Article Text

Abstract
Objectives To test whether symptoms revealed on exercise testing in patients with moderate or severe aortic stenosis are associated with changes in left ventricular systolic function and to investigate the ability of resting measures to predict peak cardiac index.
Methods In a prospective study of asymptomatic aortic stenosis, 38 patients with a median age of 63 years (range 29–83) and an effective aortic orifice area by the continuity equation of less than 1.5 cm2 had echocardiography, measurement of blood B-type natriuretic peptide (BNP) level and exercise haemodynamic testing using an inert gas rebreathing device.
Results Revealed symptoms occurred in 10 patients in whom peak cardiac index (p=0.002), stroke index (p=0.024) and maximum oxygen consumption (VO2) (p=0.003) were lower than in those without symptoms. Univariate predictors of peak cardiac index were Doppler tissue peak systolic velocity (p=0.004, r=0.45), the ratio of peak transmitral E velocity to Doppler tissue Ea velocity (p=0.039, r=−0.34) and log BNP (p<0.001, r=−0.71). The only independent predictor of peak cardiac index was the log BNP level (p<0.001, r=−0.71).
Conclusions Revealed symptoms on treadmill exercise in apparently asymptomatic aortic stenosis were associated with lower peak myocardial VO2 and lower peak stroke index during exercise. The strongest resting predictor of revealed symptoms and of peak cardiac index was the blood BNP level.
- Aortic stenosis
- cardiac index
- exercise testing
- haemodynamics
- symptoms
- AS
- Aortic stenosis
- BNP
- B-type or brain natriuretic peptide
- E/Ea
- Ratio of peak transmitral E velocity to Doppler tissue Ea velocity
- S
- Peak Doppler tissue septal shortening velocity recorded at the septum
- SAC
- Systemic arterial compliance
- SV
- Stroke volume
- VO2
- Oxygen consumption
Statistics from Altmetric.com
- AS
- Aortic stenosis
- BNP
- B-type or brain natriuretic peptide
- E/Ea
- Ratio of peak transmitral E velocity to Doppler tissue Ea velocity
- S
- Peak Doppler tissue septal shortening velocity recorded at the septum
- SAC
- Systemic arterial compliance
- SV
- Stroke volume
- VO2
- Oxygen consumption
Surgery in severe aortic stenosis (AS) is indicated for spontaneous symptoms on interview and left ventricular systolic dysfunction on echocardiography at rest.1 However, at least 3%, and up to 11%, of patients die soon after the onset of symptoms before aortic valve surgery can be performed.2–4 Ideally patients should, therefore, be identified immediately before the development of spontaneous symptoms to allow elective surgery to be planned. A number of studies5–7 has suggested that symptoms can be revealed by exercise testing in apparently asymptomatic patients. However, the validity of differentiating pathological from physiological breathlessness has been questioned, and revealed symptoms are only a class IIb indication for surgery in current American guidelines,1 whereas they are a class I indication in European guidelines.8 It would validate the status of revealed symptoms if they were associated with abnormalities of an objective physiological measure. ST segment depression is known to be non-specific in AS because of the presence of left ventricular hypertrophy,9 10 and a blunted rise in blood pressure has been of limited predictive use.9 10 Early work11 12 suggests that measures of left ventricular systolic function are likely to be more useful.
In investigating the determinants of changes of left ventricular function on exercise, the aortic valve and aorta need to be considered as a unit both anatomically and physiologically.13–16 It is not known whether measures of aortic physiology may also predict the presence of symptoms revealed on exercise.
The primary aim of this study was to investigate whether symptoms revealed on exercise testing in apparently asymptomatic patients were associated with abnormalities of left ventricular systolic function. We also investigated whether measures of aortic valve and aortic function at rest correlated with revealed symptoms or cardiac index.
Methods
Patients
The 65 patients from a prospective cohort with asymptomatic AS and an effective orifice area by the continuity equation (EOA) of less than 1.5 cm2 were approached for inclusion. Lack of symptoms was determined with a detailed history and the Canadian specific activity scale.17 Patients were excluded from the study if they had: impaired left ventricular transverse systolic function as defined by a fractional shortening less than 28% or regional wall motion abnormalities; more than mild concomitant valvular disease; significant pulmonary disease; or pulmonary hypertension.
