Article Text

Abstract
Objective: To determine whether plasma levels of B-type natriuretic peptide (BNP) predict left ventricular (LV) dysfunction on exercise echocardiography in patients with moderate to severe aortic regurgitation (AR).
Design: Case–control study.
Setting: Outpatient cardiology departments.
Patients: 39 asymptomatic or mildly symptomatic patients with chronic moderate to severe AR and a normal LV ejection fraction (>50%), and 10 normal controls.
Main outcome measures: Plasma level of BNP and echocardiographic measures of LV function at rest and immediately after treadmill exercise.
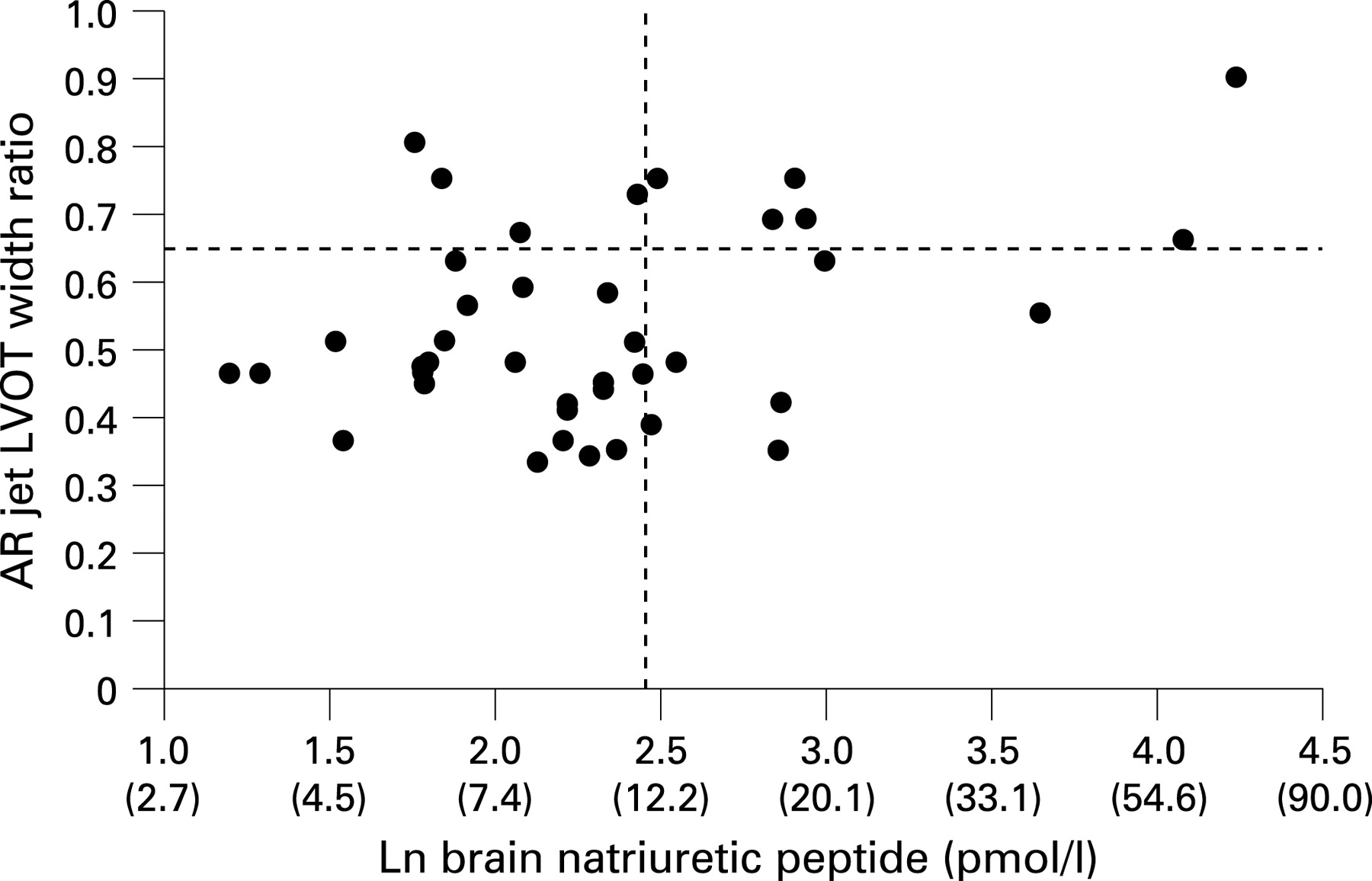
Results: LV end systolic volume index (LVESVI) was significantly increased in AR patients with normal BNP (⩽12 pmol/l) compared with controls (mean (SD) 32 (13) vs 17 (7) ml/m2, p = 0.002) but was similar for AR patients with normal and elevated BNP (38 (16), p = 0.14). In AR patients there was no association between plasma BNP and measures of LV function on echocardiography at rest (r<0.30, p>0.05 for all). However, there were modest but statistically significant associations between the plasma level of BNP and severity of AR indicated by a greater AR:LV outflow tract width ratio (r = 0.37, p = 0.02) and lower diastolic blood pressure (r = −0.44, p = 0.004). Increased BNP was also associated with a greater LVESVI (r = 0.33, p = 0.04) and lower LV longitudinal strain rate (r = −0.037, 0.02) on echocardiography after exercise.
Conclusions: In moderate to severe AR compensatory LV remodelling can occur with no increase in plasma BNP. Increased BNP is associated with more severe regurgitation and changes consistent with early LV dysfunction on exercise echocardiography.
Statistics from Altmetric.com
Asymptomatic patients with chronic aortic regurgitation (AR) can remain clinically stable for years, but many eventually develop symptoms or LV dysfunction. The presence of symptoms, a decrease in LV ejection fraction (<50%) and severe LV dilatation (LV end systolic dimension >50–55 mm) all predict poorer outcomes, and are indications for surgery according to current guidelines.1 2 However, up to a quarter of asymptomatic patients with chronic AR develop LV dysfunction without recognised symptoms,1 and early symptoms can be difficult to evaluate clinically. In addition, detection of early LV dysfunction can be difficult in severe AR because significant LV dilatation and remodelling occur in patients who are clinically well compensated. For these reasons more reliable methods are needed to detect early LV dysfunction in apparently asymptomatic patients with moderate to severe AR.
