Article Text

Abstract
Aim To define trajectories of perceived health-related quality of life (HRQoL) among survivors of acute myocardial infarction (AMI) and identify factors associated with trajectories.
Methods Data on HRQoL among 9566 survivors of AMI were collected from 77 National Health Service hospitals in England between 1 November 2011 and 24 June 2015. Longitudinal HRQoL was collected using the EuroQol five-dimension questionnaire measured at hospitalisation, 1, 6 and 12 months post-AMI. Trajectories of perceived HRQoL post-MI were determined using multilevel regression analysis and latent class growth analysis (LCGA).
Results One or more percieved health problems in mobility, self-care, usual activities, pain/discomfort and anxiety/depression was reported by 69.1% (6607/9566) at hospitalisation and 59.7% (3011/5047) at 12 months. Reduced HRQoL was associated with women (−4.07, 95% CI −4.88 to −3.25), diabetes (−2.87, 95% CI −3.87 to −1.88), previous AMI (−1.60, 95% CI −2.72 to −0.48), previous angina (−1.72, 95% CI −2.77 to −0.67), chronic renal failure (−2.96, 95% CI −5.08 to −0.84; −3.10, 95% CI −5.72 to −0.49), chronic obstructive pulmonary disease (−3.89, 95% CI −5.07 to −2.72) and cerebrovascular disease (−2.60, 95% CI −4.24 to −0.96). LCGA identified three subgroups of HRQoL which we labelled: improvers (68.1%), non-improvers (22.1%) and dis-improvers (9.8%). Non-improvers and dis-improvers were more likely to be women, non-ST-elevation myocardial infarction (NSTEMI) and have long-term health conditions, compared with improvers.
Conclusions Quality of life improves for the majority of survivors of AMI but is significantly worse and more likely to decline for women, NSTEMI and those with long-term health conditions. Assessing HRQoL both in hospital and postdischarge may be important in determining which patients could benefit from tailored interventions.
Trial registration NCT01808027 and NCT01819103.
- EQ-5D
- Growth modelling
- Health-related quality-of-life
- Outcomes research
- myocardial infarction
Statistics from Altmetric.com
Introduction
Health-related quality of life (HRQoL) after acute myocardial infarction (AMI) is an important clinical outcome.1–3 It allows definition of health outcomes from a patient’s perspective2 and, therefore, offers the potential to collect patient-centred ill-health, which may be used as an additional endpoint in the evaluation of care.4 Many patients consider the quality of additional life years gained just as important as the length of life5 and the goal of contemporary therapies, therefore, should be not only to extend life expectancy but also to ensure a high quality long-term health state. Consequently, HRQoL is increasingly being used as an outcome measure in clinical trials evaluating both the impact of disease burden and the effectiveness of cardiovascular interventions.2 6 However, patient-reported outcome measures are poorly reported in literature despite being collected.7 Despite HRQoL being recognised as an important clinical outcome after cardiovascular disease, little is known about how and among whom perceived HRQoL changes after AMI.
Participants of randomised studies are often a selected group of patients and their results may not be generalisable to the wider AMI population. Equally, ‘real-world’ studies of AMI HRQoL have, to date, been limited by small sample sizes,8 9 use of cross sectional designs,9 10 poor generalisability as thy are focused on specific groups of patients and/or those who benefit from specific cardiovascular interventions.1 There is often variability in HRQoL between individuals and across time; hence, longitudinal designs are useful for understanding the variability of HRQoL trajectories and the factors associated with these trajectories. The paucity of longitudinal HRQoL data for patients with AMI11 limits the comprehensive evaluation of the burden of AMI, as well its appraisal as a potential study endpoint. The Evaluation of the Methods and Management of Acute Coronary Events (EMMACE)-3 and EMMACE-412 national longitudinal cohort studies collected data concerning AMI, comorbidities, treatments, clinical outcomes and HRQoL for patients with AMI in 77 hospitals in England between 2011 and 2015. Thus, EMMACE represents an opportunity to study specific HRQoL trajectories of recovery following AMI and factors associated with these trajectories. We therefore aimed to address the gap in the knowledge base by first investigating how HRQoL among survivors of AMI vary over time and second to identify factors associated with perceived poor health state.
Methods
Setting and design
The study was based on the analysis of data from the EMMACE-3 and EMMACE-4, a longitudinal national cohort study described elsewhere.12 Eligible patients included all adults aged 18 years and over hospitalised with AMI (ST-elevation myocardial infarction (STEMI) or non-STEMI (NSTEMI)) who were admitted to 77 National Health Service hospitals in England between 1 November 2011 and 24 June 2015 with an acute coronary syndrome. Records for consenting patients were linked to the UK national heart attack register (Myocardial Ischaemia National Audit Project)13 to gather data about their medical history, type of AMI and hospital treatments.
