Article Text

Abstract
Objective To investigate the prevalence and significance of increased left ventricular (LV) trabeculation in highly trained athletes.
Design Cross sectional echocardiographic study.
Setting Sports cardiology institutions in the UK and France.
Subjects 1146 athletes aged 14–35 years (63.3% male), participating in 27 sporting disciplines, and 415 healthy controls of similar age. The results of athletes fulfilling conventional criteria for LV non-compaction (LVNC) were compared with 75 patients with LVNC.
Main outcome measure Number of athletes with increased LV trabeculation and the number fulfilling criteria for LVNC.
Results Athletes displayed a higher prevalence of increased LV trabeculation compared with controls (18.3% vs 7.0%; p≤0.0001) and 8.1% athletes fulfilled conventional criteria for LVNC. Increased LV trabeculation were more common in athletes of African/Afro-Caribbean origin. A small proportion of athletes (n=10; 0.9%) revealed reduced systolic function and marked repolarisation changes in association with echocardiographic criteria for LVNC raising the possibility of an underlying cardiomyopathy. Follow-up during the ensuing 48.6±14.6 months did not reveal adverse events.
Conclusions A high proportion of young athletes exhibit conventional criteria for LVNC highlighting the non-specific nature of current diagnostic criteria if applied to elite athletic populations. Further assessment of such athletes should be confined to the small minority that demonstrate low indices of systolic function and marked repolarisation changes.
Statistics from Altmetric.com
Introduction
Left ventricular non-compaction (LVNC) cardiomyopathy is characterised by increased left ventricular (LV) trabeculation and intertrabecular recesses communicating within the LV cavity. Clinical manifestations include progressive LV dilatation, systolic impairment, predilection to fatal arrhythmias and thromboembolic events.1 Studies in heart failure patients demonstrate a high prevalence of LV trabeculation often fulfilling the conventional LVNC diagnostic criteria, irrespective of the criterion used.2 Considering the low reported prevalence of LVNC, it is unclear whether the myocardial morphology is representative of primary LVNC or merely an epiphenomenon associated with increased cardiac preload.
The large cardiac preload associated with regular intensive exercise results in physiological increases in LV wall thickness and cavity size.3 ,4 Isolated case findings have also revealed increased LV myocardial trabeculation in some athletes but the significance of the anomaly is unclear. The distinction between cardiac remodelling secondary to athletic training and LVNC is important when one considers that primary cardiomyopathies are the most commonly implicated cause of exercise related sudden cardiac death (SCD) in young athletes.5
The aim of this study was to identify the prevalence and significance of increased LV trabeculation in highly trained young athletes.
Methods
Setting
The study was part of a collaborative programme between sports cardiology institutions in the UK and France. The death of some high profile athletes has led several sporting organisations in the UK to fund cardiac screening for recruits at regional and national levels. In many instances, Cardiac Risk in the Young, a charitable organisation, has subsidised such cardiovascular evaluations and the senior author (SS) has been responsible for the management and supervision of these evaluations since 1996. In France, athletes participating at the national level are required to undergo cardiovascular screening with an annual ECG and at least one echocardiogram during their career. Cardiovascular evaluations in France are predominantly supervised by the author FC at the University of Rennes.
Athletes
Between 2003 and 2011, 1146 athletes aged 14–35 years competing at regional or national levels underwent cardiac evaluation. The evaluation consisted of a self-reported health questionnaire enquiring about cardiac symptoms, drug history and a family history of premature cardiovascular disease or SCD; physical examination; 12-lead ECG and two-dimensional echocardiography. Ethnicity was determined through the self-reported questionnaire.
Controls
The control population consisted of 415 sedentary volunteers (table 1). Controls were recruited from population screening programmes offered by Cardiac Risk in the Young, that are aimed at identifying potentially sinister cardiac disorders in young and apparently healthy individuals aged 14–35 years. Evaluations were performed at secondary schools and community centres throughout the UK and included a self-reported health questionnaire, cardiovascular examination, 12-lead ECG and echocardiogram.