Brain natriuretic peptide (BNP) is a peptide hormone released from ventricular myocardium in response to increased wall stress.3 Preliminary studies suggest that increased plasma levels of BNP are associated with a greater risk of disease progression and onset of symptoms in initially asymptomatic patients with AR.4 However, it has not been clearly demonstrated that BNP is useful for detecting early LV dysfunction in AR. In a study by Gerber et al, plasma levels of BNP were higher in symptomatic than in asymptomatic patients with aortic regurgitation, but there was no association between BNP and left ventricular volumes or ejection fraction on echocardiography at rest.5
Several studies suggest that exercise stress echocardiography can be used to identify LV dysfunction in patients with chronic AR,6–10 but no previous studies have correlated the presence of early LV dysfunction on stress echocardiography with natriuretic peptide levels. In this study we assess whether raised plasma levels of BNP identify left ventricular dysfunction on exercise stress echocardiography in asymptomatic or mildly symptomatic patients with moderate–severe aortic regurgitation and a normal LV ejection fraction at rest.
METHODS
Study population
Thirty-nine asymptomatic or mildly symptomatic patients with moderate to severe AR and a normal LV ejection fraction (>50%) undergoing follow-up in the outpatient clinic were enrolled in the study between June 2006 and December 2006. AR patients were >18 years old. The AR jet: Left Ventricular Outflow Tract (LVOT) width ratio was >0.3 and holo-diastolic flow reversal in the descending thoracic aorta was present in AR patients. Patients were excluded if there was a history of myocardial infarction, angina or heart failure, LV impairment (ejection fraction <50%), any aortic diameter >5 cm, atrial fibrillation, significant renal disease (creatinine >160 μmol/l), respiratory disease or other valvular heart disease more than mild in severity. Consecutive patients who met these inclusion and exclusion criteria were invited to participate. Ten normal controls of similar age and gender, with no evidence of cardiopulmonary disease or renal disease, were also recruited. The study protocol was approved by the regional ethics committee and all subjects gave written informed consent.