Assessment of HRQoL
The primary outcome was self-reported three-level version of EuroQol five dimension (EQ-5D-3L) questionnaire.14 This contains two subscales: a descriptive system (EQ-5D) and a visual analogue scale (EQ-VAS). EQ-5D comprises five dimensions: mobility, self-care, usual activities, pain/discomfort and anxiety/depression. Each domain has three levels (3 L): no problems, some problems and extreme problems. The EQ-5D-3L dimensions data may be summarised as a single index score ranging from −0.5 to 1, with scores less than 0 indicating states ‘worse than death’, 0 indicating no quality of life or ‘death’ and 1 indicating full health and therefore no problems in any domain. A difference in a score of 7 for VAS and 0.05 for EQ-5D is regarded as clinically important.15 The index score was standardised to the UK population.14 The EQ-VAS score ranges from 0 to 100 with 0 denoting the worst imaginable health state and 100 the best imaginable health state. The validity of EQ-5D questionnaire in patients after AMI is established.16 EQ-5D data were collected at the time of enrolment and at 1, 6 and 12 months following hospitalisation.
Statistical analyses
Baseline characteristics for categorical data were described using frequencies and proportions. Normally distributed continuous data were described using means and SD and data with a skewed distribution described using medians and IQRs. Baseline differences between STEMI and NSTEMI were evaluated using Student’s t-test for continuous data and the χ2 test for categorical variables.
In order to analyse trajectories of HRQoL, we used two approaches. First multilevel models17 were fitted to determine trajectories of EQ-VAS scores, and the extent to which baseline patient characteristics were associated with these trajectories, over 12 months by nesting multiple time measurements (baseline, 1, 6 and 12 months) within individuals within hospitals. Second to have a deeper insight into recovery patterns, latent class growth analyses (LCGA)18 was used to determine subgroups of EQ-5D index scores with different courses of change (trajectories) of HRQoL over time. There is significant heterogeneity in HRQoL trajectories as shown in eFigure2 in the online supplementary file 1; hence, LCGA was used to capture this heterogeneity. LCGA are increasingly being used in the analysis of patient-reported outcomes.3 19
Supplemental material
The multilevel models adjusted for the following patient level factors: AMI phenotype (STEMI vs NSTEMI), sex, age (<80, ≥80 years), smoking status (never vs current or ex-smoker), ethnicity (white vs other), previous angina, diabetes, hypertension, heart failure, peripheral vascular disease (PVD), cerebrovascular disease, chronic renal failure, chronic obstructive pulmonary disease (COPD), percutaneous coronary intervention (PCI), coronary artery bypass graft (CABG) surgery, discharge medication and cardiac rehabilitation. In addition, interactions of all covariates with the linear component of the time effect were fitted to ascertain which factors were associated with changes in health state. Finally, we conducted a stratified analyses by AMI phenotype to determine unique risk factor profiles for each phenotype.
The LCGA estimated models for up to six latent trajectories, with the best class solution selected based on Bayesian Information Criterion, Akaike Information Criterion, entropy and clinical interpretability of the emerging classes.
Missing data
Multiple imputation20 by chained equations was used to produce 10 imputed data sets to minimise potential bias caused by missing data (supplementary eMethods and eTables 1–4). A sensitivity analysis was conducted comparing estimates from data with no imputations (supplementary etable 7a) and imputed data analysis (table 2). LCGA models were estimated using a full information maximum likelihood method.21 All statistical tests were two-sided, and statistical significance was considered at p<0.05. Statistical analyses were conducted using Stata (IC) V.15, R studio software and Mplus V.8.
Results from multilevel modelling of EuroQoL-visual analogue scale scores (regression coefficients, 95% CIs), stratified according to AMI phenotype
Patient involvement
While no patients were involved in setting the research question or the study design, we have involved a patient in the interpretation of the research findings, critical review of the manuscript and its dissemination.
Results
Study sample
From 16 780 acute coronary syndrome hospitalisations of consented patients across 77 hospitals in England between 2010 and 2015, we excluded 4250 which were not AMI, 2964 non-index hospitalisations (readmissions) leaving an analytical cohort of 9566 patients (n=3908 STEMI, n=5658 NSTEMI) (eFigure 1 in the online supplementary file 1) for whom the EQ-5D-3L questionnaire response rates were 97.5% (9332/9566), 74.7% (6679/8945), 63.9% (5572/8719) and 62.7% (5047/8043) at hospitalisation, 1 month, 6 months and 12 months, respectively. Sixty-nine patients (0.7%) died in hospital. Missing data levels were low for baseline patient demographic characteristics, being <5% except for index of multiple deprivation (IMD) (55.0%), body mass index (BMI) (35.3%) and ethnicity (9.3%) (table 1). The mean age for the analytical cohort was 64.1 (SD 11.9) years; 25.1% women, mean BMI 28.7 (6.04) kg/m2, median IMD 18.5 (IQR 10.9–31.8). Long-term health conditions were common, including hypertension (42.6%), angina (18.7%), diabetes (17.9%) and COPD (12.2%) and high rates of current or ex-smokers (65.3%). Typically, NSTEMI more frequently had a history of angina, hypertension, peripheral vascular disease, cerebrovascular disease, chronic renal failure, diabetes, heart failure, previous AMI, previous PCI and CABG surgery.
