year calendar was generated for each patient. For each day with medication, a 1 was assigned, otherwise a 0 was allocated. The adherence score (proportion of days covered) was calculated by our research team by summing the number of pills served over the studied period, in the numerator, and dividing by the number of days in the period (365 for the 1-year primary end point). As drug prescription filling will usually be delayed by the same number of days of medication missed,14 no assumption can be made whether those days are consecutive within a given period or distributed throughout the period. In the case of refill before the end of a 30-day prescription, the number of pills for the overlapping period was accounted for. We also conservatively assigned two pills for in-hospital days during follow-up, assuming that aspirin, clopidogrel and statin were provided by the hospital, leaving additional medication available upon discharge; even in the case of temporary discontinuation of medication during in-hospital periods, several non-taken pills would be available for subsequent resumption of the medication. Finally, when data were missing, repeat phone calls were made to the pharmacy to ensure that the data would be transferred to our research centre.
Self-reported persistence of DAT was assessed at 6 and 12 months through phone calls, in a non-influential matter by a different set of assistants. In order to not bias answers, patients were first asked ‘dummy questions’, such as ‘are you taking medication for arthritis?’, then ‘for hypertension?’. They were then asked if they were taking blood-thinning medication and, if so, were they taking warfarin, aspirin or clopidogrel.
Clinical end points were assessed through telephone contact at 6 and 12 months. During these short phone calls, patients were asked if they had been rehospitalised. The summary discharge forms of other hospitals were then requested to confirm the cause of admission. MI was defined as any rise in biomarker above the 99th centile, in a plausible clinical context.18 The definition of stent thrombosis was that used by the Academic Research Consortium.19 Major bleeding episodes were considered if they required a hospital stay or a physician visit. All IUCPQ charts were also reviewed. Finally, the hospital catheterisation laboratory dataset was assessed for repeat angiography or PCI.
Calculation of sample size
We powered the trial to detect an early effect of the intervention, as early as after 3 months. Considering a clopidogrel adherence score of 86±28% at this time point in unselected patients who underwent PCI (unpublished data from the Régie de l'assurance maladie du Québec dataset),3 a sample size of 115 patients per group was required to demonstrate, with a two-sided α of 0.05 and a power of 80%, that the intervention could improve the score by 10 points (to 96%, with the same SD). Any difference at 3 months was assumed to either persist or accrue between groups over time. Given that the number of pharmacies used to provide medication refill data was large, we decided to raise the sample size to 150 patients per group to mitigate an unlikely 20% missing data rate. Finally, any difference at 3 months was assumed to either persist or more likely accrue between groups over time, as others have shown decreased persistence or adherence over time after the PCI.5 No interim analysis was planned or performed. No stopping rules were applied to the study. As a result, a data safety and monitoring board was judged not to be required.
Blinding
Blinding was impractical in this study. However, to ensure that secondary clinical outcomes would be collected as blindly as possible, two investigators reviewed all study patient charts and angiographies without knowing the patient study group. All end points were adjudicated by one interventional cardiologist and one non-interventional cardiologist, blinded to the randomised group. Most importantly, care providers and pharmacists were not informed that their patients would or would not receive phone calls.
Statistical analysis
Baseline descriptive statistics to characterise the study population include frequency distributions for categorical variables and mean±SD or median (25th–75th centile) for continuous variables, and as appropriate according to the distribution. All primary and secondary end point analyses were performed using the intent-to-treat principle.20 Missing pharmacy data were first calculated, and only available data were analysed.
For all primary and secondary drug-adherence end points, we first compared adherence scores between groups and over time, using two-way analysis of variance. Thereafter, scores between groups at each of the three time points were compared with the Wilcoxon–Mann–Whitney two-sided test. Median aspirin and clopidogrel adherence scores at 1 year were considered co-primary end points and were analysed at the 0.025 significance level. Persistence of aspirin and clopidogrel treatment up to 12 months was compared using survival statistical methods with the log-rank test. The proportion of patients who delayed filling of their clopidogrel prescription for more than 1 day, binary persistence (pharmacy data or self-reported), and clinical end points were compared with the Fisher exact test. We assessed the agreement between self-reported persistence and binary persistence using κ statistics. Finally, to assess the robustness of our findings, we tested the impact of the intervention using linear regression controlling for baseline imbalanced findings. These secondary end points were analysed at the 0.05 significance level, without adjustment for multiple comparisons. All reported p values are two-sided. Statistical analyses were performed using SAS software, V.9.2.
