Article Text

Abstract
Background Little is known about the gender differences of patients undergoing aortic valve replacement (AVR) for isolated severe aortic stenosis.
Methods and Results 408 consecutive patients (215 women and 193 men; p=0.9) were analysed. At presentation, women were older (73.7±9.3 years vs men 66.5±11.5 years; p<0.001), more symptomatic (New York Heart Association (NYHA) class: women 2.3±0.7 vs men 2.0±0.65; p<0.001), and presented with smaller valve areas (women 0.6±0.2 cm2 vs men 0.7±0.2 cm2; p<0.001) and higher mean pressure gradients (women 67.3±19.2 mm Hg vs men 62.2±20.0 mm Hg, p=0.001). Despite older age and more advanced disease in women, operative mortality did not differ. Survival after AVR by Kaplan–Meier analysis tended to be even better in women (92.8%, 89.8%, 81.4% vs men 89.1%, 86.6%, 76.3% at 1, 2 and 5 years, p=0.31). After division into age quintiles, the outcome of women was significantly better in patients older than 79 years (p=0.005). After adjustment for clinical characteristics, gender did not predict operative mortality and late outcome. Despite physical improvement in both groups after surgery, women remained more symptomatic (NYHA class: women 1.6±0.7 vs men 1.3±0.4; p=0.001).
Conclusion Although women referred to AVR are older and more symptomatic, operative and long-term mortality are not increased. In the oldest age group of 79 years and older, women even have a better outcome, presumably due to a longer mean life expectancy.
- Aortic valve disease
- gender
- surgery-valve
Statistics from Altmetric.com
Aortic stenosis (AS) has become the most common heart valve disease and has been extensively studied in recent years. Although gender differences receive increasing attention in cardiology, only a small number of studies have investigated gender-specific differences in patients with AS with regard to clinical presentation and surgical outcome after aortic valve replacement (AVR).1–8 In addition, these few studies reported conflicting results. Whereas some authors1 7 showed an increased short-term mortality in women, others6 reported better long-term survival of women or no sex-related differences in outcome.2 8 In addition, most of the studies were primarily focussing on left ventricular geometry and function and paid less attention to differences in outcome and morbidity after AVR. Gender differences in AS and their potential impact on surgical treatment thus still require elucidation.
Therefore, we studied a large series of consecutive patients referred for AVR for AS with regard to gender differences in clinical presentation and surgical outcome.
Methods
Patient population
All patients (408) who were seen between January 1998 and January 2005 in our valvular heart disease outpatient clinic and who were eventually referred to AVR because of isolated severe AS (peak velocity ≥4 m/s, mean pressure gradient ≥40 mm Hg in the presence of normal left ventricular function, calculated valve area <1.0 cm2) were consecutively included in this study. The indication for surgery was given when patients were symptomatic (exertional dyspnoea, New York Heart Association (NYHA) functional class ≥II; exertional angina pectoris, Canadian Cardiovascular Society (CCS) class ≥II, syncope) or when left ventricular function was reduced (ejection fraction ≤50%) without other explanations in asymptomatic patients. Those patients who were primarily referred to surgery for coronary artery bypass grafting and additionally received an aortic valve prosthesis for non-severe AS were not included. Patients with more than mild concomitant aortic regurgitation or additional valve disease were also excluded. The Ethics Committee of the Medical University of Vienna approved the study protocol.
Study protocol
At study entry all patients had a physical examination, ECG, echocardiogram and coronary angiogram before surgery. In addition, the following clinical data were collected: age, gender, height, weight, NYHA and CCS functional class, history of hypercholesterolaemia (cholesterol >200 mg/dl or patient on lipid-lowering therapy at study entry), diabetes mellitus (fasting blood glucose >110 mg/dl or use of antidiabetic medication/insulin), hypertension (blood pressure >140/85 mm Hg on the basis of the average of repeated measurements or patient on antihypertensive medication), chronic renal insufficiency (creatinine ≥2 mg/dl), presence of chronic obstructive pulmonary disease (long-term use of broncholytic therapy) and coronary artery disease (angiographically documented coronary artery stenosis). Furthermore, the EuroSCORE was calculated in each patient to evaluate the operative risk.9 10
Patients were re-evaluated 3–9 months after AVR, and at intervals between 1 and 3 years thereafter, including history with an evaluation of functional status (NYHA and CCS class), physical examination, ECG and echocardiography.