Patient baseline characteristics, stratified by STEMI and NSTEMI
Patterns of HRQoL over time
During hospitalisation, 69.1% (6607/9566) reported ≥1 problem on EQ-5D dimensions which increased to 73.9% (4935/6679) at 30 days, decreased to 62.6% (3491/5572) at 6 months and 59.7% (3011/5047) at 12 months. The most frequent problems (some problems or extreme problems) reported at baseline were for activities (50.1%), followed by mobility (37.6%), pain (35.5%), anxiety (35.4%), self-care (14.4%) and at 12 months were pain (41.8%) followed by activities (38.8%), mobility (36.7%), anxiety (28.6%) and self-care (13.6%) (figure 1, supplementary eTable 5). Activities and anxiety improve over time, while mobility and self-care are static. Pain is increased at 1 month and then declines slightly (figure 1). Compared with STEMI, the proportion of NSTEMI reporting ≥1 problem was higher during hospitalisation (71.2% vs 65.9 %), at 30 days (75.7% vs 71.2%), 6 months (65.1% vs 58.9%) and 12 months (62.8% vs 54.8%).
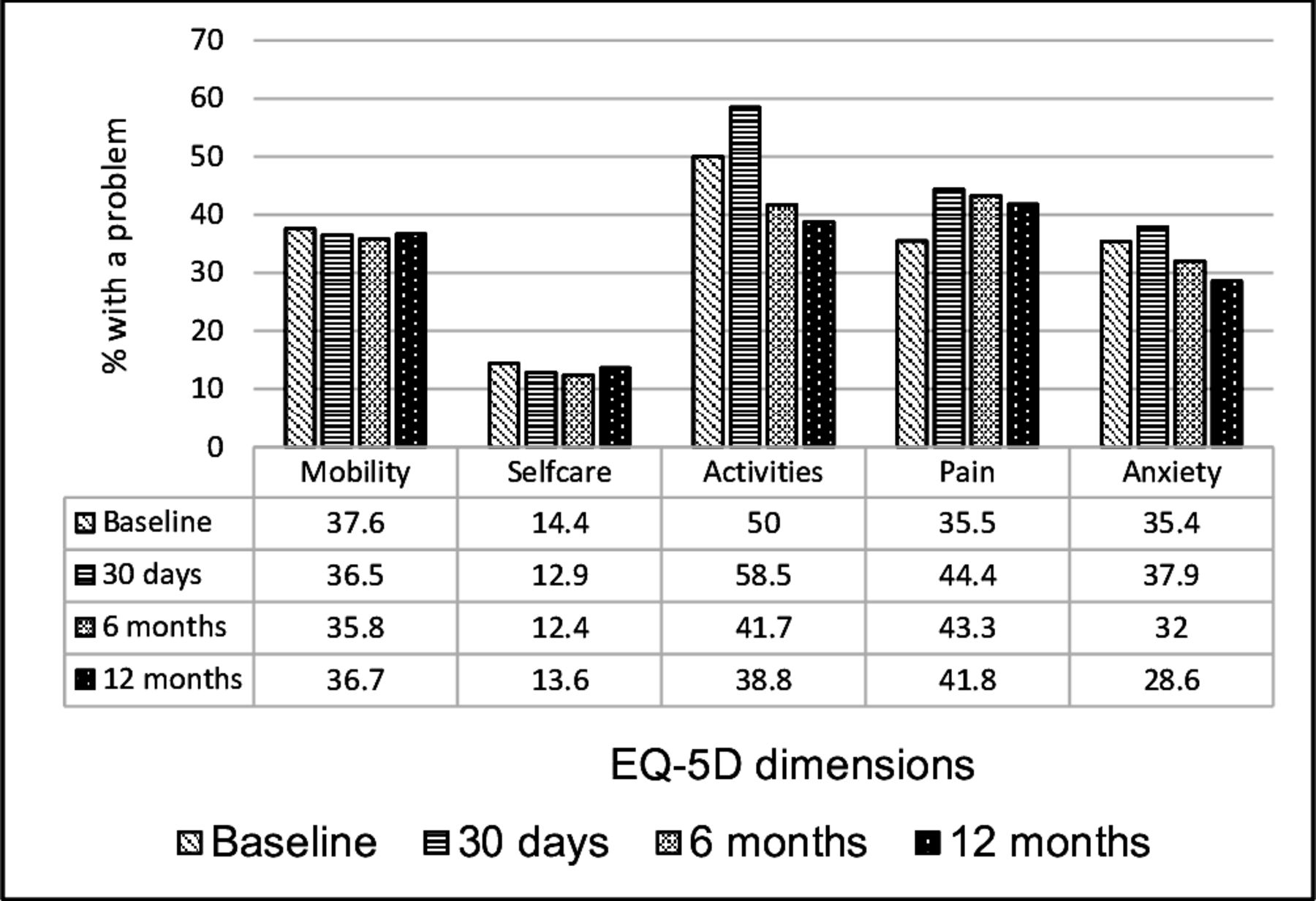
Percentage of respondents reporting less than perfect health (≥ one problem on the EuroQol-5D domains) for patients with Acute Myocardil Infaction from hospitalisation to 12 months.