Results
Recruitment and participant flow
A total of 300 patients were randomised between June 2009 and June 2010. The last patient recruited reached the 1-year follow-up time point in June 2011.
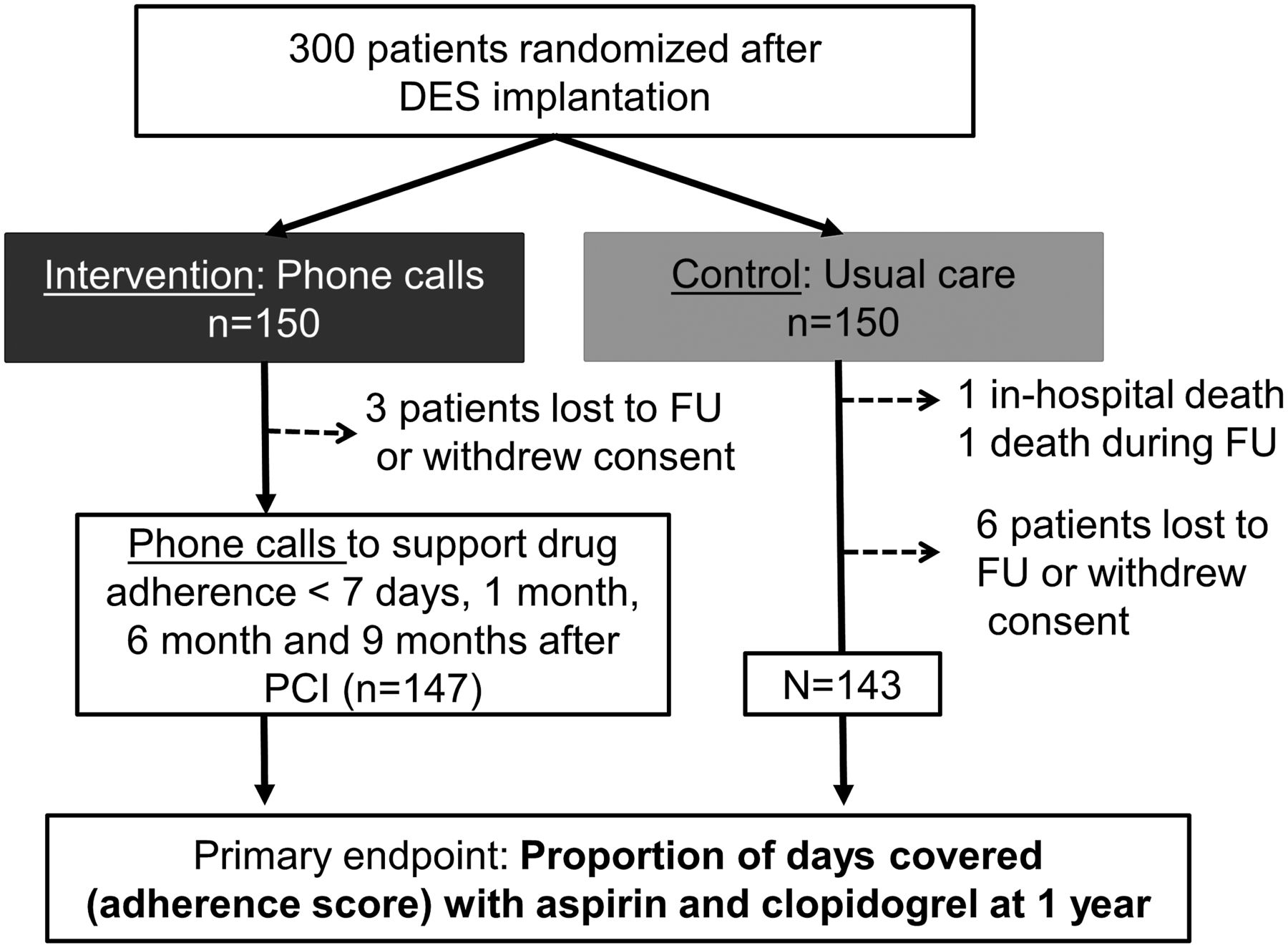
Of the 300 patients randomised, two from the control group died, one in hospital after the index PCI (an 87-year-old woman who presented with non-ST-elevation MI and underwent left main and left anterior descending artery stenting complicated by shock later during the hospital stay), and one 3 months after PCI, due to congestive heart failure without evidence of MI. Of the remaining 298 patients, nine withdrew consent or were lost to follow-up; we did not collect pharmacy data on these patients. Otherwise, of the residual 289 patients, 1-year pharmacy data were available for all of them for clopidogrel, for 286 (99.0%) for aspirin, and for 287 (99.3%) for the statin (figure 1). Therefore complete pharmacy follow-up data were available for 96% of the 300 randomised patients.