Comparison of demographics between athletes and controls*
Selection criteria included age 14–35 years, sedentary lifestyle (defined as physical activity ≤2 h per week), absence of cardiac symptoms or family history of cardiomyopathy, a structurally normal heart on echocardiography and free of regular medication.
LVNC patients
Between 2002 and 2010, 75 consecutive patients with LVNC were evaluated in two specialist cardiomyopathy clinics in South London (University Hospital Lewisham and St. George's Hospital National Health Service Trust). Individuals were diagnosed with LVNC following either primary care referral for symptoms, detection of a cardiac murmur, an abnormal ECG or during a cardiovascular assessment of an individual in the context of a family history of cardiomyopathy or SCD. LVNC was diagnosed on 2-dimensional echocardiograms according to criteria by Chin,6 and Jenni.7
Twelve-lead electrocardiography
A standard 12-lead ECG was performed using a GE Marquette Hellige (Milwaukee, Wisconsin, USA) or Philips Pagewriter Trim III (Bothel, Washington, USA) with a paper speed of 25 mm/s and amplification of 0.1 mV/mm as previously described.8 Heart rate and QRS axis were calculated. Intervals and voltages were measured in each lead with callipers. The QT was corrected for heart rate using the Bazett formula (QTc).9 Sokolow-Lyon voltage criterion,10 was used to define left ventricular hypertrophy (LVH). T-wave inversion ≥2 contiguous leads excluding leads V1 and III was considered significant.
Echocardiography
Two-dimensional echocardiography was performed using the Philips Sonos-7500, Philips-iE33 or Philips-CPX50 (Bothel, Washington, USA) and Accuson Computed Sono-graph-128XP/1°c (San Jose, California, USA). Standard cardiac views were obtained and analysed according to protocols specified by the European Association of Echocardiography.11 Left ventricular wall thickness (LVWT) was measured from 2-D parasternal short axis, at the level of the mitral valve and papillary muscles in end-diastole, the greatest measurement being defined as the maximal LVWT. Left atrial diameter and LV diameter were measured from the parasternal long-axis view using the two-dimensional images. LV systolic function was assessed using the volumetric biplane Simpson's method.11 Measures of diastolic function included pulsed wave Doppler across the mitral valve,12 and tissue Doppler velocities of the septal and lateral mitral valve annulus.13 Echocardiographic studies were saved to compact discs as numeric files to generate anonymity. Assessment for LV trabeculation was performed in end diastole. The ratios of compacted to non-compacted myocardium were performed in end diastole6 and end systole.7 Cardiac measurements were repeated by an experienced cardiac physiologist (MR) blinded to the identity of the athlete.
Definition of increased left ventricular trabeculation
Myocardial trabeculations were defined as localised protrusions of the endocardial surface ≥3 mm in diameter,14 associated with intertrabecular recesses on 2-D echocardiography. The definition of increased LV trabeculation was derived from echocardiographic measurements of our control population and was represented by the mean number of trabeculations plus 2 SD. The mean number of trabeculations in the controls was 0.76±1.1; therefore we used a rounded figure of 3 trabeculations to define increased LV trabeculation. Colour flow Doppler using a Nyquist limit of 20–30 cm/s was applied when numerous small cavities within the endocardial surface were identified in a two-layered structure. The echocardiographic criteria by Chin,6 and/or Jenni,7 were used to define LVNC.
Ethical approval/consent
The National Research Ethics Service, Essex-2 Research Ethics Committee, granted ethical approval in the UK. In France, the French Ministry of Health and Youth approved the study. Written consent was obtained from individuals aged ≥16 years and from a parent/guardian for those aged <16 years.
Statistical analysis
Statistical analyses were performed using STATA V.11.1 (StataCorps, Texas, USA). Variables were tested for normality using the Kolmorgorov-Smirnov test. Values are expressed as either mean±SD or percentages, as appropriate. Differences between group means were compared using independent t-tests or Mann-Whitney U tests (for normally and non-normally distributed variables respectively). χ2 test or Fisher's exact test was used as appropriate to test group differences of proportions. Pearson's or Spearman's correlation coefficients were used as appropriate to measure the correlation of two continuous variables.