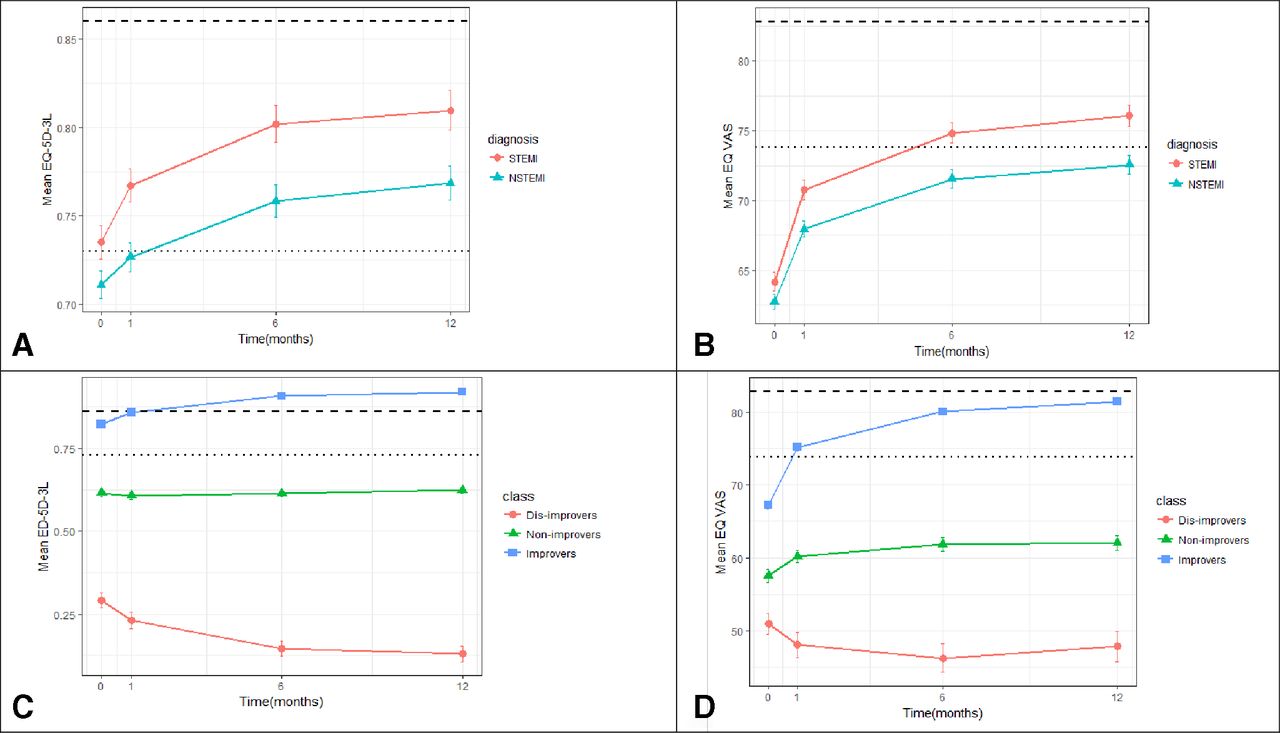
On average, health status scores improved between hospitalisation and 12 months (EQ-VAS score: 63.3 (SD 20.8) vs 73.9 (SD 18.5); EQ-5D-3L score: (0.72 (0.3) vs 0.78 (0.3). At 12 months, health status was worse for those with NSTEMI than without NSTEMI (mean (SD) EQ-VAS score: 72.6 (19.1) vs 76.1 (17.5)), diabetes (68.2 (19.9) vs 75.0 (18.0)), heart failure (EQ-VAS score: 61.6 (18.7) vs 74.2 (18.5)), chronic renal failure (62.7 (18.6) vs 74.3 (18.4)). It was also worse for women (70.8 (19.1) vs 74.9 (18.3)) and for people aged >80 years (66.9 (18.5) vs 74.7 (18.4)). Similarly, EQ-5D-3L scores were worse at 12 months for patients with NSTEMI than without NSTEMI (0.77 (0.27) vs 0.81 (0.25)), diabetes (0.69 (0.30) vs 0.80 (0.25)), heart failure (0.62 (0.28) vs 0.79 (0.26)), chronic renal failure (0.60 (0.32) vs 0.79 (0.25)), for women (0.73 (0.30) vs 0.80 (0.25), for those aged >80 years (0.70 (0.26) vs 0.79 (0.26)) and for those with no referral for cardiac rehabilitation (0.71 (0.27) vs 0.79 (0.26)). At 30 days, EQ-5D-3L scores were worse for patients with CABG surgery compared with PCI (0.68 (0.22) vs 0.77 (0.25)) but the scores were similar at 6 months (0.79 (0.23) vs 0.79 (0.27)) and slightly better for CABG surgery at 12 months (0.83 (0.21) vs 0.80 (0.26)). At all time points, NSTEMI had lower HRQoL scores compared with STEMI (figure 2A,B, eTable 6 in the supplement).
