Article Text

Abstract
OBJECTIVE To evaluate the application of guidelines in the decision making process leading to medical or surgical treatment for aortic stenosis in elderly patients.
DESIGN Cohort analysis based on a prospective inclusive registry.
SETTING 205 consecutive patients (⩾ 70 years) with clinically relevant isolated aortic stenosis and without serious comorbidity, seen for the first time in the Doppler-echocardiographic laboratories of three university hospitals in the Netherlands.
RESULTS The initial choice was surgery in 94 patients and medical treatment in 111. Only 59% of the patients who should have had valve replacement according to the practice guidelines were actually offered surgical treatment. These were mainly symptomatic patients under 80 years of age with a high gradient. Operative mortality (30 days) was only 2%. The three year survival was 80% in the surgical group (17 deaths among 94 patients) and 49% in the medical group (43/111). Multivariate analysis showed that only patients with a high baseline risk, mainly determined by impaired left ventricular function, had a significantly better three year survival with surgical treatment than with medical treatment.
CONCLUSIONS In daily practice, elderly patients with clinically relevant symptomatic aortic stenosis are often denied surgical treatment. This study indicates that a surgical approach, especially where there is impaired systolic left ventricular function, is associated with better survival.
- aortic stenosis
- elderly people
- clinical decision making
Statistics from Altmetric.com
The most frequent valvar lesion in elderly people is degenerative calcified aortic stenosis, with a prevalence of 2.5% at the age of 75 years and almost 8% at 85 years.1 More than 9% of the Western population is now over 70 years of age. As the proportion of elderly people is still rising, aortic stenosis is becoming an increasingly important health problem.
Aortic valve replacement for aortic stenosis in the elderly can be performed with an acceptable operative mortality and morbidity and with good long term results.2-9 However, the writers of these reports did not consider patients who did not have surgery, and they did not measure the difference in outcome between surgical and medical treatment. We studied a cohort of elderly patients with clinically relevant aortic stenosis on Doppler echocardiography and without major comorbidity to determine the following: the clinical characteristics that determine the choice of surgical treatment in elderly patients with clinically relevant aortic stenosis; mortality in the medical and surgical treatment group; and possible differences in the long term survival of surgically and medically treated patients after adjustment for baseline risks. To our knowledge, our cohort study is the first to examine the decision making process leading to medical or surgical treatment as well as the outcome of treatment.
Methods
We studied the records of 280 consecutive patients aged 70 years or older, in whom a diagnosis of clinically relevant aortic stenosis was made for the first time by Doppler echocardiography. The patients were diagnosed in three university hospitals (Amsterdam, Groningen, and Maastricht) in the Netherlands between January 1991 and December 1993. All had cross sectional and Doppler echocardiography. Isolated aortic stenosis was defined as an aortic valve area of ⩽ 1.0 cm2 or a maximum gradient of ⩾ 50 mm Hg and a maximum aortic regurgitation of grade II of IV as assessed by Doppler echocardiography.10 Patients with serious concomitant valvar disease, for example mitral regurgitation exceeding grade 2, were not included.
Seventy five patients were excluded: nine (3%) refused aortic valve replacement and 45 (16%) had major non-cardiac comorbidity according to Greenfield’s definition.11 Three patients (1%) lived in a nursing home. Eight patients (3%) with very poor cardiac status at the time of echocardiography, in whom surgical treatment was not a realistic option, were excluded; these were mainly patients with extensive acute myocardial infarction. The medical records of 10 patients (4%) could not be traced. Ultimately, the records of 205 patients were analysed. Follow up was achieved in 202 patients (99%). Two patients moved abroad and were censored at the date of the last contact. Follow up ended in May 1995. In patients who died, relevant data about the death were obtained from the municipal office (99% complete). Information about functional class and Rankin score12 were collected from the general practitioner (98% complete).
We collected the clinical characteristics and sociodemographic data—such as sex, age, and place of residence (independent, home for the elderly, or nursing home)—at the time of the Doppler echocardiography. Clinical symptoms included angina pectoris, dyspnoea (according to New York Heart Association (NYHA) grade), syncope, history of myocardial infarction (enzyme levels, ECG), and cardiac surgery.
