Article Text

Abstract
Background: Population studies have shown that increased large artery stiffness is an independent predictor of cardiovascular events. Experimental studies have shown that a stiff aorta is associated with decreased coronary blood flow. However, a link between large artery stiffness and coronary microvascular function in the clinical setting has not been demonstrated previously.
Objective: To evaluate the relationship between large artery stiffness and coronary flow velocity reserve (CFVR).
Patients and methods: 102 consecutive subjects (mean (SD) age 62 (10) years) without coronary and peripheral arterial disease were enrolled in the study. After 15 minutes’ rest, measurements were obtained of brachial-ankle pulse wave velocity (baPWV), augmentation index (AIx) from a carotid pulse tracing, and transthoracic echocardiographic measures, including coronary flow velocity in the left anterior descending coronary artery. In addition, coronary flow velocity during hyperaemia was measured during an intravenous infusion of adenosine triphosphate. CFVR was defined as the ratio of hyperaemic to basal coronary velocity.
Results: Subjects with decreased CFVR (<2.5; n = 40) had significantly higher baPWV (1848 (369) cm/s vs 1548 (333) cm/s; p<0.001), greater AIx (25.3 (11.0)% vs 16.3 (20.0)%; p = 0.01) and greater pulse pressure (PP) (64 (13) mm Hg vs 54 (13) mm Hg; p<0.001) than those with normal CFVR (⩾2.5; n = 62). Multivariate analysis showed that AIx and PP were independent predictors of CFVR (r = −0.32, p<0.001 and −0.25, p = 0.02, respectively).
Conclusions: The data suggest that large artery stiffening is linked to a reduction of CFVR, which may partially explain the higher cardiac event rate in patients with increased large artery stiffness.
Statistics from Altmetric.com
Several studies have suggested that large artery stiffness may predict cardiovascular morbidity or mortality1 and coronary atherosclerosis2 in the general population. The Conduit Artery Functional Evaluation (CAFE) study, a large substudy within the Anglo-Scandinavian Cardiac Outcomes Trial (ASCOT), showed that central pulse pressure (PP) was associated with major cardiovascular outcomes in a large cohort of patients.3 Therefore, large artery stiffness is an important cardiovascular risk factor in the general population. It is well known that the aortic pressure waveform is determined not only by cardiac output and peripheral vascular resistance but also by the stiffness of conduit arteries and the timing and magnitude of pressure wave reflections.4 That is, in a normal elastic aorta, the pressure wave reflects from the periphery and returns to the heart during diastole. This reflected wave helps augment diastolic aortic pressure; and since coronary perfusion occurs mainly during diastole, this may improve coronary blood flow. As the aorta stiffens, the velocity of the pressure wave increases, and the reflected pressure wave eventually reaches the heart during systole rather than diastole. This causes augmentation of systolic blood pressure and consequently, increased cardiac after load and myocardial oxygen demand. In addition, the diminished elasticity of the stiff aorta, combined with the absence of diastolic augmentation from the reflected pressure wave, has the potential to reduce coronary perfusion pressure and coronary blood flow.
Experimental studies have shown that coronary artery blood flow varies with aortic stiffness.5 6 Kingwell et al demonstrated that measures of large artery stiffness were correlated with the time to ischaemic ST-segment changes during a treadmill stress test in patients with coronary artery disease.7 Thus, coronary perfusion reserve might be influenced by large artery stiffness. However, there have been few studies in the clinical setting to support this theory. Accordingly, we sought to examine the relationship between the elastic properties of arterial stiffness and coronary flow velocity reserve (CFVR).
SUBJECTS AND METHODS
Study group
One hundred and seven asymptomatic consecutive subjects who were not receiving any drugs and who were found to have hypertension, hyperlipidaemia or diabetes on a periodic group examination were referred to our hospital for further evaluation. All subjects were enrolled in the present study between April 2005 and September 2006. If subjects had an electrocardiographic abnormality, a treadmill exercise test was performed; and if ischaemic changes were observed, further myocardial scintigraphy was done to rule out coronary artery disease. The diagnosis of hypertension was determined based on blood pressure levels measured at the time of the pulse wave analysis (systolic blood pressure ⩾140 mm Hg or diastolic blood pressure ⩾90 mm Hg, or both). Diabetes was considered present if a subject had a fasting glucose level >6.9 mmol/l.