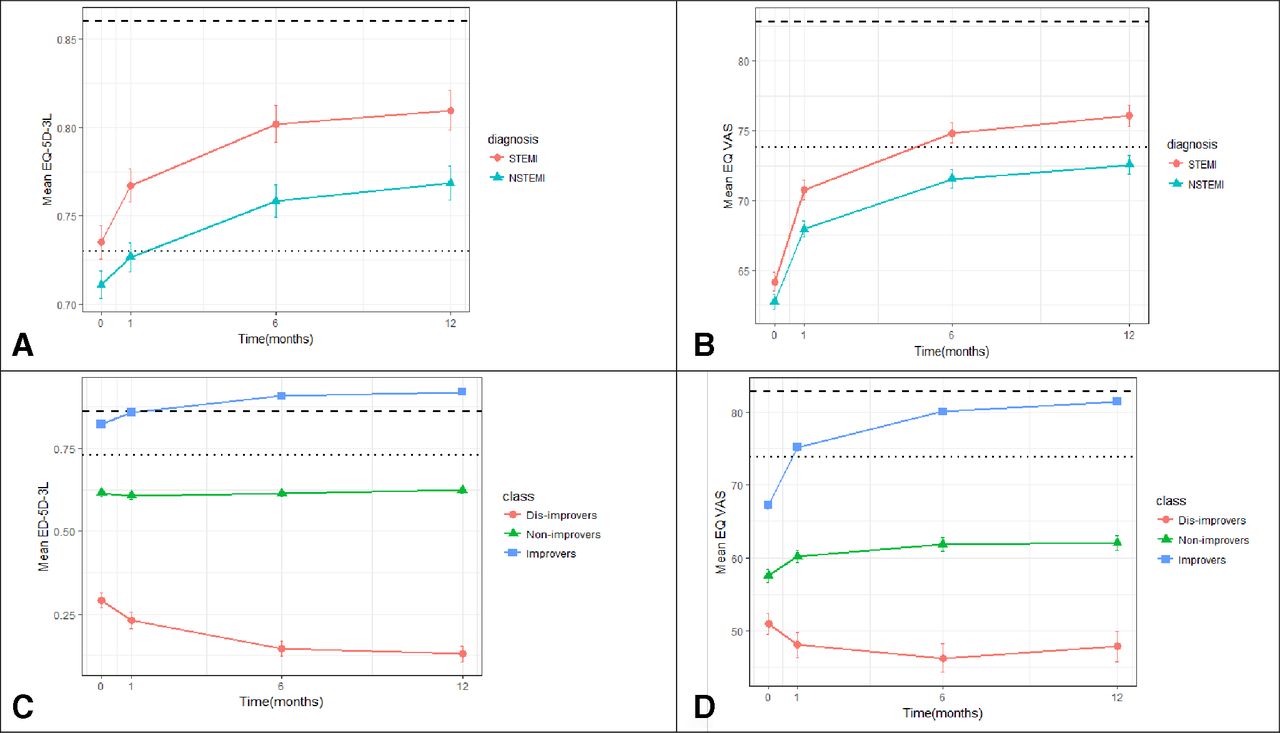
Patterns of change over a year. (A) EQ-5D-3L, (B) EQ VAS by Myocardial Infaction type; (C) EQ-5D-3L, (D) EQVAS by class, - - - - - - UK general population,…….UK >75 years). STEMI indicates ST-elevation myocardial infarction STEMI; NSTEMI, non ST-elevation myocardial infarction.