Clinical assessment
Subject details were collected from standardised questionnaires by the study cardiologist at the time of enrolment. A baseline medical history, medication regime, weight, height, pulse and supine blood pressure were obtained. The symptomatic status of each patient was graded according to the New York Heart Association (NYHA) classification system. An ECG was obtained and baseline blood tests for natriuretic peptide levels were taken.
Exercise testing
All subjects underwent a symptom-limited exercise test using an adaptation of the Standard Bruce Protocol, with smaller increments in workload after each minute. Blood pressure was recorded every 2 minutes.11 Exercise was stopped for marked dyspnoea, fatigue, chest discomfort, >2 mm ST depression, significant arrhythmia, on patient request or after completion of 15 minutes of the protocol (15.6 metabolic equivalents (METS)).
Rest and stress echocardiography
Two-dimensional echocardiography was performed using a Vivid 7 Dimension machine (General Electric, Vingmed Ultrasound, Horten, Norway) before and immediately after exercise treadmill testing. At rest, LV dimensions were obtained from the parasternal views according to standard guidelines.12 LV end-systolic and end-diastolic volumes and ejection fraction were measured from the apical four-chamber view using the single-plane modified Simpson’s method,12 which was chosen to allow comparison of pre-exercise and post-exercise LV volumes. All long and short axis LV images were acquired at high frame rates for measurement of 2D speckle tracking based strain, strain rate and LV rotation. Endocardial borders were traced in apical and short axis views and commercial software automatically tracked myocardial motion in six regions of interest. An index of global LV longitudinal strain and strain rate was generated by averaging measurements from all regions of interest in the apical four-chamber view.13 LV torsion measurements were made using a previously described technique.14
LV mass was calculated from linear dimensions using the American Society of Echocardiography recommended formula.12 The left atrial area was measured in apical four-chamber view. Diastolic function was assessed using measurements of transmitral early (E) and late (A) inflow velocities at the mitral valve leaflet tips using a 5 mm sample volume in the apical four-chamber window. Pulsed wave tissue Doppler imaging of the mitral annulus was taken by placing a 5 mm sample volume at the junction of the LV wall and the septal and lateral mitral valve annulus. Care was taken to ensure the smallest possible angle between the ultrasound beam and longitudinal myocardial motion. The septal E/E' ratio was used to give an estimate of LV filling pressure. An intravenous injection of agitated saline was used to enhance the tricuspid regurgitant jet for estimation of right ventricular systolic pressure (RVSP) at rest. Right atrial pressure was estimated from M-mode assessment of the inferior vena cava dimension. Quantitative and qualitative measures of aortic regurgitation severity were made according to American Society of Echocardiography guidelines.15 Measurements of AR jet: LVOT width ratio, AR jet: LVOT area, AR pressure half time, and peak diastolic and end-diastolic flow velocities in the descending thoracic and abdominal aorta were made.
Immediately following peak exercise, echocardiographic images were obtained. Apical four-chamber views were obtained at high frame rates for LV volume calculations, pulsed wave tissue Doppler imaging and 2D speckle tracking based LV longitudinal strain and strain rate measurements. LV torsion measurements could not be reliably obtained after exercise.
Images were stored digitally and analysed offline using a standard GE analysis package (EchoPac PC version 3.0 X GE Medical Milwaukee, WI) by an investigator blinded to clinical and natriuretic peptide data. All echocardiography measurements were averaged from three to five cardiac cycles.