Operative mortality was defined as death from any cause within 30 days after operation if the patient was discharged from hospital or within any interval if the patient was not discharged.11
For the assessment of outcome, the primary endpoint was death. Operative as well as late deaths were included in the analysis. Deaths were classified as cardiac or non-cardiac on the basis of a review of medical records, including autopsy records and death certificates, which were available in all cases.
For the assessment of outcome with regard to morbidity, postoperative symptoms and functional status at last follow-up were assessed.
Echocardiography
A comprehensive echocardiographic examination including M-mode echocardiography, two-dimensional echocardiography and conventional and colour Doppler ultrasonography were conducted by experienced echocardiographers. Echocardiographic data were obtained with commercially available ultrasound machines. Assessment of AS included peak and mean transvalvular gradients and the aortic valve area as obtained from the continuity equation. Wall thickness of the left ventricle was assessed by standard measurement of septal and posterior wall thickness.
Coronary angiography
Preoperative coronary angiography was performed in all patients. Reduction of the diameter of 50% or greater was considered to define significant left main stenosis. A cut-off value of 70% was used for the right coronary artery, left descending and circumflex arteries. Multivessel coronary artery disease was defined as the presence of significant stenoses in two or more vessels.
Statistical analysis
Statistical analysis was performed using SAS 9.1 for Windows.
Continuous variables were expressed as mean±SD and compared between groups using the two-sided two-sample Student's t test. Not normally distributed variables were transformed by using the logarithm function to achieve normal distribution. Normal distribution was then checked by looking at histograms. Categorical variables were expressed as frequency percentages and compared between groups by the χ2 test or Fisher's exact test, when cells with expected cell frequencies of less than five were present. Kaplan–Meier estimates were used to calculate the 1, 3 and 5-year survival. Differences between survival curves of male and female patients were analysed using log rank tests.
To determine the effect of gender on long-term survival, a multivariable Cox regression was performed. All variables that showed p values of less than 0.05 in a univariable analysis and that showed p values below 0.1 in a joint non-stepwise multivariable analysis were used as covariables in the multivariable Cox regression. The following influence factors were assessed: metric: body surface area, body mass index, age, EuroSCORE; dichotomous: sex, presence of diabetes, hypertension, coronary artery disease, coronary artery disease of two or more vessels, coronary artery disease of three vessels, left ventricular dysfunction, peripheral vascular disease, previous cardiac surgery, renal dysfunction, concomitant aortocoronary bypass surgery; to assess influence parameters on operative mortality, a multiple logistic regression was performed in the same way as the Cox regression for long-term survival. In addition, the effect of gender was tested in quintiles of age.
Results
Preoperative presentation
Preoperative clinical data
Preoperative patient characteristics are shown in table 1. Of the 408 patients, 215 were women. Female patients were significantly older (p<0.001) with 48.4% of them being older than 75 years compared with only 24.9% of men (p<0.001). Women were more symptomatic preoperatively (p<0.001), they more frequently suffered from exertional dizziness (p<0.001) and more often had hypertension (p<0.001). The additive EuroSCORE was significantly higher in women (p<0.001).
Baseline clinical characteristics
Preoperative echocardiographic data
Table 2 shows the echocardiographic data at baseline. Women presented with smaller valve areas indexed to the body surface area (p=0.03) and higher mean pressure gradients (p<0.001). Left ventricles were smaller in women (p<0.001), however, after adjusting for body surface area no difference was present (p=0.2). Similarly, left ventricles were less hypertrophied in women in absolute terms (p<0.008) but when adjusted for left ventricular size the difference disappeared (p=0.8). Systolic pulmonary artery pressure was higher in female than in male patients (p=0.04).