Factors associated with HRQoL trajectories
On average, the multilevel modelling analyses found that each month following AMI was associated with an increase in patients’ EQ-VAS score of 2.16 (95% CI 2.00 to 2.33) (table 2). Adjusted analysis showed that factors associated with lower health states were female sex (−4.07, 95% CI −4.88 to −3.25), ex or current smoking (−0.92, 95% CI −1.74 to −0.09), diabetes (−2.87, 95% CI −3.87 to −1.88), previous AMI (−1.60, 95% CI −2.72 to −0.48), previous angina (−1.72, 95% CI −2.77 to −0.67), chronic renal failure (−2.96, 95% CI −5.08 to −0.84), heart failure (−3.10, 95% CI −5.72 to −0.49), PVD (−2.66, 95% CI −4.69 to −0.63), COPD (−3.89, 95% CI −5.07 to −2.72), cerebrovascular disease (−2.60, 95% CI −4.24 to −0.96) and previous CABG surgery (−2.56, 95% CI −4.13 to −1.00). There was no evidence of a significant association between referral for cardiac rehabilitation or discharge medications with HRQoL. Statistically significant interactions with time were observed for age, cerebrovascular disease, COPD, previous angina, ex or current smoking status and previous PCI.
The stratified analyses by STEMI and NSTEMI showed similar associations with the exception of previous angina, CABG surgery and chronic renal failure, which were only statistically significant for NSTEMI and cerebrovascular disease which was significant in patients with STEMI.
Subgroups of HRQoL trajectories
Based on the goodness of fit statistics, the five-class solution provided the best model fit for the LCGA of EQ-5D index scores (etable 8a in supplement) but the three-class solution was preferred based on clinical interpretability. The three identified distinct HRQoL trajectories were: improvers (68.1%), non-improvers (22.1%) and dis-improvers (9.8%) (figure 2C,D). The classes were named based on the class average EQ-5D-3L scores at baseline, 1, 6 and 12 month. Improvers’ HRQoL increased between hospitalisation and 12 months (VAS score: 67.24 (SD 19.37) vs 81.44 (SD 13.04); EQ-5D-3L score: 0.83 (0.2) vs 0.92 (0.11)), compared with declining HRQoL in dis-improvers (VAS score: 51.0 (SD 21.3) vs 47.85 (SD 19.16); EQ-5D-3L score: 0.31 (0.34) vs 0.13 (0.23)). The EQ-5D-3L and EQ-VAS scores for non-improvers remained stable over time.
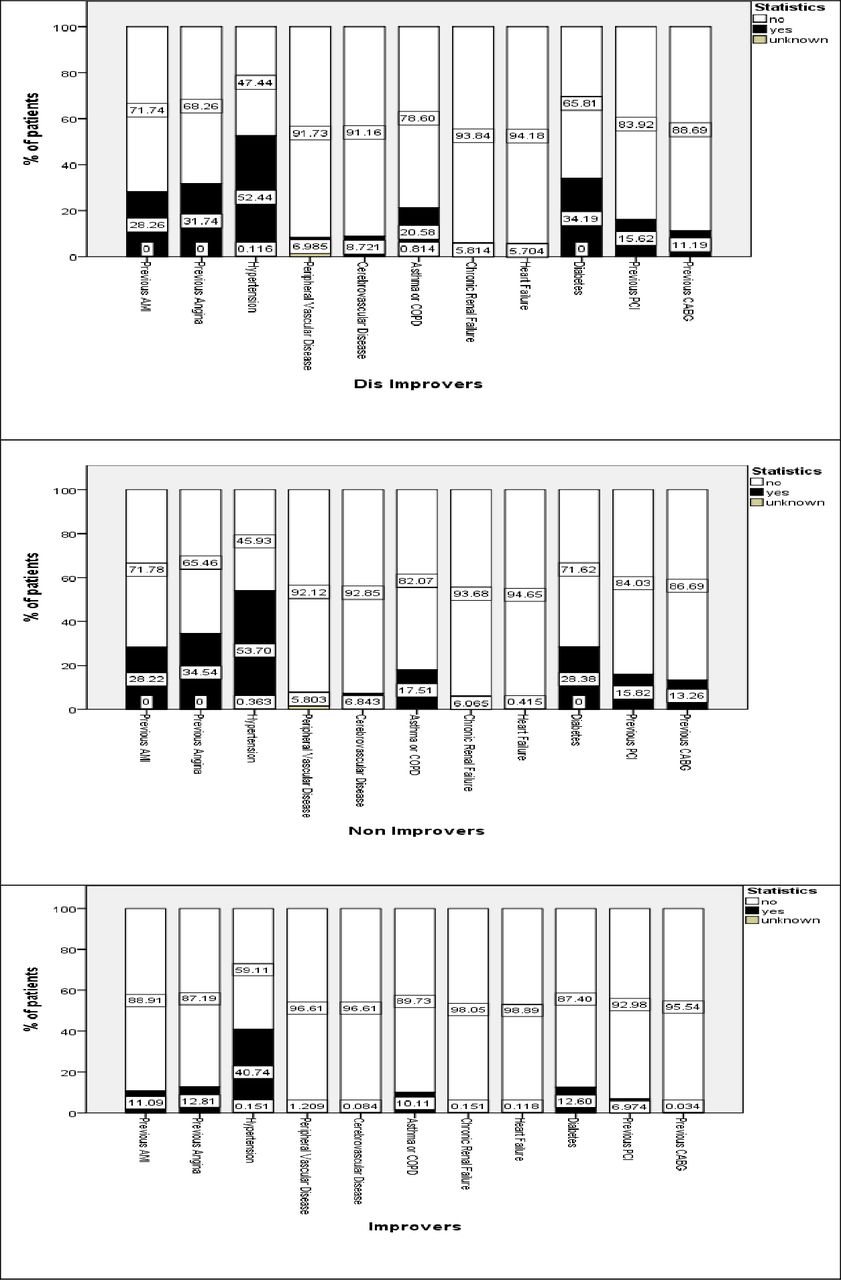
Age, gender, previous angina, previous AMI and diabetes were significant predictors of class membership (table 3). Compared with the improvers, non-improvers and dis-improvers were more likely to be of older age (62.6 vs 68.5 and 64.5), women (19.4% vs 37.6% and 35.2%), have NSTEMI (55.8% vs 69.9% and 65.8%), previous angina (12.8% vs 34.5% and 31.7%), diabetes (12.6% vs 28.4% and 34.2%), previous AMI (11.1% vs 28.2% and 28.3%), previous CABG surgery (4.43% vs 13.3% and 11.2%) and previous PCI (7.0% vs 15.8% and 