Flowchart of the study population. DES, drug-eluting stent; FU, follow-up. This figure is only reproduced in colour in the online version.
Baseline clinical, socioeconomic, angiographic and procedural characteristics
Mean age was 64±10 years, and 73% were male. Most patients (73%) underwent DES implantation for acute coronary syndrome. The groups were well balanced, except for the higher proportion of patients who had a prior coronary artery bypass graft (CABG) or chronic renal failure in the control group compared with the intervention group (p<0.05) (table 1). All patients had drug insurance cover, either from public provincial plans (59%) or through private plans (41%). The majority of patients were retired, and a large proportion was using pill organisers. Education level was relatively low. These baseline characteristics were well balanced (table 2).
Baseline clinical characteristics
Baseline social characteristics
The most commonly used DES was the sirolimus-eluting stent (64%). Patients received on average 1.9±1.1 stents. Angiographic and procedural characteristics were also well balanced overall. However, more saphenous vein graft disease and more vessels were treated in patients in the control group than in the intervention group (p<0.05) (table 3).
Procedural characteristics
Telephone follow-up data for the intervention group
Three patients were lost to follow-up or withdrew consent for follow-up. The other 147 patients from this group received four phone calls: one within 7 days of the procedure, one at 1 month, one at 6 months and one at 9 months of follow-up. During the first call, 96% of patients knew they had received a DES, but only 92% reported going to the pharmacy to get the medication. If they reported that they had not, they were urged to do so as early as possible. At 1 month, <1% reported having missed or forgotten to take their medication, a proportion that remained stable at 6 and 9 months. Finally, 19/139 (14%) reported minor bleeding problems during the first call, such as bruises and nose and gingival bleeding. This proportion was 17% at 1 month, 13% at 6 months and 8% at 9 months.
Drug adherence and persistence by pharmacy data
Three patients required calculation adjustment that did not influence the results. One patient in the intervention group underwent CABG 6 months after randomisation; clopidogrel was appropriately stopped before surgery, and clopidogrel adherence was therefore calculated up to the time of its cessation. One patient in the intervention group presented with a rash attributed to clopidogrel, and was switched to ticlopidine 2 months after randomisation. Drug adherence to clopidogrel was calculated up to the switch for that patient. Finally, one patient, again from the intervention group, presented with a pulmonary embolism and was placed on warfarin 3 months after randomisation. Clopidogrel was stopped for 4 months, and resumed afterwards. Despite discussion with the treating physician, it was decided not to administer clopidogrel with warfarin. We conservatively calculated the adherence score on the full year, attributing a 0 for all the days the patient was not receiving clopidogrel, but was receiving warfarin.
For the primary end point, at 12 months, median (25th–75th centile) refill-adherence scores for aspirin and clopidogrel were 99.2% (97.5–100%) and 99.3% (97.5–100%) in the intervention group compared with 90.2% (84.2–95.4%) and 91.5% (85.1–96.0%) in the control group (Wilcoxon–Mann–Whitney p<0.0001, for aspirin and clopidogrel). The improvement in adherence was seen as early as 1 month after the PCI, and persisted for up to 1 year. Adherence to the statin followed the same pattern (figure 2, with dashed boxes showing the primary end point). Using two-way analysis of variance, we did not find any significant impact of time on adherence score over the study period, but only a significant impact of the treatment group. After adjustment for baseline differences (previous CABG, chronic renal failure, saphenous vein graft disease, and number of vessels treated), the effect of the intervention on ASA or clopidogrel adherence (as a percentage) remained largely unchanged (online supplementary table 1).