All patients underwent transthoracic echocardiography including tissue Doppler, measurement of blood B-type natriuretic peptide (BNP) level and exercise stress testing with haemodynamic monitoring. The study was approved by the local ethics committee and all patients gave written, informed consent. Coronary angiography was not part of this study but was requested as clinically indicated by the cardiologist with responsibility for the clinical care of the case. Coronary lesions were graded by eye as severe (>75% luminal diameter) or 50–75% or subcritical (<50%).
Echocardiography
A Vingmed system 5 (GE Medical, Milwaukee, Wisconsin, USA) was used with a 3–2 20 mm duplex probe and 1.9 MHz continuous wave stand-alone probe. Pulsed Doppler recordings were made in the apical four-chamber view at the tips of the mitral valve leaflets and in the five-chamber view just below the aortic valve. These signals were used to obtain early transmitral (E) filling velocity and the velocity time integral and mean pressure difference of the subaortic flow, respectively. Tissue Doppler recordings were made from the apical four-chamber to give the peak shortening systolic velocity (S′) and the early diastolic velocity (Ea). The ratio of peak transmitral E velocity to Doppler tissue Ea velocity (E/Ea) was calculated.18 19 Continuous wave recordings were made from the apex and right intercostal positions to obtain peak velocity, derived peak and mean pressure difference and velocity time integral. The EOA in cm2 was calculated by the classic continuity and indexed to body surface area calculated using the modified Dubois formula.20 Left ventricular mass was calculated by the ASE formula.21 Left ventricular stroke work loss (SWL) was calculated as a measure of the flow-independent index of AS severity by the formula:16
B-type natriuretic peptide
After 30 min rest following the echocardiogram and before the exercise test, whole blood was collected from a forearm vein into 4.5 ml EDTA tubes. Serum BNP was analysed within 4 h using the Triage BNP assay (Biosite Diagnostics, San Diego, USA), which uses the fluorescent intensity of BNP-tagged antibodies.
Exercise testing with haemodynamic monitoring
Exercise testing was performed with a Marquette Case 8000 system (GE Medical) according to American College of Cardiology/American Heart Association practice guidelines22 using a Bruce protocol modified by two warm-up stages.23 During the exercise test, haemodynamic measures were recorded using an inert gas rebreathing device (Innocor; Innovision, Odense, Denmark), which uses photoacoustic spectrometry and correlates well with both the direct Fick method and thermodilution.24–26 The patients breathed though a hermetically sealed circuit containing an oxygen-enriched gas mixture of 0.1% sulphur hexafluoride (insoluble in blood) and 0.5% nitrous oxide (blood soluble) contained in a 3 litre rubber bag. The concentration of nitrous oxide decreases during the rebreathing manoeuvre with a rate proportional to pulmonary blood flow. A constant ventilation rate was ensured by having the subject breathe in synchrony with a graphical tachometer on a computer screen, and a constant ventilation volume was ensured by requesting the subject to empty the rebreathing bag with each breath. Inert gas rebreathing was conducted before the commencement of the exercise test, at each stage during exercise and then during recovery.
Cardiac output and index were calculated by the Innocor (Innovision) device and the stroke index was derived as the quotient of the cardiac index and the heart rate. Mean stroke index, mean cardiac index and mean oxygen consumption (VO2) were calculated at every stage. The number of patients in whom the stroke index failed to rise by more than 10% throughout the test or fell during the first stage was noted.
Systemic arterial compliance was estimated using the stroke index divided by the pulse pressure measured from the brachial cuff. Systemic vascular resistance (SVR) was calculated as (80 × mean arterial pressure/cardiac output). As a measure of resting global left ventricular afterload the valvulo-arterial impedance (Zva) was calculated:14
Cardiac power output was calculated as the product of cardiac output and the mean arterial blood pressure. Circulatory power was calculated as the product of VO2 and systolic arterial pressure using, for peak circulatory power, the peak VO2 and the last systolic arterial pressure measurement. When the systolic arterial pressure measurement was not obtained at peak exercise, we considered the value measured at the previous stage. Circulatory stroke work was calculated as the circulatory power divided by heart rate.