Measurement of natriuretic peptides
Venous blood samples were collected from an indwelling intravenous catheter with the subject supine before exercise. Samples were collected in EDTA tubes, immediately placed on ice and centrifuged within 2 h at −4°C. Plasma was stored at −80°C before being assayed for BNP using an established radioimmunoassay.16 The normal range for BNP is 3–12 pmol/l and the within-assay coefficient of variation is 0.5–2%. To convert BNP measured in pmol/l to pg/ml, divide by 0.289. To convert Nt-BNP measured in pmol/l to pg/ml, divide by 0.462.
Statistical analysis
Correlation coefficients were used to evaluate associations between continuous variables. χ2 tests were used to investigate whether the proportion of NYHA class and AR severity grade differed across groups. Fisher exact tests were used where appropriate. Mann–Whitney U tests were applied to test whether the AR severity measures and exercise echocardiography differed between groups. Analyses of covariance were used to compare across normal control and AR patients with normal and elevated BNP adjusting for age; F test and contrasts were derived for pairwise comparisons. Post hoc Tukey studentised range significant tests (HSD) were also applied in the multi-groups comparisons. Peptide levels underwent natural log transformation due to their right skew distribution in all analyses. Results are presented as means and standard deviations unless otherwise stated. A p value <0.05 was considered statistically significant. SAS institute released SAS 9.1 was used in the analysis.
RESULTS
Baseline characteristics of patients with aortic regurgitation and normal controls
Thirty-nine patients with AR and ten age and sex-matched control subjects were studied. The causes of AR were rheumatic heart disease (18), bicuspid aortic valve (15), connective tissue disease (one), aortic root dilatation (two) and uncertain (two). Patients with AR had a mean age of 42 years (range from 18 to 71 years). Thirty-two patients with AR had NYHA class 1 and seven patients had non-limiting NYHA class 2 symptoms. Twenty-five (64%) AR patients were on an angiotensin converting enzyme inhibitor, five (13%) a calcium channel blocker, and two (5%) a β-blocker. No control patients were taking medication. Compared with control subjects, AR patients had higher systolic (129 (SD 6) vs 112 (SD 9) mm Hg, p = 0.004) and lower diastolic (58 (SD 13) vs 71 (SD 6) mm Hg, p = 0.01) blood pressures at rest, and a higher body mass index (29 (SD 5) vs 24 (SD 3) kg/cm2, p = 0.01). Body surface area was similar in AR patients and control subjects (1.9 (SD 0.3) vs 2.1 (SD 0.2) m2, p = 0.6).
Patients with AR were divided into two groups according to whether they had normal (<12 pmol/l) or elevated BNP (>12 pmol/l) levels as determined by the normal reference range for the assay used.16 Clinical and echocardiographic data are compared for normal controls and patients with AR by plasma BNP in table 1. Associations between the plasma level of BNP and Nt-BNP and echocardiographic measurements at rest and after exercise are presented in table 2.
BNP and severity of aortic regurgitation
Patients with elevated BNP (>12 pmol/l) levels had more severe AR as indicated by a lower diastolic blood pressure and by echocardiographic measures of severity of regurgitation. There were also statistically significant associations between the plasma level of BNP and several echocardiographic measures of AR severity (table 2).
BNP and LV function on echocardiography at rest
Patients with AR had greater left ventricular end-systolic and diastolic volumes and increased left ventricular mass compared with control subjects. However, there was no significant difference in LV dimensions, volumes or mass between AR patients with normal and elevated levels of BNP at rest (table 1). There was also no significant association between the plasma level of BNP or Nt-BNP and other echocardiographically derived measures of systolic function at rest, including tissue Doppler based motion of the lateral mitral annulus (S′), 2D speckle tracking based global longitudinal strain and strain rate, and LV torsion (tables 1 and 2). In contrast, there was an association between the plasma level of BNP and both indexed LA area (r = 0.53, p = 0.001) and pulmonary artery pressure (PAP) at rest (r = 0.39, p = 0.02), even though few AR patients had elevated PAP and mean values were not significantly higher than in control subjects (25 (SD 4) vs 28 (SD 7) mm Hg, p = 0.1).