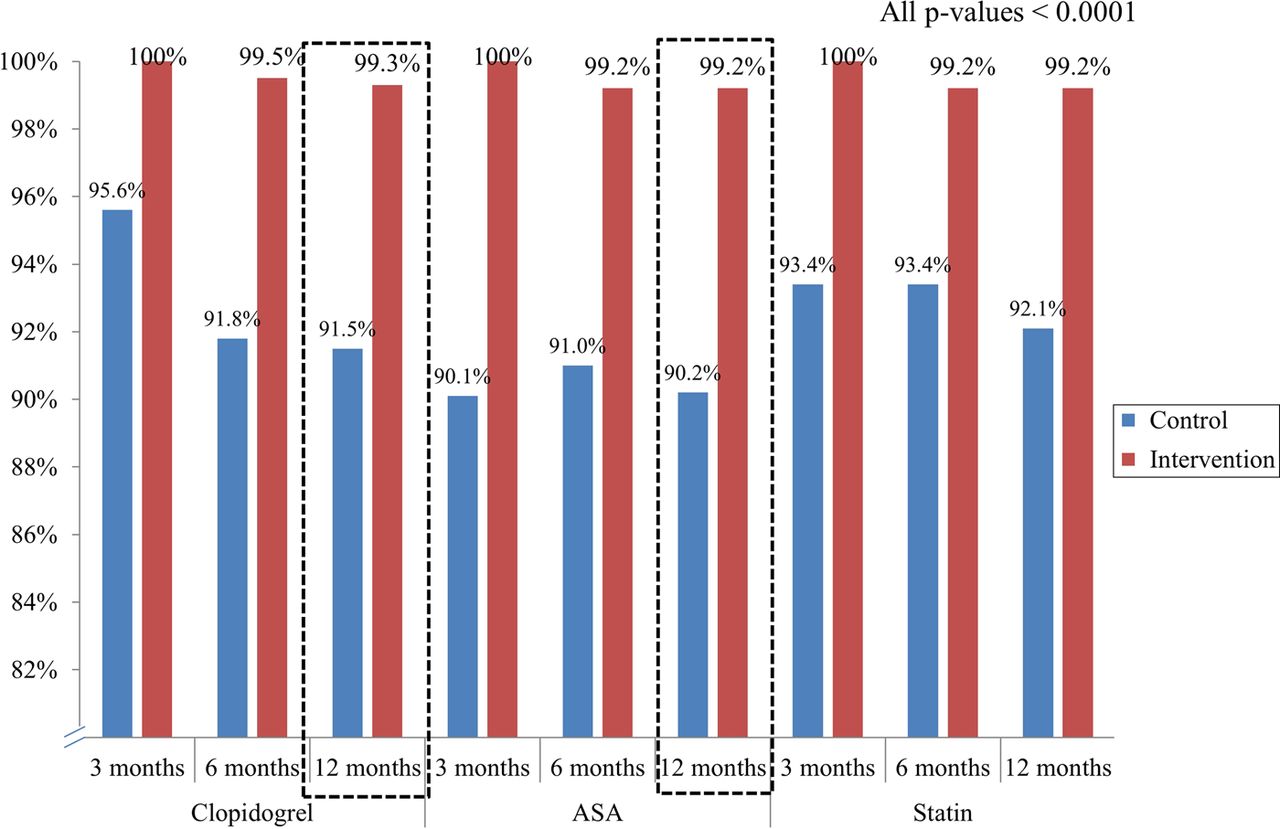
Median refill-adherence scores at 3, 6 and 12 months. Dashed boxes highlight the primary end point. This figure is only reproduced in colour in the online version.