The exercise test was defined as positive by an experienced cardiac physiologist if it was stopped prematurely because of limiting breathlessness, chest discomfort or dizziness rather than by quickly reversible minor breathlessness.5 Other predetermined criteria for cessation were ST segment depression of greater than 5 mm measured 80 ms after the J point, more than three consecutive ventricular premature beats and a fall in SBP by more than 20 mm Hg from baseline,9 although in practice no test was terminated for any of these reasons. Otherwise the test continued until the patient was fatigued. The physiologist was blinded to the results of the Innocor (Innovision), which was operated by the attending cardiologist and was analysed at a later date.
Statistical analysis
All continuous variables included in the analysis are presented as mean±SD, whereas non-continuous variables are presented as median (range). Univariate analyses were performed on continuous variables using an independent samples t test for parametric data and the Mann–Whitney U test for non-parametric data. For the determinants of peak cardiac index, multivariate forward linear stepwise regression was conducted. Statistical significance for all variables was set at the 5% level. All data were collected and analysed using SPSS statistical software (Chicago, USA) version 14.0.1.
Results
Of the 65 patients approached for inclusion, 10 declined and 17 were unable to use the cardiac output machine or produced data that failed the machine's intrinsic quality control tests. The remaining 38 patients had a median age of 63 years (range 29–83) and 32 (84%) were men. This was similar to the main cohort, median age 66 years (range 29–87) of whom 47 (72%) were men. The AS was severe (EOA <1.0 cm2) in 18 and moderate (EOA 1.0–1.5 cm2) in 20 patients (table 1). Twelve of 38 (32%) patients were on regular B-blockade therapy, five of 38 (13%) patients were on calcium channel antagonists, eight of 38 (21%) patients were on ACE inhibitors, 18 of 38 (34%) patients were on statins and three of 38 (8%) patients were on nitrate therapy. Table 2 gives the cardiovascular risk factors for the patient cohort. One patient had diabetes mellitus and 14 of 38 (37%) patients had hypertension.
Resting echocardiographic characteristics
Population cardiovascular risk factors
Ten patients developed symptoms on exercise, seven of 18 (39%) with severe and three of 20 (15%) with moderate AS (two with EOA 1.3 cm2 and one with EOA 1.0 cm2). Six patients developed chest discomfort and four exertional dyspnoea. No patient experienced pre-syncope. Coronary angiography was performed in all seven patients with severe AS and showed normal anatomy in three, subcritical disease (<50%) in two, a 50–75% lesion in one and severe disease in one. Of the patients with moderate AS, one had severe disease of all three main epicardial arteries and another had 50–75% lesions of all three main epicardial arteries. The third had had coronary artery bypass grafting (CABG) in 1995, but was 80 years old and did not have spontaneous symptoms, so the decision was to continue medical treatment without further angiography.
Haemodynamic measures at rest and on exercise
The exercise time was 636 s (±191) in those with symptoms compared with 933 s (±149) in those who did not develop symptoms (p<0.001). Resting haemodynamic measures were similar (table 3). The myocardial maximum VO2 was similar in the two groups at comparable exercise times (figure 1A), although the peak level was higher in asymptomatic patients (table 3). The stroke index rose in the first minute of exercise in asymptomatic patients then remained approximately constant throughout exercise and declined during recovery (figure 1B). By contrast, in those who developed symptoms, the mean stroke index fell throughout exercise and returned to resting levels during recovery (figure 1B). The stroke index failed to rise by more than 10% from rest to peak exercise in eight of 10 (80%) patients with symptoms and in 15 of 28 (53%) patients with no symptoms. Six (60%) patients in the symptomatic group had a fall in stroke index within the first stage of exercise compared with only five (18%) patients within the asymptomatic group. There was no relationship between concurrent B-blockade use and the stroke volume index response during exercise (p=0.08). The heart rate increased more in those patients who were asymptomatic so that differences in cardiac index were smaller, but still statistically significant (figure 1C, table 3). The mean rise in blood pressure was 14±21 mm Hg in the symptomatic group and 23±15 mm Hg in the asymptomatic group (p=0.165). The measures derived from cardiac output and blood pressure, cardiac power output and circulatory power, were significantly lower in the group with revealed symptoms. There was a mean 2.2 mm (±1.7) ST depression in the symptomatic group and 0.9 mm (±1.5) ST depression in the asymptomatic group (p=0.025). SVR fell less during exercise in those with revealed symptoms and the difference between the two groups was statistically significant at peak exercise. Systemic arterial compliance also fell less in the group with revealed symptoms, but the difference was not significantly different at rest or at peak exercise (table 3).