Logistic regression was used to determine which of the following variables were associated with increased LV trabeculation: ethnicity; age; body surface area (BSA) and T-wave inversion. A multivariate model was fitted which included variables identified as statistically significant in the univariate analyses.
Statistical significance was defined as a two-tailed p value of <0.05 throughout and p values were adjusted for multiple testing, where appropriate, using the Bonferroni correction.
Results
Athletes
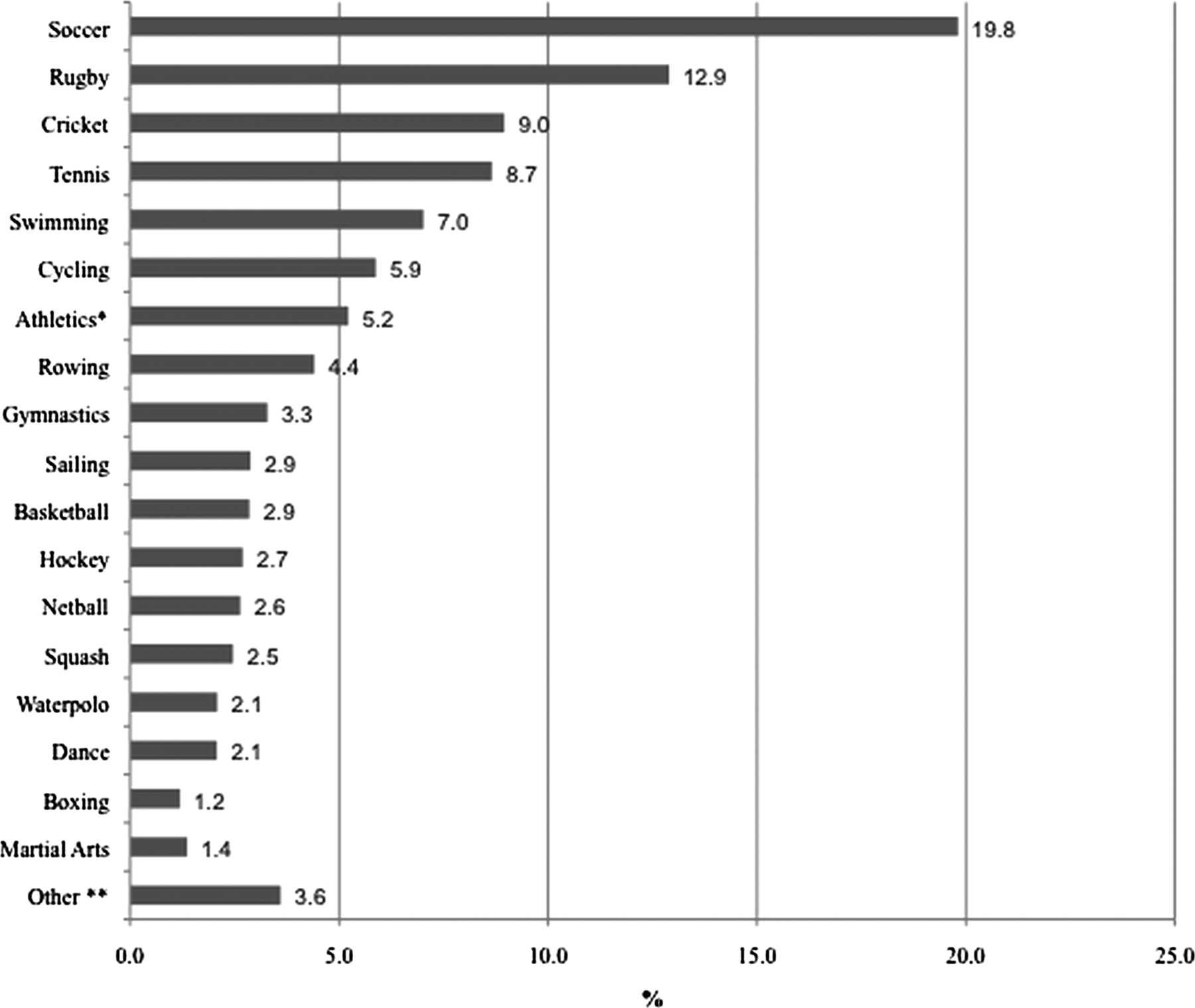
The athletes were aged 20.9±6.0 years. The majority were men and of Caucasian ethnicity, (table 1). Athletes participated in 27 different disciplines (figure 1) but the vast majority consisted of soccer, rugby, cricket, tennis and swimming which collectively comprised 57.3% of the athletic cohort. Athletes trained for an average period of 17.7 h per week. All athletes were asymptomatic, none reported symptoms of cardiac disease or a family history of cardiomyopathy or premature SCD. None of the athletes revealed a blood pressure of ≥140 mm Hg systolic or ≥90 mm Hg diastolic.