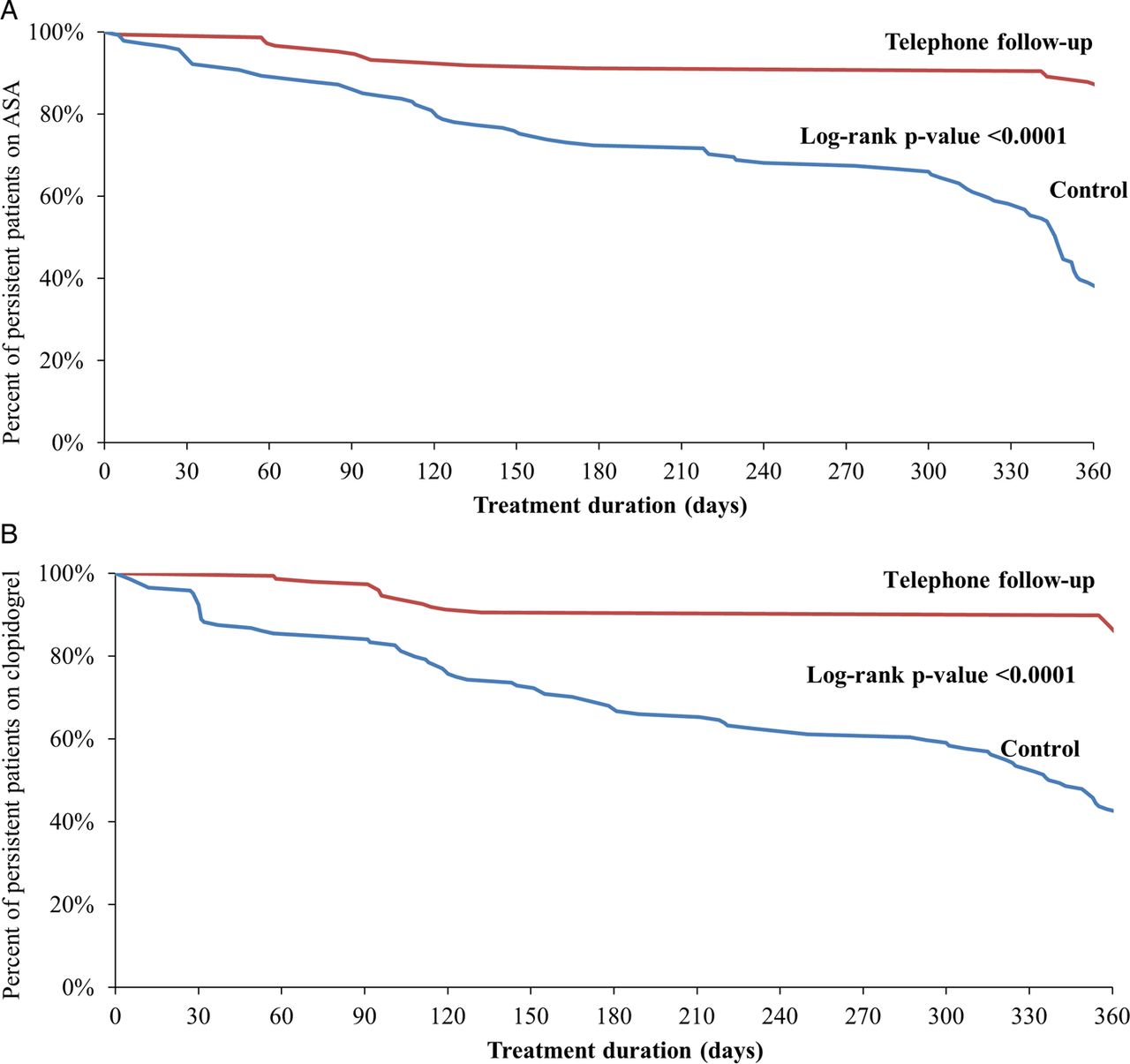
Delayed filling of the clopidogrel prescription (later than the day after discharge) was encountered in 21.6% of the intervention group vs 27.1% of the control group (p=0.28). If persistence, defined as no gaps longer than 14 days, is considered, significant improvements resulted from the intervention for both ASA and clopidogrel (figure 3A,B). Of note, for clopidogrel, 87.2% of patients in the intervention group were still persistent at 12 months compared with 43.1% in the control group (p<0.0001). When binary persistence was assessed, 97.3% of intervention vs 93.1% of control group patients were still taking ASA at 6 months (p=0.11), but 91.2% vs 64.6% at 12 months (p<0.0001). For clopidogrel, no difference in binary persistence was observed at 6 months (94.6% vs 97.2%; p=0.38), but the proportions fell to 91.9% and 80.6%, respectively, at 12 months (p=0.0049).