Haemodynamic and vascular function at rest and peak exercise in patients with and without symptoms on exercise

(A) Myocardial oxygen consumption (VO2 max) during the treadmill exercise test. Mean results are shown at rest, during exercise and in recovery for patients who developed symptoms (group 1, front) and those who were asymptomatic (group 2, back). The legend gives the mean (SD) at each stage of exercise for both groups of patients. (B) Stroke volume index (SVi) during the treadmill exercise test. Mean results are shown at rest, during exercise and in recovery for patients who developed symptoms (group 1, front) and those who were asymptomatic (group 2, back). The legend gives the mean (SD) at each stage of exercise for both groups of patients. (c) Cardiac index (Ci) during the treadmill exercise test. Mean results are shown at rest, during exercise and in recovery for patients who developed symptoms (group 1, front) and those who were asymptomatic (group 2, back). The legend gives the mean (SD) at each stage of exercise for both groups of patients.
Resting correlates of revealed symptoms
The EOA index was significantly lower in those developing symptoms and there were non-significant trends towards higher transaortic pressure differences in those developing symptoms (table 4). Measures of left ventricular function including fractional shortening and tissue Doppler parameters (table 4) were similar in those with and without symptoms, and measures of aortic physiology did not differ (table 3). By contrast, BNP levels at rest were significantly higher in those who developed symptoms (186±146 pg/ml) than in those who were asymptomatic (55±55 pg/ml) (table 2).
Echocardiographic variables and BNP in patients with or without symptoms on exercise
Factors affecting peak haemodynamic performance
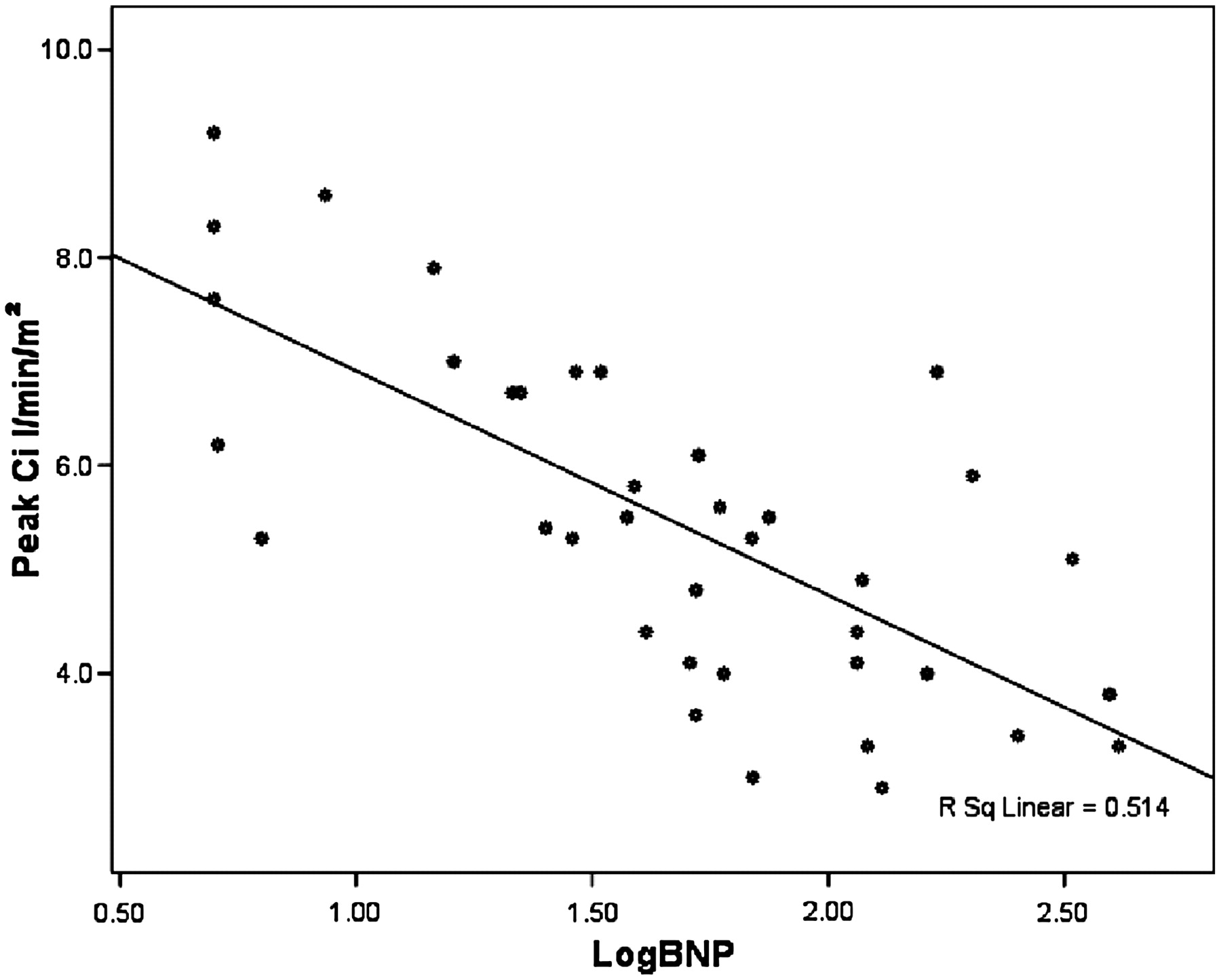
Log BNP levels were inversely related to peak cardiac index (p<0.001, r=−0.71) (figure 2), whereas there were weaker relationships with tissue Doppler systolic velocity (p=0.004, r=0.45), and the E/Ea ratio (p=0.039, r=−0.34). No measures of aortic valve stenosis were related to the peak cardiac index: EOA (p=0.2), EOA index (p=0.3), peak gradient (p=0.4), mean gradient (p=0.6) and SWL (p=0.44). SVR was related to the peak cardiac index (p=0.013, r=−0.40), but there was no relationship with systemic arterial compliance (p=0.94) or the SWL (p=0.44). There was no significant relationship between peak cardiac index and either the change in SBP on exercise (p=0.07, r=−0.29), or maximum ST segment depression (p=0.44, r=−0.13) or the change in systemic arterial compliance (p=0.136) or the change in SVR (p=0.762). Using multivariate stepwise linear regression, only the log BNP level was independently related to peak cardiac index.