Sporting disciplines expressed as percentage of the total athletic cohort. Athletics* indicated Track and field events; Other** constitutes <3% of the total cohort, Badminton, n=1 Biathlon, n=15; Diving, n=5; Fencing, n=5; Handball, n=6; Speed skating, n=3; Volleyball, n=6.
Controls
The controls were older than the athletes but had a similar BSA. The majority was men, Caucasian and none exhibited symptoms of cardiovascular disease (table 1).
Patients with left ventricular non-compaction
Detailed demographic and clinical characteristics of patients with LVNC are presented in table 2.
Demographics, clinical, electrocardiographic and echocardiographic characteristics of patients with left ventricular non-compaction (n=75)*
Athletes exhibiting increased left ventricular trabeculation
Athletes revealed a higher prevalence of increased LV trabeculation compared with controls (18.3% vs 7.0%; p<0.0001). The prevalence was similar in men and women (20.7% vs 18.1%; p=0.279) but was more common in African/Afro-Caribbean (black) compared with Caucasian (white) athletes (28.8% vs 16.3%; p=0.002). Athletes with increased LV trabeculation most commonly (87%) participated in high dynamic sports.
Athletes fulfilling criteria for left ventricular Non compaction
Of the total athlete cohort, 9.5% fulfilled the Jenni criteria, 10.1% fulfilled the Chin criteria and 8.1% fulfilled both criteria for LVNC (figures 2 and 3). In contrast, none of the controls showed features of LVNC. The mean non-compacted, compacted layers and ratios in athletes fulfilling LVNC criteria and controls exhibiting increased LV trabeculation are presented in table 3. Athletes fulfilling both criteria did not show any significant ethnicity (11% of black vs 8.4% of Caucasian athletes; p=0.342) or sex predilection (7.6% of men vs 9% of women; p=0.434) and did not differ in age (20±6 vs 21±5 years old; p=0.692) or BSA (1.9±0.52 vs 2.0±0.3 m2; p=0.793) compared with athletes without LVNC criteria.

2-D echocardiographic examples of an athlete demonstrating measurements of compacted and non-compacted layers in end-diastole (A) and end-systole (B).

Flow chart demonstrating the prevalence of athletes fulfilling left ventricular non-compaction criteria, T-wave inversion and low ejection fraction (EF).
Athletes fulfilling LVNC criteria did not differ from those without LVNC criteria in terms of training related (Group 1),15 ECG changes with the exception of a higher prevalence of Sokolow-Lyon voltage criterion for LVH. In contrast, athletes fulfilling LVNC criteria had a higher prevalence of non-training related (Group 2),15 ECG changes (33% vs 14.6%; p<0.0001), including left and right axis deviation, voltage criterion for right ventricular hypertrophy and T-wave inversions. The higher prevalence of T-wave inversions in athletes fulfilling LVNC criteria compared with those without persisted across ethnicity (31.3% vs 3.7% in black athletes, p=0.001; 13.0% vs 5.3% in white athletes, p<0.019) and sex (16.3% vs 6.0% in men, p=0.0075; 13.2% vs 4.6% in women, p=0.041) (table 3).
There were no significant differences in LVWT, LV cavity size or indices of diastolic function between athletes fulfilling LVNC criteria compared with those without (table 4).