Exclusion criteria included significant ischaemic heart disease, valvular heart disease, ejection fraction ⩽60% as assessed by echocardiography, known history of bronchial asthma, atrial fibrillation, other conduction disturbances or significant peripheral vascular disease (ankle to brachial blood pressure ratio ⩽0.9). Treadmill testing was performed in five subjects who had an electrocardiographic abnormality at rest. In three subjects with a positive stress test, myocardial perfusion scintigraphy was performed and one patient was diagnosed with coronary artery disease; another subject had an ankle to brachial blood pressure ratio of 0.85. Therefore, these two subjects were excluded and the final study group comprised 105 subjects. The study was approved by the ethics committee of Ehime University Graduate School of Medicine, and all subjects gave informed consent before participation.
Pulse wave analysis
Subjects were examined in the morning (08:30–09:00) after a 12-hour overnight fast in a quiet, temperature-controlled laboratory (22°C) after 15 minutes of lying supine. The brachial–ankle pulse wave velocity (baPWV) was measured using the volume-plethysmographic method with previously validated equipment (form PWV/ABI; Colin Medical Technology, Komaki, Japan). A detailed description of this device has been reported previously.8 9 Cuffs were connected to both the plethysmographic and oscillometric sensors and wrapped around both arms and ankles while the patient was supine. Transit time (δTba) between the brachial and ankle pulse waves was automatically measured based on the time delay between the foot of the pressure increase (sharp initial systolic upstroke of the wave) in the arm and ankle. The distance between the two recording sites was calculated automatically based on the height of the subject (H) and anthropomorphic data for the Japanese population. The path length from the suprasternal notch to the brachium (Lb) and ankle (La) was calculated using the following equation: Lb = 0.2195 × H (cm) −2.0734, La = 0.8129 × H (cm) +12.328. The baPWV was then calculated using the following equation: baPWV = (La − Lb)/δTba. The average of the right and left baPWV was used in the final analysis. Although the brachial and ankle blood pressure can be measured simultaneously using this oscillometric method, we used only the brachial blood pressure in this study.
Measurement of the carotid augmentation index (AIx) was performed using a multielement applanation tonometry sensor for the left common carotid artery.10 11 This sensor consists of 15 pressure-sensitive small elements aligned side by side. The sensor element, which is manually located at the centre of the carotid artery, can identify the carotid pulse tracing. The reliability of this tonometry sensor has been reported previously.10 11 The AIx was defined as the increment in pressure from the first systolic shoulder (inflection point) to the peak pressure of the aortic pressure waveform expressed as a percentage of the peak pressure.12 All measurements were carried out by the same trained investigator.
Echocardiographic examination
Immediately after measurement of the arterial stiffness variables, echocardiographic examinations were performed using either a Sequoia 512 (Siemens Medical Solutions USA, Inc, Ultrasound Division, Mountain View, CA, USA) or Vivid 7 Dimension ultrasound machine (GE Healthcare, Milwaukee, WI, USA). Conventional M-mode, two-dimensional and Doppler echocardiograms of the inflow tract of the left ventricle were recorded. The left ventricular internal dimension and wall thickness were measured at end diastole and end systole according to the recommendations of the American Society of Echocardiography.13 The left ventricular mass was calculated by the equation of Devereux et al14 and normalised to body surface area (left ventricular mass index (LVMI)).
Coronary flow velocity (CFV) was measured as previously described.15–17 In brief, subjects were examined in the left lateral decubitus position. A modified apical view was obtained from the fourth or fifth intercostal space between the mid-clavicular and parasternal views. Colour Doppler imaging was performed at 3.5 or 5 MHz with a velocity range of ±10.0 cm/s or ±12.0 cm/s. Pulse wave Doppler flow in the distal left anterior descending artery (LAD) was recorded with the guidance of colour Doppler scan flow mapping. An effort was made to set the θ angle as small as possible. The changes in CFV were measured at rest and during hyperaemia produced by intravenous adenosine triphosphate administration (0.14 mg/kg/min over 3 minutes). Echo contrast (Levovist, Schering, Germany; at concentration of 300 mg/ml) was used to improve the quality of the Doppler envelope in 50/105 subjects (48%) according to the echocardiographer’s judgment, as previously described.15 An experienced echocardiographer, who was unaware of each patient’s data, manually contoured the CFV profile. With the analysis programme provided on the ultrasound system, the averaged diastolic peak velocity was determined from three cardiac cycles at both baseline and peak hyperaemic conditions and averaged. CFVR was defined as the ratio of hyperaemic to basal CFV.