{kind=link}
{kind=link}
Plot of peak cardiac index against log B-type natriuretic peptide (BNP). The relationship between peak cardiac index (Ci) and log BNP.
Discussion
Patients with apparently asymptomatic AS with symptoms revealed by exercise testing had lower peak myocardial VO2 and lower peak stroke index than those patients who remained asymptomatic. The differences in stroke index were apparent at all levels of exercise and were not an artefact of shorter exercise times. The most powerful resting determinant of peak cardiac index and also the development of symptoms was the blood BNP level.
Little previous work exists. Lee et al27 showed normal increases in stroke volume on exercise measured invasively in patients with mild and moderate AS. However, in patients with symptomatic severe AS, stroke volume was significantly decreased at rest and on exercise. Otto et al28 observed a slight decrease in stroke volume after exercise in 28 asymptomatic patients with AS using Doppler echocardiography. Clyne et al11 showed that maximum VO2 was lower in 14 patients with symptoms compared with controls. However, none of these studies compared patients with and without symptoms revealed by exercise. Marechaux et al12 showed that patients with a fall in ejection fraction on exercise were more likely to develop symptoms than those in whom the ejection fraction rose on exercise. Similarly, Lancellotti et al29 demonstrated that an abnormal exercise response in patients with asymptomatic AS was mediated by impaired contractile reserve and a relatively large increase in gradient. The findings of both of these studies are consistent with ours and support the idea that the left ventricular response to exercise is abnormal in apparently asymptomatic AS and more abnormal in those within this group who have symptoms revealed on exercise than in those who remain asymptomatic. We did not find a clear cut-off in exercise response, but a fall in cardiac index within the first stage of exercise occurred in 60% with symptoms and in only 18% without symptoms. We and others have already shown that revealed symptoms are associated with cardiac events and the development of spontaneous symptoms within 1 year,5 6 but it is unconfirmed whether the addition of the change in stroke index would improve the prognostic ability of symptoms alone.