{kind=link}
{kind=link}
{kind=link}
Persistence of acetylsalicylic acid (ASA) (A) and clopidogrel (B) treatment. This figure is only reproduced in colour in the online version.
Self-reported drug persistence
At 6 months, 96% of patients in the intervention group reported taking aspirin compared with 94% in the control group (p=0.59). The vast majority also reported taking clopidogrel at this 6-month time point (95% in the intervention group vs 98% in the control group; p=0.34). These proportions remained stable at 1 year: 98% in the intervention group vs 99% in the control group reported taking ASA (p=1.0), whereas 97% in the intervention group vs 100% in the control group (p=0.06) reported taking clopidogrel. We assessed self-reported persistence versus binary persistence at 12 months. We found weak agreement. At 12 months, 98.6% of patients reported taking clopidogrel, whereas only 86.4% were still taking the drug according to pharmacy data (binary persistence) (κ=0.14; 95% CI −0.01 to 0.28). Almost all patients (99%) reported taking ASA, whereas it could only be confirmed in 78% (κ=0.01; 95% CI −0.04 to 0.07).
Clinical outcomes
During the 1-year follow-up, one patient from the control group died from heart failure. The patient did not undergo catheterisation. No patient presented with stent thrombosis, and no patient presented with ST-elevation MI or sudden death. One patient underwent CABG. No patient presented with major bleeding complications requiring interruption of the therapy. A few patients (6.8% from the intervention group vs 3.5% from the control group, p=0.29) presented with unstable angina requiring hospitalisation during the 1-year follow-up, and 2.0% in the intervention group vs 7.0% in the control group (p=0.05) presented with recurrent stable angina. Three patients presented with non-ST elevation MI (one in the intervention group, two in the control group, p=0.61); they all underwent repeat coronary angiography and none had stent thrombosis. Eight patients underwent repeat target lesion PCI (five (3.4%) in the intervention group, three (2.1%) in the control group (p=0.72)), and 11 underwent non-target repeat PCI (six (4.1%) in the intervention group, five (3.5%) in the control group (p=1.0)).
Discussion
Our objective was to assess if closer follow-up after DES implantation would improve adherence to DAT. In this single-centre trial, a simple strategy of telephone follow-up with patients resulted in a significant improvement in adherence to aspirin and clopidogrel after DES implantation. Although adherence scores in the control group were higher than 80%—a threshold often considered satisfactory for other drugs16—the intervention permitted near-perfect scores to be reached. The intervention also had a favourable effect on adherence to statin therapy. Persistence was also greatly improved with the intervention. Finally, most patients in both groups reported taking DAT appropriately, even at 1 year; self-reported compliance clearly and grossly overestimated the true medication refill-adherence status in our study, with very low agreement with actual pharmacy data. This finding strongly questions the value of using patients’ reports on drug compliance.
Premature discontinuation of DAT is a very strong risk factor for stent thrombosis and mortality.1 The value of extending DAT for at least 1 year is clearly documented.21 ,22 Unfortunately, one out of seven patients in the Prospective Registry Evaluating Myocardial Infarction: Events and Recovery Study2 who underwent DES implantation reported having stopped their DAT at 30 days. These patients were found to be at much higher risk of mortality, reaching 5% at 12 months.2 Even delaying initiation of DAT after discharge increases the risk of mortality.3 ,4 Up to one in every six patients delays filling their clopidogrel prescription after hospital discharge after PCI.5 In Quebec, using pharmacy data, we found that one in every five patients after stent implantation either delayed or never received DAT, largely because of restricted access before 2008.3 Finally, even temporary discontinuation of DAT can be dramatic. Another study found that up to 15% of patients interrupted their DAT for more than 5 consecutive days, for reasons usually not related to major bleeding.5
Such dependence on DAT after DES implantation poses potential problems. Despite new and more potent antiplatelet agents that may confer incremental clinical benefits,23 ,24 drugs can only work in patients who take them. Drug adherence is a multifaceted process with several potential barriers.12 More specific to DAT, impaired access, treatment of asymptomatic disease (many patients have no more symptoms after PCI), bleeding events, and inadequate follow-up discharge planning are among the potential barriers to optimal compliance.12
To the best of our knowledge, this is the first study to test the hypothesis of improved adherence to DAT with a close follow-up telephone contact. We used a simple human approach to support patients; such an approach has also proven to be beneficial for other conditions, such as hypertension.15 At the first telephone call, 8% of patients had not yet visited the pharmacy. Between 10 and 15% of patients reported potential minor bleeding problems; they were encouraged not to stop their medication. The importance of repeated contact, even without identifying serious problems, may also explain the positive results of the present study.