Comparison of electrocardiographic and echocardiographic parameters in athletes with and without LVNC*
Comparison of athletes fulfilling criteria for LVNC with patients with LVNC
Compared with two-thirds of patients with LVNC who exhibited symptoms of heart failure, athletes fulfilling echocardiographic criteria for LVNC were asymptomatic. Sokolow-Lyon voltage criterion for LVH was present in a significant proportion of patients with LVNC (58.3%) and athletes fulfilling LVNC criteria (32.2%), however unlike athletes, none of the patients with LVNC demonstrated large QRS complexes in isolation.
T-wave inversion was identified in 30.5% of patients with LVNC and 16.1% of athletes fulfilling LVNC criteria but there were important differences in the distribution and magnitude of T-wave inversion between the groups. Compared with athletes, patients with LVNC predominantly expressed T-wave inversion in the inferior (20.0% vs 5.4%; p=0.007) and lateral leads (28.0% vs 2.2%; p<0.001). In contrast, most T-wave inversions in athletes fulfilling LVNC criteria were mostly present in the anterior leads, although comparison with patients with LVNC did not achieve statistical significance (10.0% vs 4.0%; p=0.23). There was also a trend towards an increased prevalence of deep T-wave inversions (−0.2 mV) in patients with LVNC compared with athletes fulfilling LVNC criteria, which also failed to achieve statistical significance. (17% vs 7.5%; p=0.06).
Patients with LVNC demonstrated a larger LV end-diastolic cavity (2.9±0.7 cm/m2; range 2.0–5.1; vs 2.6±0.4 cm/m2; range 1.8–3.9; p=0.0006) and left atrial area (2.0±0.4 cm/m2; vs 1.7±0.2 cm/m2; p=0.0001) as well as significantly abnormal indices of LV systolic ejection fraction (EF: 46.3%±19.3%; vs 60.3%±8.3%; p<0.0001, S′ septal 6.4 cm/s±1.7 cm/s vs 8.8 cm/s±1.6 cm/s; p<0.0001 and S′ lateral 7.0 cm/s±2.5 cm/s; p<0.0001) and diastolic function (E/A ratio: 1.6±0.8 vs 2.0±0.6; p<0.0001) compared with athletes fulfilling LVNC criteria.
Distribution of left ventricular trabeculation
No single pattern of distribution of trabeculations discriminated between patients with LVNC and athletes fulfilling LVNC criteria. However, patients with LVNC expressed increased trabeculations in the apical region compared with athletes fulfilling LVNC criteria (68% vs 47%; p<0.0001) and athletes fulfilling LVNC criteria revealed a higher prevalence of trabeculations in the mid-cavity region compared with patients with LVNC (53% vs 27%; p<0.0001).
The ‘gray zone’
An important minority of athletes (N=10; 0.9%) fulfilling LVNC criteria also exhibited deep T-wave inversions and depressed LV systolic function (ejection fraction of ≤50%) and consisted of 3.4% (n=5) of black athletes and 0.5% (n=5) of white athletes. The demographic and clinical characteristics of these athletes are presented in table 5. All athletes had normal indices of diastolic function.
Demographic data on the 10 athletes with LVNC criteria and reduced systolic function
All 10 athletes underwent 48 h ECG monitoring, a conventional exercise stress test using the Bruce protocol and cardiac MRI to investigate the broader phenotypic features of LVNC. None showed non-sustained ventricular tachycardia or >500 ventricular extrasystoles during 48 h Holter. All athletes exercised to exhaustion and achieved ≥90% of their age-predicted heart rate with an appropriate rise in blood pressure. None developed sustained ventricular arrhythmias during or post exercise. Echocardiography performed immediately after exercise revealed hyperdynamic LV contraction.
All athletes with echocardiographic LVNC criteria also fulfilled the Petersen cardiac MRI criteria for LVNC,16 and revealed a subnormal LV ejection fraction on cardiac magnetic resonance (CMR) (49.3%±1.4%; range 48–51%). None exhibited late enhancement following gadolinium. During a mean follow-up of 48.6±14.6 months, all athletes remained asymptomatic and free of adverse events.