15.6%) (figure 3, supplementary etable 9). Compared with improvers, non-improvers and dis-improvers were less likely to be referred for cardiac rehabilitation (92.1% vs 88.3% and 87.65). The rates of PCI revascularisation were slightly higher for improvers compared with dis-improvers and non-improvers (38.2% vs 34.8% and 31.3%) and were lower for CABG surgery for dis-improvers (dis-improvers (2.56%); non-improvers (4.41%) and improvers (4.04%)).
Predictors of class membership, reference class 3 (improvers)

{kind=link}
{kind=link}
{kind=link}
Percentange of patients with condition within each class. CABG, coronary artery bypass grafting; PCI, Percutaneous Coronary Intervention; AMI, Acute Myocardial Infarction; COPD, Chronic Obstructive Pulmonary Disease.
Discussion
This nationwide longitudinal study specifically set out to investigate how HRQoL, as measured using EuroQol EQ-5D-3L, changes over time following AMI. Among 9566 respondents surveyed over four time points up to 12 months, we found that over two-thirds reported one or more problem affecting their HRQoL at baseline and 30 days after MI. While in general HRQoL improved in the year following AMI, for a third of patients it failed to improve or declined and was worse than that of the UK general population (VAS: 82.8; EQ-5D: 0.86)22; average differences with the UK general population were greater than the minimum clinically important difference for EQ-5D-3L (0.05) and EQ-VAS (seven points).15 Following AMI, women, NSTEMI and those with long-term health conditions were less likely to report an improvement in their HRQoL.
HRQoL is a critical measure of both disease burden and the effectiveness of treatment interventions.2 3 6 It is not surprising then that the importance of measures of patient-reported health status has been increasingly recognised in randomised controlled trials.6 Such studies collect HRQoL data not only for the purposes of health economic evaluations but because of the realisation that health longevity is highly relevant to those who experience ill health.
Our results support previous findings of worse HRQoL at baseline, 1, 6 and 12 months after AMI compared with the general population2 23 and shows effects of a comparable magnitude with estimates among patients with chronic conditions such as cancer24 and pulmonary embolism.25 Whereas limitations in self-care were infrequent, moderate or severe problems were frequently reported for usual activities, pain, anxiety and mobility, both at baseline and at 12 months of follow-up. We noted, as others have, that following AMI, HRQoL more frequently declines in women,9 26 NSTEMI,9 the elderly and people with comorbidities.9 27 Poor HRQoL in NSTEMI has been attributed to having more symptomatic disease and a history of angina pectoris,9 a finding replicated in our study.