Echocardiographic data at baseline
Surgery
Three hundred and sixty-seven (192 women and 175 men) of the 408 patients originally referred for surgery eventually underwent AVR. Thirty-seven patients were not treated surgically for the following reasons: 16 patients refused surgery despite recommendation (10 women and seven men), 11 patients died on the waiting list (seven women and four men), 10 patients were not operated because of a high-risk profile and significant comorbidity (five women and five men). Four patients were lost to follow-up (two women and two men). Of those who died on the waiting list, eight patients were classified as cardiac death (five women and three men), the others died of stroke (one woman), aplastic anaemia (one woman) and infection (one man).
Surgical data are shown in table 3.
Surgical data
Women more often received bioprosthetic valves (p<0.001), whereas mechanical valves were more often used in men (p<0.001). The size of prostheses differed significantly (p<0.001).
Operative mortality
Of the 367 patients who underwent surgery 29 (7.9%) died perioperatively (7.3% of women and 8.6% of men; p=0.6). This number was not too far from the predicted mortality rate of 6.5% by the additive EuroSCORE and is the result of a significant number of high-risk patients in whom the additive EuroSCORE is known to underestimates the operative risk. Causes of operative death are shown in table 4.
Causes of death
By multivariable logistic regression, diabetes, age, previous cardiac surgery and renal dysfunction significantly increased operative mortality, whereas gender had no impact on operative death neither in the univariable nor in the multivariable adjusted model (table 5). In addition, the effect of gender was assessed in quintiles of age but again no impact of gender on operative mortality was found in any age quintile.
Logistic regression analysis of ‘operative mortality’, n=367
Late outcome
Follow-up was complete in 99.7% of patients who underwent surgery (n=366). Patients were followed for 3.6±2.2 years (women 3.6±2.2 years vs men 3.7±2.2 years, p=0.792). Thirty-seven late deaths were observed (14 women, 23 men; p=0.2). The causes of late death are given in table 4.
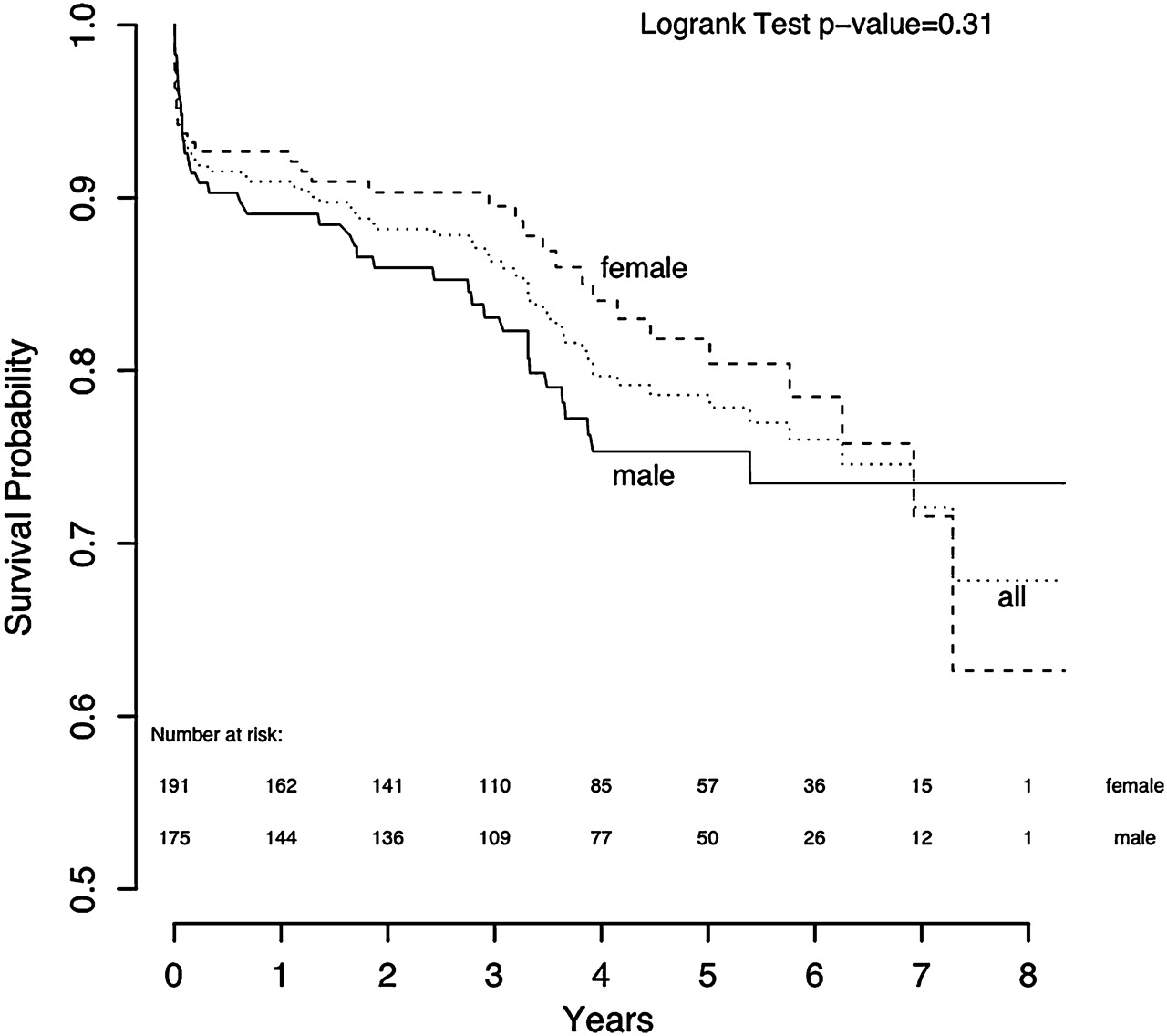
Overall survival by Kaplan–Meier analysis was 91.0%, 88.2% and 78.8% at 1, 2 and 5 years, respectively. Survival of women tended to be slightly better (92.8%, 89.8%, 81.4% vs men 89.1%, 86.6%, 76.3% at 1, 2 and 5 years), however, this difference did not reach statistical significance (p=0.31; figure 1).
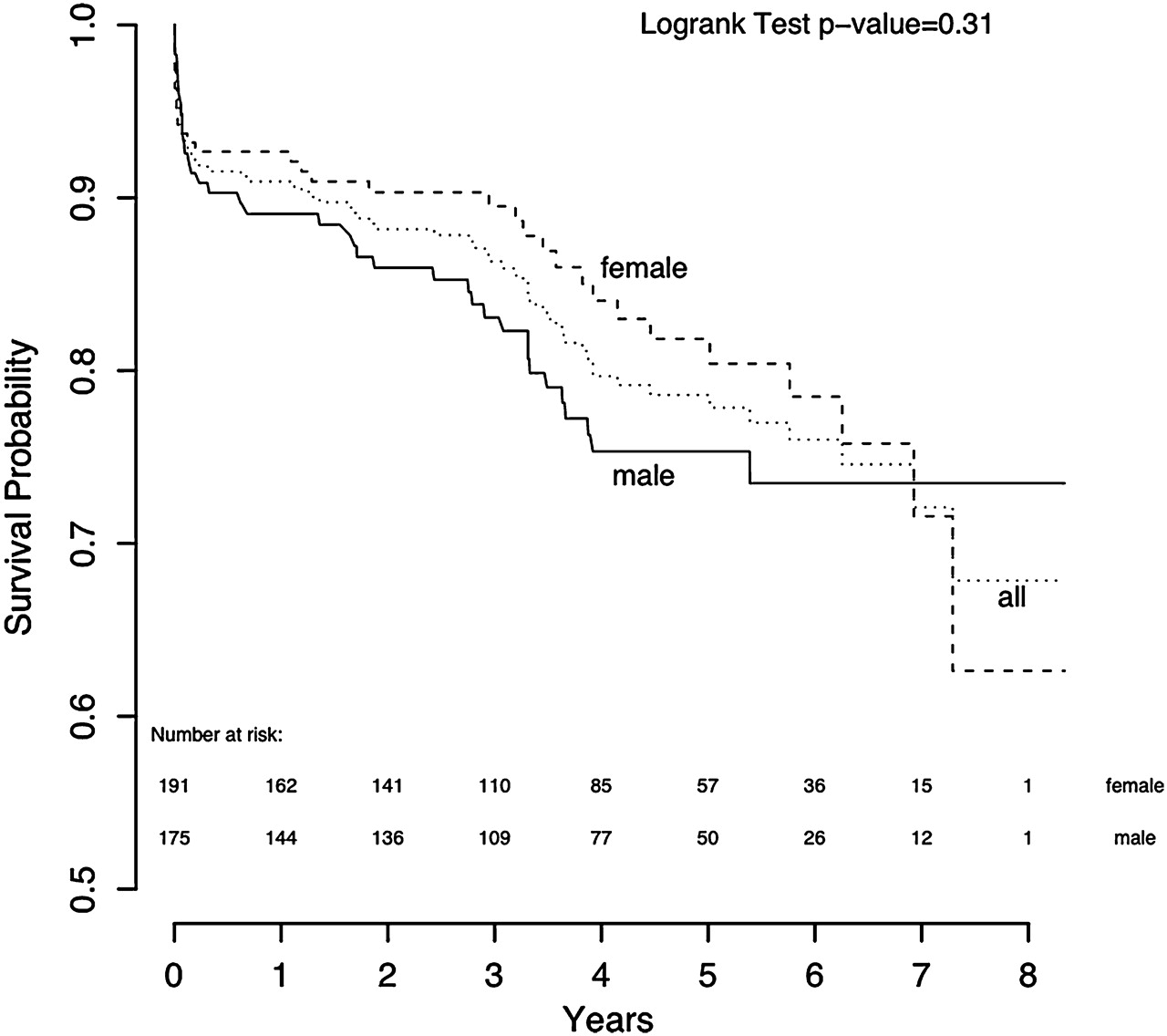
Kaplan–Meier curve for overall survival. Numbers at the bottom indicate the number of patients at each follow-up year.
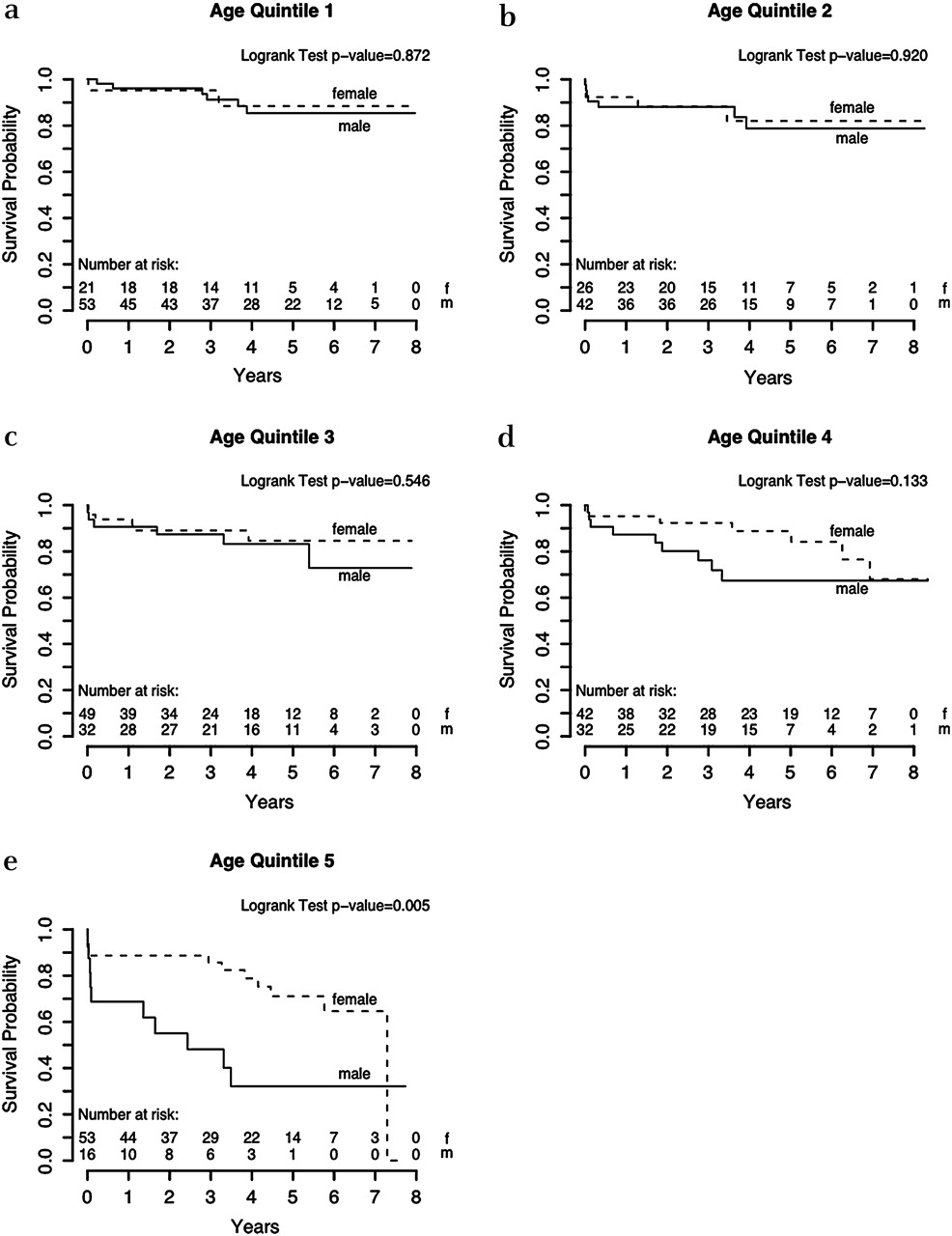