Determinants of increased LV trabeculations in athletes
Univariate analysis demonstrated a significant association between increased LV trabeculation, African/Afro-Caribbean ethnicity and T-wave inversion. Black athletes were more likely to exhibit increased trabeculation (OR: 2.06; 95% CI 1.39 to 3.08, p<0.001). There was no significant association between increased LV trabeculation, age, sex, BSA, hours of training per week, LV end-diastolic cavity size and maximal-LVWT. Multivariable analysis revealed that after adjusting for ethnicity, T-wave inversion was independently associated with athletes exhibiting increased LV trabeculation compared with athletes that did not show increased LV trabeculation (OR 3.46, 95% CI 1.26 to 9.51, p=0.016).
Intraobserver variability/interobserver variability
There were two cases of disparity with respect to increased LV trabeculation during reanalysis by first author (SG) translating to a κ (measurement of agreement)=0.99 (p<0.0001). There were 10 cases of disparity between SG and an independent reviewer (MR) translating to a κ 0.84 (p<0.0001). All 12 cases were excluded from the athletic group with increased LV trabeculation following review by the senior author (SS).
Discussion
This study reveals that almost 20% of the athlete cohort expressed an increased number of LV trabeculation and almost 10% athletes fulfilled established echocardiographic LVNC criteria. When consideration is given to the fact that an increasing number of sporting organisations are investigating athletes with ECG and echocardiography, our observations have serious ramifications.
Given the high prevalence of athletes fulfilling LVNC criteria compared with the low prevalence of cardiomyopathies implicated in SCD in young athletes, it is likely that in most athletes these LV morphological anomalies represent a non-specific epiphenomenon that has become increasingly conspicuous through improvements in echocardiographic image resolution. Our multivariable analysis did not provide any strong associations between the presence of increased LV trabeculation and sporting discipline, or training intensity, to enable any concrete inferences relating to the generation of this phenomenon in athletes. The very fact that almost 10% of athletes revealed features that could be consistent with LVNC compared with none of their sedentary counterparts indicates that the increased LV trabeculation observed in athletes may be partly explained by a consequence of, or response to, the high cardiac preload and afterload demands associated with intensive physical exercise. The greater prevalence of increased LV trabeculation in black athletes suggests that genetic factors may also play an important role.
It is well recognised that athletic training is associated with electrical and structural modifications that may overlap with those observed in primary myocardial disorders. Our athletes fulfilling criteria for LVNC exhibited a relatively high prevalence of T-wave inversions which are also common in patients with other cardiomyopathies implicated in exercise related SCD.5 ,17 However, the specific pattern and distribution of these changes was consistent with normal variations based on consensus documents pertaining to interpretation of the athlete's ECG in Europe15 and the USA18 which accept anterior T-wave inversion in black athletes.19 In contrast, patients with LVNC had a high prevalence of T-wave inversion in the inferior and lateral leads, which is not usually considered indicative of athletic training in Caucasian athletes at least.
A significant number of athletes (64%) fulfilling criteria for LVNC and patients with LVNC exhibited LV cavity dimensions ≥54 mm. In contrast with patients with LVNC, almost all athletes fulfilling criteria for LVNC demonstrated normal indices of systolic (89%) and diastolic function (100%).