We used the following criteria. Congestive heart failure was present if pulmonary oedema or pulmonary vascular congestion was diagnosed by auscultation or radiographically at the time of echocardiography. ECG data included atrial fibrillation and left ventricular hypertrophy.13 Left ventricular function was qualitatively assessed from the cross sectional echo image and defined as “good” or “impaired,” that is, asynergy of two or more segments or ejection fraction below 45%.14 ,15 The maximum and the mean instantaneous gradients across the aortic valve were determined by continuous wave Doppler echocardiography with multiple acoustic windows.16 ,17 Aortic regurgitation was determined by colour Doppler flow imaging.18 We also collected information about valve replacement and, if recorded, the arguments leading to the decision to operate or to treat medically.
In all surgical procedures, cardioplegia was achieved by antegrade perfusion of the coronary arteries with St Thomas’ Hospital solution. After excision of the aortic valve and, if necessary, careful annular debridement of calcium, the largest prosthesis that could be fitted was implanted.
All patients with a mechanical prosthesis received life long anticoagulant treatment (target international normalised ratio 3 to 4.5). After the operation, the patients with a bioprosthesis received anticoagulation for three months, or longer if there was a special indication, for example atrial fibrillation.
Concomitant coronary artery bypass grafting was performed if significant lesions (⩾ 50%) were present in the major branches. Patients who were not operated on were treated medically with diuretics and digoxin.
The attending cardiologist decided whether or not a patient was eligible for aortic valve replacement. The ultimate decision was made during one of the weekly cardiovascular surgical meetings. Patients were considered to have been treated surgically when the decision to replace the aortic valve was taken within 180 days of the echocardiography. The day of the decision was considered to be the start of follow up. Thus patients who died while on the waiting list remained in the surgical group according to the intention to treat principle. All other patients were considered as being treated medically. The survival time in these medically treated patients started 11 days after echocardiography, which was the median time from the Doppler echocardiography to the day of the decision to perform aortic valve replacement in the surgical group.
The determinants of the decision to treat patients surgically or not were identified by assessing the relation of the clinical characteristics at the time of echocardiography to that decision. The primary end point was all cause mortality during follow up.
STATISTICS
Continuous variables are reported as means and ranges; χ2 analysis was used in the univariate analysis of determinants of valve replacement. Cumulative survival was estimated by the Kaplan–Meier method. Patients were censored if they were alive at the end of follow up. Survival analysis was performed by Cox proportional hazard analysis. Differences in survival were determined by the log-rank test.
Using Cox proportional hazard analysis we identified univariately the risk factors of mortality during follow up in all medically treated patients. Then we constructed, step by step, a multivariate Cox proportional hazard risk model. The main baseline characteristics—such as the severity of the aortic stenosis, left ventricular function, and previous myocardial infarction—entered the model and remained in the model if the level of significance was below 0.20. On biological grounds, age and sex were forced in the model. With the multivariate risk model developed in the medically treated patients, we calculated individual risk scores for each patient, including the surgically treated patients. Thereafter, they were ranked in three groups with a low risk score, an intermediate score, and a high individual risk score. We used this risk score in a stratified analysis and compared the mortality between surgically and medically treated patients, thereby adjusting for unequal distributions of baseline risk between the treatment groups.
Database structuring and data analysis were done in SAS statistical software.19
Results
BASELINE CHARACTERISTICS
The study population consisted of 205 elderly patients (⩾ 70 years) with clinically relevant isolated aortic stenosis. Baseline characteristics at the time of echocardiography are summarised in table1.
Baseline characteristics of 205 elderly patients with aortic stenosis, and the determinants of surgical treatment
The median age of the patients was 78 years (range 70 to 93 years); 184 patients (90%) were self supporting and 21 (10%) were living in a home for the elderly. Ninety six patients (47%) were referred for the first time for diagnostic evaluation of a systolic murmur, of whom 18 were asymptomatic. Fifty four patients (26%) were already known at the outpatient clinic to have moderate aortic stenosis, and met the inclusion criteria at the time of entering the study. Fifty five patients (27%) were referred for treatment advice by other hospitals. Nineteen patients had a history of coronary bypass surgery. A coronary angiogram was performed in 93 of the 94 surgically treated patients, 45 (48%) of whom had coronary artery disease (table 1). Twenty seven (24%) of the 111 medically treated patients underwent coronary angiography which showed coronary artery disease in 19.