Coronary microvascular dysfunction was defined as a CFVR of <2.5, which is the lower limit of normal flow reserve in arteries free from significant obstructive coronary artery disease.18 19
Measurement of metabolic variables
Total cholesterol, triglycerides, high-density lipoprotein cholesterol, low-density lipoprotein cholesterol and fasting blood glucose levels were measured by enzymatic methods. All blood samples were obtained on the morning of the study.
Statistical analysis
Data are expressed as the mean (SD). Differences in distributions of factors between the groups were assessed using unpaired t tests for numerical values, and χ2 tests or Fisher exact tests for categorical values. Univariate analysis was performed on the clinical data, metabolic variables, and echocardiographic and arterial stiffness variables for determination of significant predictors of CFVR. Stepwise multivariate regression analysis was performed for determination of independent predictors of CFVR. The interobserver and intraobserver variabilities were assessed for coronary velocity measurements in 15 recordings in seven randomly selected patients. The interobserver variability was calculated as the SD of the differences between the measurements of two independent observers, who were unaware of the other patient data, expressed as a percentage of the average value. The intraobserver variability was calculated as the SD of the differences between the first and second determination (3-week interval) for a single observer and expressed as a percentage of the average value. All statistical analyses were performed using SPSS 11.0.1J software for Windows (SPSS Inc, Chicago, Illinois, USA). Values of p<0.05 were considered significant.
RESULTS
CFVR could not be measured in three of 105 subjects because of technical difficulties; thus, CVFR was analysed in the remaining 102 subjects. Table 1 presents the baseline characteristics of the subjects.
Comparison of study subjects with and without coronary microvascular dysfunction
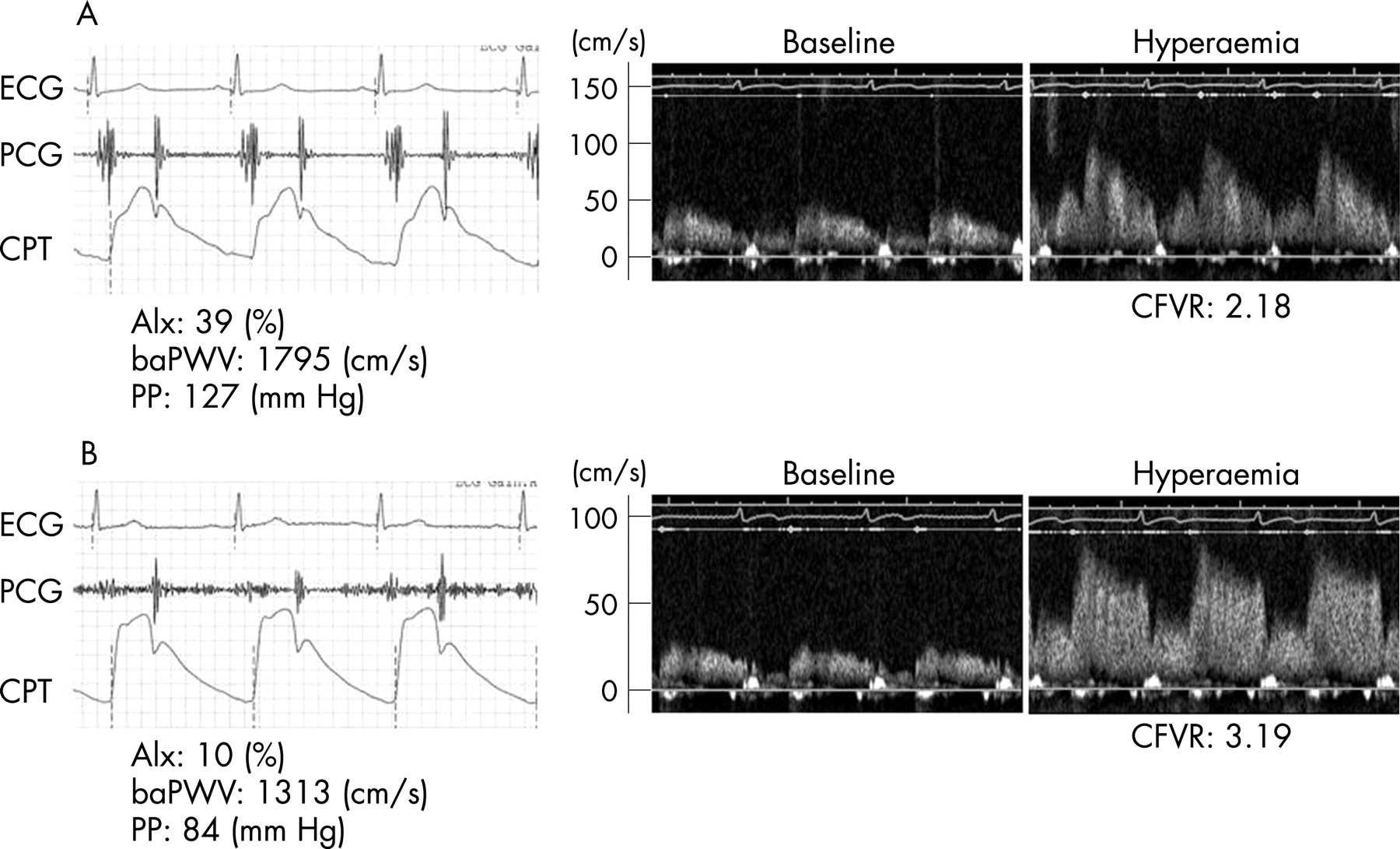