BNP, exercise capacity and symptoms
Patients with AR had a lower exercise capacity (METS) than control subjects, but there was no significant difference between AR patients with normal and elevated levels of BNP. AR patients with BNP>12 pmol/l were, however, more likely to have NYHA class 2 symptoms than patients with BNP ⩽12 pmol/l (36% versus 11%, p = 0.06).
BNP and LV function on echocardiography after exercise
Compared with AR patients with a normal BNP level, those with BNP >12 pmol/l had higher indexed LV end-systolic (p = 0.09) and diastolic volumes (p = 0.05) and a smaller percentage decrease in LVESVI (p = 0.03) and LVEDVI (p = 0.03) on echocardiography performed immediately after treadmill exercise (table 1). There was a statistically significant association (p<0.05) between age and both LV end-systolic volume index (LVESVI) and LV end-diastolic volume index (LVEDVI). After adjustment for age, p was <0.01 for post-exercise LVESVI, % change in LVESVI, LVEDVI, and % change in LVEDVI. All other results were similar with and without adjustment for age. A lower longitudinal global strain rate (p = 0.05) and change in strain rate (p = 0.02) were seen after exercise. However, there was no significant difference in lateral S′ or global longitudinal strain between groups after exercise. Peak heart rate and systolic blood pressure were not significantly different between the two AR groups. There were moderate and statistically significant correlations between each of these post exercise measures of LV function and the plasma level of BNP (table 2). The area under the receiver operator characteristics curve (AUC) for a post exercise LVESVI >24 mls/m2 (upper quartile) was modest (0.64 (p = 0.08)). After adjustment for age the AUC increased to 0.78 (age, p = 0.05; BNP, p = 0.02).
N-terminal pro-B type natriuretic peptide in AR
Selected echocardiographic measures of severity of AR and myocardial function at rest and after exercise are presented for patients with Nt-BNP below and above 35 pmol/l in table 3, and correlation coefficients are presented together with BNP in table 2. Results of all analyses were similar for BNP and Nt-BNP. However, the differences in LVESVI, LVEDVI and LV mass index measured at rest between AR patients with a plasma level of Nt-BNP greater than 35 pmol/l and those with a level lower than 35 pmol/l were statistically significant (p<0.05). The predictive value of Nt-BNP for a post-exercise LVESVI >24 mls/m2 (upper quartile) was 0.65 (p = 0.08) before, and 0.81 (p = 0.01) after, adjustment for age.
DISCUSSION
In this study most patients with moderate to severe AR had evidence of substantial LV remodelling with an increase in LV mass and LV end-systolic and diastolic volumes compared with normal controls. Despite this, the plasma level of BNP was within the normal range for many AR patients. An increase in the plasma level of BNP or Nt-BNP was associated with more severe regurgitation at rest, as well as increased LV end-systolic and end-diastolic volumes and decreased longitudinal strain rate on echocardiography performed immediately after treadmill exercise. These observations suggest that measurement of BNP or Nt-BNP may identify early LV dysfunction in patients with severe AR which may not be evident on resting echocardiography alone.
The decision to proceed to valve replacement in aortic regurgitation is usually made on clinical evidence of cardiac decompensation, suggested by onset of symptoms or a decrease in LV ejection fraction. Significant LV dysfunction may occur before a clear reduction in ejection fraction is detected. In addition, symptom onset can be difficult to determine in a chronic disease which progresses slowly. Although many studies have demonstrated that a raised plasma level of BNP or Nt-BNP is a powerful predictor of adverse outcomes in a broad range of cardiac disease, few studies have systematically assessed the factors which influence BNP levels in patients with AR, and there is limited information on whether measurement of BNP provides prognostic information additional to clinical assessment and resting echocardiography.
Weber et al evaluated the relationship between Nt-BNP levels and the progression of disease in 37 patients with chronic aortic regurgitation and an EF >45% undergoing clinical follow-up.4 They demonstrated a strong correlation between AR severity and Nt-BNP levels, and a significant reduction in Nt-BNP levels after valve surgery. Similarly, Eimer et al, in a small pilot study involving 12 patients with AR, also demonstrated a relationship between BNP levels and AR severity.17 The majority of patients in both these studies had mild–moderate AR. The current study demonstrated a correlation between BNP levels and several echocardiographic measures of AR severity in patients with at least moderate–severe AR.