The surgical group consisted of 94 patients (46%). The median decision time with regard to the choice of treatment was 11 days; the median time to operation was 29 days. Three patients died while on the waiting list for an operation. A concomitant bypass procedure was performed in 34 of the 91 operated patients (37%). No other concomitant procedures were done. Eleven patients received a bioprosthesis (11 of 91, 12%). The medical treatment group comprised 111 patients. After 180 days it was decided to perform aortic valve replacement in 18 of these 111 medically treated patients (16%), mainly because of deteriorating condition.
THE DECISION MAKING PROCESS
The main predictors of surgical treatment, in order of decreasing importance, were: maximum gradient across the aortic valve ⩾ 75 mm Hg (relative risk 4.07); angina pectoris or dyspnoea of NYHA class III or IV (relative risk 2.73); age 80 years or older (relative risk 0.42); left ventricular hypertrophy on the ECG, syncope, no history of myocardial infarction, and absence of atrial fibrillation (table 1). Impaired left ventricular function at the time of Doppler echocardiography did not play a significant role in the decision to offer surgical treatment (relative risk 0.81, 95% confidence interval 0.59 to 1.13).
A decision to perform aortic valve replacement was made in 10 of the 44 patients without symptoms of angina or dyspnoea (NYHA class I). Three of these died during follow up, while all 34 medically treated patients survived.
Twenty six patients were in class II, of whom 21 were treated medically and five surgically. None of these patients died.
In 79 of the 135 patients (59%) with severe symptoms of angina or dyspnoea (NYHA class III or IV) at the time of Doppler echocardiography, a decision to offer surgical treatment was taken within 180 days. Reasons for not proceeding with surgical treatment in 56 seriously ill patients, as recorded from their clinical records, were: impaired systolic left ventricular function in eight (14%), advanced age in seven (13%), comorbidity in seven (13%), symptoms attributed to coronary artery disease in six (11%), and decrease in symptoms after starting medical treatment in five (9%). Other reasons for not proceeding with surgical treatment were obesity, a recent myocardial infarction, and insufficient vitality.
OUTCOME OF TREATMENT
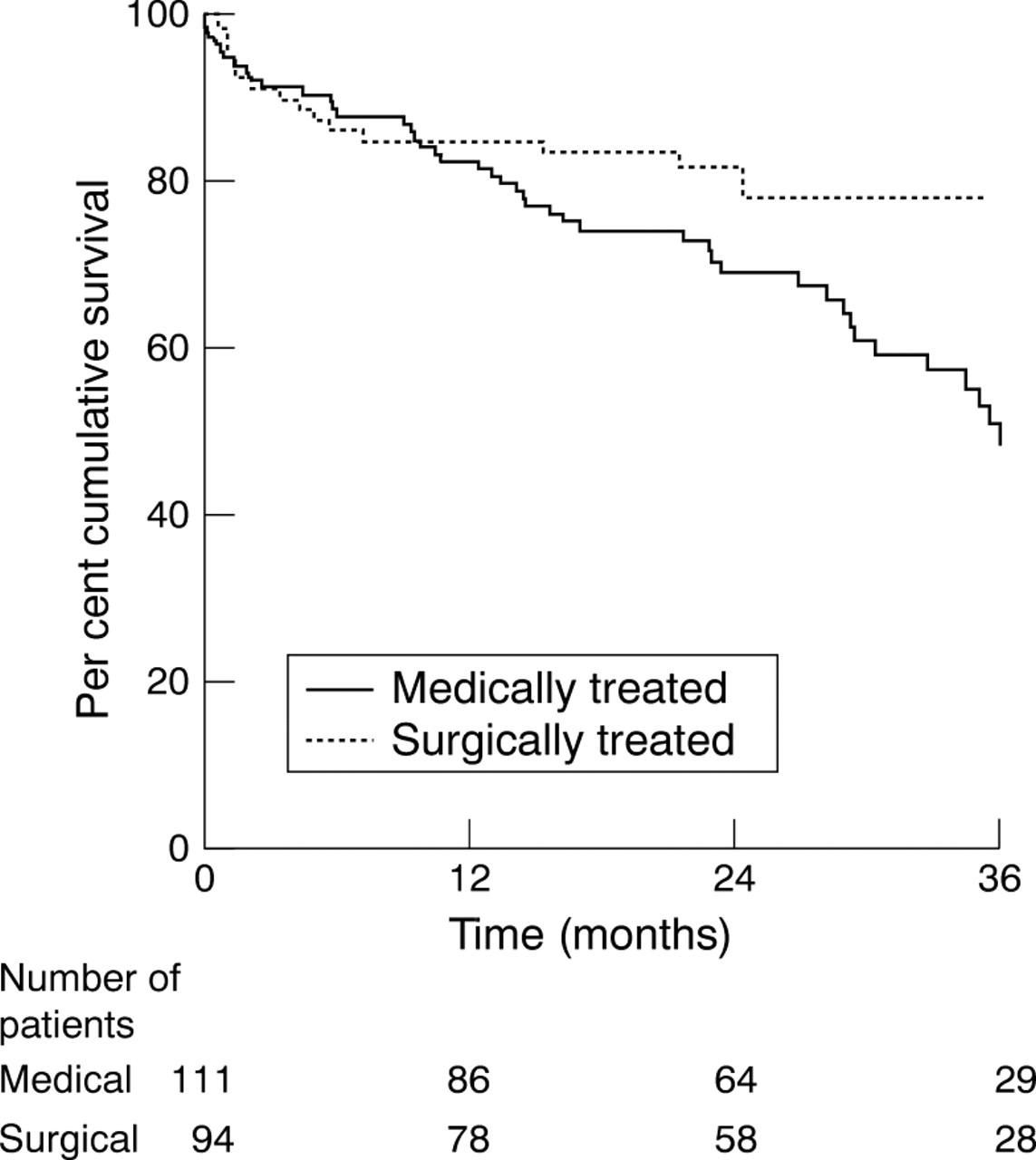