Of concern, was the observation that a small minority of athletes (n=10; 0.9%) fulfilling criteria for LVNC also exhibited marked repolarisation changes as well as depressed basal systolic function, a finding that was also recently reported in a small cohort of Dutch football players.20 Our study demonstrated that such abnormalities were more common in black athletes compared with Caucasian athletes (3.4% vs 0.5%; p=0.012) and could be considered to be indicative of incomplete expression of the LVNC phenotype in predisposed athletes, that may be unmasked through intensive exercise (figure 4). Conversely these manifestations may represent conventionally atypical features of cardiac adaptation similar to those reported previously.21 Indeed, none of the 10 athletes in question reported symptoms, an ominous family history or additional ECG anomalies, which would be highly suggestive of cardiac pathology. Furthermore, indices of diastolic function were normal. Comprehensive assessment failed to reveal any other features of the disease phenotype; there were no arrhythmias during exercise or Holter monitoring, the exercise echocardiogram showed normal systolic function and there was no evidence of late enhancement on the cardiac MRI following gadolinium. Based on our assessments we did not feel there was sufficient evidence of a cardiomyopathy to warrant disqualification from competitive sport and none of these athletes experienced adverse events during a subsequent follow-up period of over 4 years.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Potential significance of increased left ventricular (LV) trabeculation in young individuals engaging in intensive physical training. In the majority of athletes, increased LV trabeculation are likely to represent expressions of physiological cardiac remodelling. However, a small minority may express a triad of reduced LV systolic function, repolarisation changes raising suspicion of left ventricular non-compaction. EF; ejection fraction; FS, fractional shortening; LV, left ventricle; LVED, left ventricular end-diastolic diameter; LVH, left ventricular hypertrophy.
Conclusions
A high proportion of athletes fulfil conventional criteria for LVNC without other phenotypical features of the disorder. The presence of increased LV trabeculation or even echocardiographic criteria for LVNC in isolation is probably of little significance and may be regarded as part of the spectrum of the ‘athlete's heart.’ Indeed more stringent criteria for the consideration of a diagnosis of LVNC are required to minimise the risk of overdiagnosis in this cohort, and prevent unnecessary and expensive investigation with advanced imaging techniques. Following ECG and echocardiography 0.9% of highly trained athletes demonstrate concomitant T-wave inversion and reduced baseline indices of systolic function that may be considered diagnostic of LVNC. This grey zone is considerably smaller than that observed in athletes overlapping with the HCM phenotype following echocardiography. A more protracted longitudinal evaluation and assessment of first degree relatives is required in the small group of athletes with this triad to ascertain the true prevalence of LVNC in athletes.
Limitations
Our observations and conclusions regarding increased LV trabeculation and criteria for LVNC in athletes were based on echocardiographic criteria although cardiac MRI may be considered the ‘gold-standard’ assessment for myocardial trabeculation. However, our study represented a realistic situation of preparticipation cardiac evaluations, which rely on ECG and echocardiography. Although, the follow-up period of athletes was a respectable 48.6±14.6 months, the authors recognise that the duration of surveillance is probably too short to identify adverse events for most cardiomyopathies. Due to the lack of co-operation from the athletes in the ‘grey zone’, we were unable to study the impact of detraining on LV morphology; the regression of increased trabeculation would have favoured a physiological process. Finally, evaluation of first-degree relatives in athletes with increased LV trabeculation may have provided valuable data in establishing whether increased LV trabeculation in our athletes, particularly those fulfilling conventional criteria for LVNC, has a familial component or is merely part of a physiological cardiac remodelling process to exercise.
Acknowledgments
The authors are grateful to Cardiac Risk in the Young (CRY) for providing the portable echocardiography equipment and ECG machines used for the study in the UK. The authors would also like to acknowledge Azra Loncarevic-Srmic and Rebecca Howes who assisted in the collection and collation of data.
References
Footnotes
SG and NC contributed equally.
-
Contributors SG: Study design/planning, data collection/conduct and preparation/reporting of manuscript. NC, RLB, MR, GK, VFP, SG, NS, AZ, MW: Study design, data collection and preparation of manuscript. MP, FC: Interpretation of data, revision of manuscript for intellectual content. SS: Lead for study, study design, data collection, quality control of data, preparation of manuscript, responsible guarantor of overall content.
-
Funding S Gati, MR, NC, S Ghani, AZ, NS were funded by research grants from CRY. SS has been co-applicant on previous grants from CRY to study African/Afro-Caribbean athletes. Studies on French athletes were supported by grants from the Club des Cardiologues du Sport and from the French Ministry of Health and Sport.
-
Competing interests None.
-
Ethical approval The National Research Ethics Service, Essex-2 Research Ethics Committee and French Ministry of Health and Youth.
-
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Correction