Figure 1 shows representative cases of subjects with and without coronary microvascular dysfunction. Table 2 shows the clinical characteristics of the study subjects with and without coronary microvascular dysfunction. There was no significant difference in risk factors between the two groups except for the proportion of current smokers and metabolic variables. Subjects with decreased CFVR (<2.5) had significantly higher systolic blood pressure, rate–pressure product and PP than those with normal CFVR (⩾2.5). Subjects with coronary microvascular dysfunction had significantly higher baPWV and greater AIx than those with normal microvascular function.
{kind=link}
Correlation between CFVR and study characteristics
In the entire study group, an inverse correlation was noted between CFVR and age (r = −0.41; p<0.001), mean blood pressure (r = −0.34; p<0.001), PP (r = −0.43; p<0.001), rate–pressure product (r = −0.37; p<0.001), LVMI (r = −0.24; p = 0.02), baPWV (r = −0.46; p<0.001) and AIx (r = −0.41; p<0.001). Multivariate analysis was performed to detect independent predictors of CFVR among age, gender, body mass index, fasting blood glucose, low-density lipoprotein cholesterol, current smoker, mean blood pressure, PP, rate–pressure product, LVMI, E/A, baPWV and AIx. Among these variables, AIx, PP and fasting blood glucose were significant independent predictors of CFVR (r = −0.32, p<0.001, r = −0.25, p = 0.02 and r = −0.18, p = 0.03, respectively). The baPWV showed a tendency to be a significant predictor (r = −0.20, p = 0.063) (table 3).
Observer variabilities
The interobserver and intraobserver variabilities for the measurement of Doppler velocity recordings were 4.7% and 3.9%, respectively.
DISCUSSION
The major finding of this study was that large artery stiffening was linked to a reduction of CFVR, even after adjustment for age, metabolic variables, rate–pressure product and LVMI, which are known to affect CFVR.18 This result suggests that arterial stiffness is an important factor to predict CFVR, which might partially explain the relationship between large artery stiffness and cardiovascular morbidity or mortality.