The operative mortality within 30 days after the operation was 2.2%. During the first six months the survival in both the surgical and the medical group decreased to about 85%. In the following 2.5 years the survival curve in the surgical group levelled off (three year survival 80%, 95% confidence interval 72% to 89%), whereas the measured survival in the medical group continued in a steep decline (three year survival 49%; 37% to 61%) (fig 1).

Survival in elderly patients with aortic stenosis stratified by treatment.
Impaired systolic left ventricular function (hazard ratio 4.8) was the main independent risk factor for mortality in the medically treated patients (table 2). In the surgical treatment group, impaired left ventricular function was not an independent risk factor for mortality (hazard ratio 1.7, 95% confidence interval 0.64 to 4.4). In these surgically treated patients, a previous coronary bypass operation, moderately impaired renal function (creatinine 110–250 μmol/l), age ⩾ 80 years, and a history of myocardial infarction were associated with mortality.
Determinants of mortality during follow up in 111 medically treated elderly patients with aortic stenosis
Independent risk factors for mortality in the medically treated patients were impaired systolic left ventricular function, moderate (grade 2) mitral regurgitation, and symptoms of angina or dyspnoea class III or IV. These factors in addition to age (⩾ 80 years) and sex (female) were used to calculate an individual risk score for all 205 patients (table 2). Sixty eight patients were at low risk, 68 were at intermediate risk, and 69 were at high risk (table 3). The risk score discriminated well in the medically treated group, with a three year mortality of 17% in the low risk patients and 75% in the high risk patients.
Mortality in patients with low, intermediate, and high risk score, stratified by treatment group
In the group with a high individual baseline risk score, medical treatment carried a higher risk than surgical treatment (relative risk 3.1, 95% confidence interval 1.6 to 6.1) (table 3). In the intermediate and low risk categories there was no significant difference between the outcomes of medical or surgical treatment. This was also reflected in the survival curves (fig 2).

{kind=link}
{kind=link}
Survival in patients with (A) low, (B) intermediate, and (C) high individual risk score, stratified by treatment.
Patients with surgical treatment had a much better NYHA classification at follow up than at baseline (table 4). Ten patients (11%) had the same Rankin score at baseline and follow up. In 14 patients (15%) the Rankin score had worsened and in 51 (55%) it had improved, while 17 patients (18%) died.