Gerber et al5 evaluated 40 patients with chronic AR from outpatient clinics and those meeting criteria for valve surgery. In this population of patients with markedly dilated ventricles, there was no correlation between BNP levels and LV dimensions and volumes at rest. Similarly, we demonstrated that significant compensatory LV remodelling can occur in asymptomatic AR patients with normal BNP levels. Although the study by Gerber et al demonstrated higher BNP levels in symptomatic patients with AR, no study has assessed the relationship between levels of BNP and exercise treadmill capacity. Previous studies suggest that reporting of symptoms does not necessarily correlate with exercise capacity.18 Exercise capacity can be influenced by factors other than cardiac function, and there can be considerable individual variation in physical fitness. For this reason a direct measure of early LV dysfunction may be preferred.
Prognostic studies have demonstrated worse outcome in AR patients with an impaired haemodynamic response to exercise.6 19 In the current study, patients with elevated BNP levels had several echocardiographic measures suggesting LV dysfunction immediately after exercise. AR patients with elevated BNP had higher LV end-systolic and diastolic volume index and a trend to lower post-exercise ejection fraction than AR patients with normal BNP levels. However, the predictive value of both BNP and Nt-BNP for post-exercise LV dysfunction on echocardiography was modest. Further research will be needed to determine whether BNP/Nt-BNP has prognostic value better than or additional to exercise stress echocardiography.
Strain rate is a less load-dependent marker of myocardial contractility,20 which has been associated with subclinical myocardial dysfunction and poorer post-operative outcome in patients with organic mitral regurgitation.21 In the current study, patients with elevated BNP levels had lower global longitudinal strain rate and change in strain rate after exercise. Two previous studies have investigated the role of long axis contraction (S′) in asymptomatic patients with AR.22 23 The presence of an S′ velocity of the mitral annulus <9 cm/sec has been associated with poorer exercise tolerance and a higher LV end-diastolic pressure and end-diastolic wall stress on cardiac catheterisation. However, there was no significant association between S′ velocity at rest or post-exercise and the plasma level of BNP in this study.
Study limitations
The number of patients studied was modest. However, it is unlikely that the association between BNP/Nt-BNP and post-exercise LV dysfunction was due to chance alone, because there were statistically significant associations between several post-exercise measures of LV dysfunction and both BNP and Nt-BNP. On average patients were younger than in some previous reports. This may reflect the larger proportion of patients with rheumatic heart disease who have AR at an earlier age. Plasma levels of natriuretic peptides increase with age,24 25 but after adjustment for age the associations between BNP/Nt-BNP and post-exercise LV function were stronger, and other associations were similar. The study was too small to allow meaningful subgroup analyses, for example of patients with no and mild symptoms. For asymptomatic patients with normal LV function the rate of progression to symptoms or overt LV dysfunction is on average about 6% per year.1 A much larger study with long-term follow-up is therefore needed to determine whether BNP can reliably predict outcomes.
Conclusion
This study suggests that AR patients with elevated BNP levels are more likely to have early LV dysfunction after exercise, but the clinical significance of these changes is currently uncertain. A large prospective study is needed to determine whether including serial measurements of BNP or Nt-BNP during follow-up improves the ability to detect early LV dysfunction and thereby allows more optimal timing of aortic valve replacement.

{kind=link}
{kind=link}
Acknowledgments
We are grateful to Diane Caveney and Jenny White for management of the study, to our echocardiography sonographers, Margaret Oldfield, Shawn O’Leary and Marcus Silbury, and to Barbara Semb, Research Secretary, Green Lane Research and Education Fund, for secretarial assistance.
REFERENCES
Footnotes
Competing interests: None.
Funding: This study was supported by a grant from the National Heart Foundation of New Zealand.