Relationship between arterial stiffness, coronary flow and CFVR
In an experimental study, a decrease in aortic compliance with aortic banding caused subendocardial ischaemia.5 Ohtsuka et al demonstrated that a canine model of decreased aortic distensibility contributed to a decrease in coronary flow reserve even in the absence of coronary artery stenosis.6 However, there is little information about the relationship between coronary flow and arterial stiffness in humans. Recently, Leung et al demonstrated a correlation between a reduction of CFVR and a decrease of central PWV and PP during percutaneous coronary intervention in patients with coronary artery disease.20 Fukuda et al reported a correlation between baPWV and CFVR with a Doppler guide wire in patients with coronary artery disease.21
Our finding that large artery stiffness is associated with CFVR is consistent with these previous studies. However, multiple regression analysis in our study showed that the AIx and PP were significantly related to CFVR, whereas baPWV was not. Several possible explanations may account for these differences. First, the former study did not evaluate AIx and the latter study did not evaluate AIx and PP, whereas we included both AIx and PP as independent variables in our multivariate analysis. Thus, possibly, the statistical power of baPWV to predict CFVR was lowered because of the similar nature of these three variables. Second, ageing does not appear to have the same effect on AIx and PWV. The Anglo-Cardiff Collaborative Trial has shown that AIx is a more sensitive marker of arterial stiffening in younger subjects, whereas PWV is a better marker in older subjects.22 Moreover, it has been reported that baPWV is significantly higher in subjects with coronary artery disease than in those without.8 Thus, if our study group included older subjects or subjects with definite coronary atherosclerosis, it is possible that baPWV might have been a stronger independent predictor of CFVR. Third, the effect of glyceryl trinitrate administration on compliance of the systemic arteries during a catheter procedure cannot be ignored.4
Other mechanisms of reduced CFVR in large artery stiffening
It is well known that CFVR is affected by both epicardial stenosis and microvascular function.18 CFVR is decreased when there is >50% luminal stenosis and is used to judge ischaemia and the need for percutaneous coronary intervention.18 Hypertension, diabetes mellitus, hypercholesterolaemia or a smoking habit are known to cause deterioration of collagen and elastin in the vascular wall,4 resulting in a gradual stiffening of the vasculature. CFVR is also decreased in subjects without coronary artery stenosis, but with such traditional atherosclerotic risk factors.18 Reduced CFVR in these pathological conditions is thought to be associated with endothelial dysfunction, resulting in diminished nitric oxide production.23 Indeed, CFVR obtained by the same method as in our study has been demonstrated to be changed by conditions such as hypertension,24 diabetes mellitus,25 lipid loading26 statin therapy,27 or passive smoking.28 Recently, McEniery et al reported a correlation between endothelial function in the systemic and brachial arteries and PP, PWV and AIx.29 Taken together with our results, it would appear that endothelial function is changed not only in systemic arteries but also in coronary arteries in subjects with a stiff aorta.
Clinical implications
Non-invasive measurement of AIx and PP may be a possible surrogate for coronary microvascular dysfunction. Arterial stiffness has been shown to be reduced by antihypertensive agents, statins, thiazolidinediones and lifestyle modification.4 Improvement of angina status by long-term medical treatment may be partially responsible for improvement of CFVR as indicated by arterial stiffness and endothelial dysfunction.30
Study limitations
The present study has several limitations. First, we have not completely excluded subclinical coronary artery disease because coronary angiography was not performed. Thus, to confirm our observations, we analysed CFVR data in 50 additional subjects matched for age, gender and clinical background with the 102 subjects. These 50 additional subjects underwent coronary angiography because of atypical chest pain but had normal coronary arteries. There was no significant difference between CFVR in these 50 subjects (mean (SD) 2.77 (0.69); range 1.79–4.60) and in the 102 subjects (2.76 (0.67); range 1.79–4.56; p = 0.93). Therefore, we think that it is unlikely that subclinical coronary artery disease affected CFVR in this study. Second, we did not measure central AIx or central blood pressure. Therefore, although the peripheral AIx and PP showed a close association with CFVR, we could not determine whether central AIx or central PP would better correlate with CFVR. Third, there are limitations in the method we used to measure baPWV. We assessed vessel path length by an equation, although unfolding of the aorta with increasing age may make such an approximation less reliable. Lastly, subjects in this study did not have definite atherosclerotic disease, but had risk factors for atherosclerosis. A large, population-based study is required to confirm the validity of our results.
CONCLUSIONS
We demonstrated that an increase in arterial stiffness is associated with decreased CFVR. Our findings provide in vivo physiological data to support the epidemiological observations that arterial stiffness is an important and independent prognostic marker for cardiovascular events.
Acknowledgments
We appreciate the help of Dr Toshihiko Morikawa (Department of Biostatistics, Kurume University Graduate School of Medicine) with the statistical analysis.
REFERENCES
Footnotes
Competing interests: None.
Ethics approval: From the ethics committee of Ehime University Graduate School of Medicine, Toon, Japan.