New York Heart Association class at baseline and at end of follow up, by treatment
In the medically treated group, many symptomatic patients had died (table 4). Twenty eight patients (26%) had the same Rankin score at baseline and at follow up. In 19 patients (17%) the Rankin score had worsened, and in 16 (15%) it had improved, while 46 patients (42%) died.
Discussion
The guidelines for surgical treatment were followed in only 79 of the 135 patients (59%) with aortic stenosis and angina or dyspnoea of NYHA class III and IV. A strict selection procedure for the surgical treatment of elderly patients with clinically relevant aortic stenosis is a possible explanation for the strikingly low operative mortality of 2.2%. The motivation for not offering surgical treatment—as given in the medical records—was impaired left ventricular function, advanced age, symptoms attributed to coronary artery disease, and decrease in symptoms after starting medical treatment. These factors are not supported by published reports and are contrary to current practice guidelines.6 ,20-24
This cohort study is the first to be directed at the decision making process leading to medical or surgical treatment as well as at the outcome of treatment in patients aged 70 years or more with clinically relevant aortic stenosis. We found that patients with serious symptoms (NYHA class III or IV) who were younger than 80 years, had a high transvalvar gradient (⩾ 75 mm Hg), left ventricular hypertrophy, and no previous myocardial infarction, were those predominantly selected for surgical treatment. Impaired left ventricular function played no clear role in the decision making process at these three Dutch university hospitals, although current guidelines recommend surgical treatment in these patients, even if they are asymptomatic.18 ,24 ,25 This conservative attitude of cardiologists towards surgical treatment of elderly patients with impaired left ventricular function and clinically relevant aortic stenosis may reflect the one sided nature of surgical cohort studies, in which operative risks and perspectives are examined and the gloomy prospects of medical treatment are omitted.26-31 Our study, however, showed that patients with impaired systolic left ventricular function profited most from surgical treatment in comparison with medical treatment (table 3, fig 2). This finding is in line with those surgical cohort studies that have shown that relieving aortic stenosis by surgical treatment effectively improves left ventricular function.32 ,33
In our study, impaired systolic left ventricular function carried a high mortality risk in the medical group (hazard ratio 4.8), while it was not an independent risk factor for mortality in the surgical group. However, studies with a longer follow up, focusing on the outcome of surgery in aortic stenosis,2-9 have shown that impaired left ventricular function is a determinant of late mortality. This difference probably reflects the relatively short follow up.
LIMITATIONS OF THE STUDY
It is not clear whether current practice guidelines24can be extrapolated to elderly patients. Although many studies describe good results of aortic valve replacement in elderly people, our knowledge of the natural history of aortic stenosis originates from studies that in most cases contain only a few or no elderly patients.23 ,26-29 In our study, impaired left ventricular function was a much more potent predictor than functional class of mortality in medically treated patients. It can be speculated that in elderly patients the onset of symptoms is delayed because they already have a decreased activity level and because they alter their lifestyle more easily than younger patients. Therefore it may be better to look for prognostic factors other than clinical symptoms to guide treatment decisions in elderly patients, for example echocardiographic indices of left ventricular function, or to use a more specific activity scale than the NYHA classification to estimate functional capacity of elderly patients.34
We used qualitative and semiquantitative cross sectional echocardiography to assess systolic left ventricular function, as this is the way left ventricular function is determined in the majority of cases in clinical practice. Qualitative assessment has been shown to have a good correlation with left ventricular ejection fraction determined by nuclear angiography.16 As coronary angiography was performed in only a few of the medically treated patients, the influence of this clinical characteristic on the treatment strategy and outcome could not be analysed.
CONCLUSIONS
Our study of 205 elderly patients with clinically relevant aortic stenosis and without serious comorbidity in three Dutch university hospitals showed that only 59% of the patients who should undergo valve replacement according to the practice guidelines were actually offered surgical treatment. Severely symptomatic patients (NYHA class III or IV) less than 80 years old, with a high maximum transvalvar gradient (⩾ 75 mm Hg) and no previous myocardial infarction, are the most likely to be selected for surgical treatment. Impaired left ventricular function played no clear role in the decision making process. However, our study indicates that the outcome in patients with impaired left ventricular function is better after surgical treatment than after medical treatment. We suggest there should be more liberal indications for surgical treatment in elderly patients with clinically relevant aortic stenosis, especially in the presence of impaired systolic left ventricular function.