By multivariable analysis, diabetes, age and previous cardiac surgery showed a significant influence on long-term survival. In addition, the analysis indicated a significantly worse outcome of men over the age of 79 years (p=0.04; table 6). In the univariable analysis gender did not influence survival, indicating an interaction between gender and covariables. Therefore, we included the interaction term gender with age into the multivariable analysis, but the effect of gender remained significant (p=0.0462), whereas the interaction term gender with age did not show a significant influence (data not shown). In the next step we included the quadratic interaction term age squared with gender. As a result, gender no longer had a significant impact on survival. But age squared with gender itself now showed a significant influence (p=0.0419). To evaluate these results further, the study population was divided into age quintiles (table 7) and the effect of gender on survival was displayed by Kaplan–Meier curves for each quintile (figure 2 panels a–e). No impact of gender was seen in patients younger than 79 years. However, in the oldest quintile (figure 2 panel e), a worse outcome of men was observed.
Cox proportional hazards regression analysis of ‘long-term mortality’, n=367
Information about age quintiles

{kind=link}
{kind=link}
Panels a–e. Kaplan–Meier curves for each age quintile.
Clinical data at last follow-up
Detailed follow-up data are shown in table 8.
Clinical and echocardiographic data at last follow-up
As compared with preoperative functional status, symptomatic status was still significantly improved at last follow-up. Women, however, remained significantly more symptomatic than men (p<0.002).
Echocardiographic data at last follow-up
In both women and men relative wall thickness significantly decreased postoperatively (table 8). Accordingly, a decrease in septal wall thickness was observed from 16.8±2.7 mm preoperatively to 14.8±2.6 mm (p<0.001) in men and from 15.5±2.6 mm to 13.9±2.3 mm (p<0.001) in women.
Wherease no gender-related difference was observed for relative wall thickness, absolute septal wall thickness remained significantly greater in men (p<0.006).
Discussion
In the present study, female patients undergoing AVR for isolated severe AS presented with unfavourable preoperative characteristics compared with men. Nevertheless, there was no difference between men and women concerning operative as well as late survival. Women, however, remained more symptomatic postoperatively.
Gender differences in presentation of patients with AS
In our study female patients were older and more symptomatic than men at presentation. This is in agreement with previously published data.1–3 5 12 13 The advanced symptomatic status of women has been attributed to more severe left ventricular diastolic dysfunction, a higher prevalence of pulmonary hypertension and older age at presentation. However, two large recent studies of mild/moderate and severe AS14 15 also showed that women were older at study entry, but in contrast to the other studies no difference with regard to time from symptom onset to AVR was found.