Near-perfect drug adherence and persistence is what physicians really expect with DAT after DES implantation. However, median adherence scores were around 90% at 1 year in the control group. This represents 10% of the year without DAT, or roughly 36 days. Although we acknowledge that this period is spread over the year, such non-adherence is expected to result in a lower antiplatelet effect. When we looked at persistence of clopidogrel treatment, only 43% of the patients in the control group had not encountered a 2-week period without medication over the 1-year follow-up. Missing DAT for more than 5 days increases the risk of mortality.5 Therefore, our intervention, if performed on a larger sample, may show improved survival.
Study limitations
We used a surrogate marker, the refill-adherence score, as the primary end point. Use of a clinical end point such as stent thrombosis would have required a much larger sample size. Indeed, no patient presented with stent thrombosis, highlighting this fact. The study had therefore limited power for clinical end points. Also, it is not possible to know with refill-adherence if the patients skipped doses evenly during the period, or if the doses were all consecutive. While forgetting one dose might be benign, longer treatment gaps are clearly dangerous.5 Although our research personnel administered the 6- and 12-month drug-persistence questions in a non-influential fashion, we cannot exclude the possibility that patients minimised any compliance issues in order to ‘satisfy’ the research team, or for other reasons. The study was performed in a publicly managed healthcare system, with theoretically minimised access problems. As a result, all patients were insured through private or public drug plans. However, as most patients in the western world receive DAT through insurance plans, we believe our results can be generalised. Only clopidogrel was used during that period; however, we expect that patients could also benefit from such an intervention irrespective of the agent used in conjunction with aspirin. Ticagrelor has a shorter half-life24; use of ticagrelor without close follow-up may result in periods with an earlier decrease in the antiplatelet effect, which may strongly impair the effectiveness of this drug. Finally, we had no data on the frequency of outpatient physician follow-up (general practitioner or cardiologist) in both groups; however, given that treating physicians were not informed about the patient's study group, any imbalance is unlikely.
Conclusions
A simple approach that consisted of four phone calls over the year after DES implantation resulted in a significant improvement in adherence to aspirin and clopidogrel, but also to the statin, to near-perfect scores. Persistence was also greatly improved. Such an approach may provide additional clinical benefits beyond the use of more potent antiplatelet agents. Whether improved drug adherence through such a simple programme can translate into better clinical outcomes requires further investigation.
Acknowledgments
The authors thank Jessie Micholuk, Sarah Cohen-Fournier, Marie Martin de Mereuil, Brigitte Fournier and Guy Rossignol for providing assistance with the performance of the study.
References
Footnotes
-
Contributors Study concept, design and responsibility for the overall content as guarantor: SR. Coronary angiography review: SR and RB. Analysis and interpretation of data: SR and MD. Drafting of the manuscript: SR. Critical revision of the manuscript for important intellectual content: JR-C, MD, J-PD, EL, GB, OG, C-MN, BN, GP, LR, IT, RDL and OFB. Study supervision: SR. There was no data sharing; all data related to this project is presented in this article.
-
Funding The study was supported by an unrestricted research grant from BMS-Sanofi Canada. SR, EL and OFB are junior physician-scientists of the Fonds de la recherche du Québec-Santé (FRQS) (Quebec Research Fund-Health).
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval The study protocol was performed in accordance with the institutional ethics committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.