We looked for possible resting determinants of revealed symptoms and an abnormal left ventricular systolic response to exercise. We found that indexed EOA was lower in those with symptoms. No echocardiographic measure of left ventricular function was predictive although our population included patients only with preserved systolic function. Even within this group, however, the blood BNP level was significantly higher in those in whom symptoms were revealed and the resting BNP correlated inversely with peak cardiac index (figure 2). This is consistent with studies showing that BNP levels are higher in patients with spontaneous symptoms and tend to rise before symptoms develop.30 31 We have previously shown in another population that BNP levels are higher in patients with revealed symptoms.32 These observations suggest that the BNP level is a more sensitive marker than resting echocardiographic measures for early decompensation manifesting as abnormal systolic function and revealed symptoms on exercise. It is likely that BNP could be used routinely in the follow-up of patients with AS to help determine the need for exercise testing and the frequency of follow-up.32
In contradistinction to previous studies13 we did not find a significant effect from aortic physiology, probably because aortic compliance was relatively mildly impaired in our population. However, we noted a trend towards a blunted fall in SVR associated with revealed symptoms, which is in agreement with Laskey et al.15 There are other potential causes of a blunted rise in VO2 including peripheral vascular or skeletal muscle deconditioning and coronary disease. Three of the nine patients with revealed symptoms had stenoses greater than 50% on coronary angiography and the tenth had had CABG. All three with symptoms and moderate AS had coronary stenoses greater than 50%. We did not address coronary disease statistically because we did not have ethics approval to perform coronary angiograms in patients who remained asymptomatic.
AS, coronary disease and reduced aortic compliance exist as a continuum making it difficult and, arguably, clinically unrealistic to identify a pure sample. We included patients with moderate AS because these are known to develop revealed symptoms on exercise,5 and when associated with low aortic compliance have as high an incidence of left ventricular systolic and diastolic dysfunction as those with severe AS and normal aortic compliance.13 The effect of coronary disease can occur with minor angiographic findings at angiography,33 and because of this it is usual in the literature to study measures of aortic valve or aortic physiology without integrating the effect of coronary disease.12–14 We believe that revealing symptoms by exercise, whatever their origin, is useful clinically because it suggests that invasive intervention should be considered. In some patients this will most appropriately be percutaneous coronary interventionI, in others CABG with aortic valve replacement or in others aortic valve replacement alone. In our experience in this and other studies, it is rare to reveal symptoms in apparently asymptomatic patients with EOA greater than 1.3 cm2, suggesting that this could be a threshold for exercise testing in clinical practice.
This study has limitations. The population size is small. It would have been ideal to have had coronary angiography in all cases, but this was not feasible ethically. We argue, as have others,13 that the inclusion of patients with coronary disease reflects clinical reality although their exclusion would undoubtedly have given a neater, more homogeneous study group. Furthermore, the inclusion of patients with coronary disease is expected to have reduced rather than enhanced the predictive power of BNP. The determination of dyspnoea during exercise testing was largely subjective but was validated by the attending physician being blinded to the results of the haemodynamic monitoring and the association with an abnormal haemodynamic response.
In conclusion, this study shows that symptoms revealed by exercise testing in apparently asymptomatic patients with AS have a lower peak VO2 and a reduced peak stroke index. This suggests that revealed symptoms are genuine and not an artefact of interpretation. The strongest resting predictor of revealed symptoms and of peak cardiac index was the blood BNP level.
References
Footnotes
Competing interests None.
Ethics approval This study was conducted with the approval of the St Thomas' Hospital Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.