Consistent with previous studies, we noted that HRQoL was better for patients recovering from PCI at 1 month, but this gap was reduced at 6 months and became significantly in favour of CABG at 12 months28 29 and this improvement is attributed to greater angina relief in patients with CABG surgery compared with PCI.29
This research, which to our knowledge is the largest reported to date, provides novel findings. In particular, we identified three data-driven clusters of unique HRQoL trajectories—those with low HRQoL, which declined over time; those with high HRQoL, which improved and those with moderate levels of HRQoL, which did not change significantly over the study period. Each unique class of HRQoL trajectory was associated with certain patient characteristics collected at baseline. Thus enabling the prediction of future health status as well as the early identification of a group of patients with AMI who may benefit from healthcare interventions to maintain and/or improve their HRQoL. For example, dis-improvers were typically women, NSTEMI, smokers or ex-smokers and patients who had diabetes, previous angina and COPD. Such patients could be targeted for additional care and benefit from support services (eg, tailored cardiac rehabilitation, enhanced interaction with health and social care professionals or use of pharmacotherapies). The benefits of interventions for improving quality of life have been demonstrated in other diseases.30 NSTEMI is synonymous with older age and multimorbidity and may explain our finding of comorbidities and NSTEMI being associated with a declining HRQoL trajectory.
Strengths and weaknesses
The strengths of this research lie in its nationwide coverage which minimises selection bias and increases generalisability, the use of a longitudinal study design and group-based trajectory modelling using LCGA methods.3 18 Nonetheless, there are limitations to our study. Other growth mixture models were not explored; however, the LCGA used in this study produced clinically meaningful classes. We used a generic quality of life metric rather than a disease specific quality of life measure. However, the generic quality of life measure used in this study does capture dimensions that are impacted by AMI such as mobility, depression/anxiety and pain. Quality of life beyond 1 year was not considered and a UK cohort with limited racial diversity and universal healthcare access was used. The generalisability of our findings may be affected by selection bias because participants who were lost to follow-up may be those with a greater disease burden or lower HRQoL; however, we used multiple imputation to mitigate against the potential bias this may have caused. There is a possibility that HRQoL in MI survivors is affected by socioeconomic status, cardiac rehabilitation uptake, coronary anatomy, coronary artery disease burden, acuity of presentation, cardiogenic shock, cardiac arrest and other clinical factors, and therefore residual confounding remains.
Conclusions
This nationwide longitudinal study including over 9000 survivors of hospitalised AMI found that while HRQoL improves for the majority, it is significantly worse and more likely to decline for women, NSTEMI and people with long-term health conditions. Moreover, a data-driven approach has enabled the identification of three distinct, but readily identifiable groups of patients who have significantly different trajectories of HRQoL and who may be suitable for tailored interventions to improve and maintain their HRQoL following AMI.
Key messages
What is already known on this subject?
Health-related quality of life (HRQoL) is an important outcome following acute myocardial infarction (AMI). Previous studies have shown that changes in perceived HRQoL after AMI are associated with a range of clinical outcomes, including death, anxiety and depression, and medication compliance. Little is known about how and among whom perceived HRQoL changes after AMI.
What might this study add?
In this national longitudinal cohort of 9566 hospital survivors of AMI, we identified three subgroups of HRQoL trajectories: improvers (68.1%), non-improvers (22.1%) and dis-improvers (9.8%). Dis-improvers, whose HRQoL decreased between hospitalisation and 12 months, were more likely to be women, have non ST-elevation myocardial infarction and long-term health conditions.
How might this impact on clinical practice?
The characteristics of survivors of AMI associated with poor HRQoL identified in this study may be used to design targeted interventions to improve HRQoL in patients following AMI.
Acknowledgments
We gratefully acknowledge the contributions from all hospitals and healthcare professions and patients who participated in the EMMACE study.
Footnotes
Contributors TM analysed the data and drafted the manuscript. CPG contributed to the design of the study, provided clinical expert advice in interpretation of the results, and was involved in manuscript writing. MH and OA were involved in design of the study, data management, and writing the manuscript. RW provided statistical advice, interpreted data, and was involved in manuscript writing. MP and TBD were involved in manuscript writing and interpretation of the results. GO was involved as a patient advisor in the interpretation of the research and the writing of the manuscript. AH contributed to the design of the study and manuscript writing. All authors made critical revisions and provided intellectual content to the manuscript, approved the final version to be published and agreed to be accountable for all aspects of the work. CPG and TM are the guarantors for this study.
Funding This research was funded by the National Institute for Health Research (NIHR/CS/009/004) and BHF Project Grant no. PG/19/54/34511. CPG was funded by the National Institute for Health Research (NIHR/CS/009/004). TBD and MH were funded by the British Heart Foundation (PG/13/81/30474).
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval EMMACE-3 and 4 were given a favourable ethical opinion by the Leeds (West) and West Midlands Research Ethics committees (REC reference: 10/H131374 and 12/WM/0431) are registered on ClinicalTrials.gov (NCT01808027and NCT01819103), and were adopted onto the National Institute for Health Research Comprehensive Research Network portfolio (9102).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available.