Several possible explanations for gender differences in AS patients have been discussed. Recent studies show that AS shares many similarities with atherosclerosis.16–18 As atherosclerosis has a later disease onset in women, probably caused by the protecting effects of oestrogen, similar mechanisms may explain the delayed development of calcific AS. However, the reported observation that calcification of the mitral ring and the aortic valve cusps develops earlier in women does not support this hypothesis.19 20
Part of the observed differences in age at presentation may be explained by the higher prevalence of bicuspid valves in men (women, one; men, three).19 20
Finally, it has been hypothesised that women receive medical attention later than men, either because they wait longer before visiting a doctor or because it takes longer until they are referred to surgery. Both problems have also been discussed for coronary artery disease.21
In the present study the advanced symptomatic status in women at presentation could be explained by more severe stenosis as indicated by higher gradients and smaller estimated valve areas. Similar results have also been observed by Douglas et al4 and Favero et al22 In contrast to previous studies,2 23 24 the present data did not show significant gender differences in left ventricular geometry and hypertrophy after adjusting for body surface area (table 2).
Gender differences in surgical outcome of AS
Mortality
We found no statistically significant difference between men and women younger than 79 years with regard to operative and late mortality. This is particularly surprising because women presented with a worse risk profile, including older age, higher NYHA functional class, higher EuroSCORE and more advanced severity of AS. As a matter of fact, multivariable analysis identified female gender even as an independent predictor of better survival in patients older than 79 years. This finding, however, may be explained by the demographic background of the general population in Austria. Whereas the mean life expectancy of men presently is 77 years, it is 83 years in women.25
Milavetz et al5 also did not find gender-specific differences in short-term and long-term mortality between sexes in their series, whereas data from the Euro Heart Survey13 indicate a tendency towards a better outcome after AVR in women. A recent study by Kulik and coworkers6 also reported better long-term survival of women following bioprosthetic AVR but not after mechanical AVR. In contrast to these reports, Morris et al1 reported a better outcome of men after AVR for severe AS. These results, however, were explained by differences in baseline characteristics contributing to risk. In the multivariable analysis, gender was no independent predictor of survival. Differences in surgical outcome between male and female AS patients in various studies may thus probably be due to differences in risk profile. The demographic background of life expectancy, however, has in none of these studies been taken into consideration.
The EuroSCORE, which is now frequently used for risk assessment of patients undergoing AVR, calculates an increased risk for women. The findings of our study, however, question an increased risk in women per se. The score has been developed and validated for coronary artery bypass surgery. While female gender may increase the risk there, this may not apply to aortic valve replacement.
Morbidity
Postoperatively, women remained significantly more symptomatic than men. This may be due to a greater extent of myocardial fibrosis and diastolic dysfunction due to a more advanced stage of the disease at presentation. Women more frequently had systemic as well as pulmonary hypertension after surgery, probably a sign of the age difference. Finally, mild shortness of breath as a non-specific symptom is not uncommon in the elderly. The finding of more shortness breath could thus also be caused by the higher age of women.
Limitations
The major limitation of the present study is patient selection. The fact that our patients had been referred to an outpatient clinic of a tertiary care centre and that the inclusion criterion was the referral for AVR may have caused selection bias. However, it is unlikely that this will affect the observed gender differences. The results should be valid for a contemporary population undergoing AVR for AS.
Symptomatic status is not easy to evaluate and is certainly influenced by many variables, which may have been a limitation in the present study. However, the cause and extent of physical limitation were carefully assessed by a physician preoperatively and at each follow-up visit.
Conclusions
The present study shows that women who are currently referred for AVR because of severe AS are significantly older, more symptomatic and present with more advanced valve disease compared with men. In addition, women have a higher predicted operative risk by the EuroSCORE and remain more symptomatic after surgery. Nevertheless, women do not appear to have a higher operative mortality or worse late outcome. The even better survival of women in the age group above 79 years may reflect the demographic background, with higher mean life expectancies of women in the general population.
Further research must address whether differences in baseline characteristics are due to differences in disease onset and progression or whether women get delayed medical attention for some reason.
References
Footnotes
Competing interests None.
Ethics approval The Ethics Committee of the Medical University of Vienna approved the study protocol.
Provenance and peer review Not commissioned; externally peer reviewed.