Article Text

Abstract
Calcific aortic stenosis is a prevalent and worrisome healthcare problem. The therapeutic approach in asymptomatic aortic stenosis is not well established. We argue that the natural history of this disease is based on old incomplete studies with many limitations. Likewise, studies suggesting that replacement, either surgical or percutaneous, improves prognosis in asymptomatic patients with severe aortic stenosis have important drawbacks and do not support this strategy as the treatment of choice. Despite the lack of evidence, some groups recommend early valve replacement in patients with severe asymptomatic aortic stenosis. There are five ongoing randomised trials which will shed light on this topic. Our conclusion is that unless a randomised study changes the evidence, valve replacement cannot be recommended in asymptomatic patients with severe aortic stenosis.
- valve disease surgery
- aortic stenosis
Statistics from Altmetric.com
The problem
Calcific aortic stenosis is the final stage of a slowly progressing disease related to atherosclerosis, inflammation, haemodynamic factors and active calcification.1 Its prevalence increases with age. Almost 4% of people older than 70 years and 10% of those older than 80 have calcific aortic stenosis, moderate or severe in 48% of them.2 Once symptoms appear, the disease is rapidly progressive and patients require aortic valve replacement (AVR), either surgical or transcatheter. In its Fourth Adult Cardiac Database Report, the European Association for Cardio-Thoracic Surgery estimates that 41.917 surgical procedures were performed in Europe in 2010 to implant an aortic artificial valve.3 With our population getting older, we are facing a relevant, costly and worrisome health problem with a tendency to worsen in the near future.4
However, even in severe aortic stenosis, patients may remain asymptomatic for long periods of time. In this situation, the choice of treatment, AVR or medical, remains controversial. In this work, we analyse the current tendency to recommend AVR for asymptomatic patients with severe aortic stenosis (ASAS) and discuss the evidence which supports it.
The natural history: a mistaken view
The natural history of severe aortic stenosis is not as precisely known as is commonly believed. In 1968, Ross and Braunwald5 published a seminal paper whose famous figure 1 showing the average course of valvular aortic stenosis has been widely taken as the natural history of aortic stenosis in adults. The article and such figure represent the evidence available at that time. Then, patients presented with symptoms at a mean age of 48 years, most with rheumatic or bicuspid aortic valves, the mean age at death was 63 years, and infective endocarditis was the cause of death in 15%–20% of patients. These characteristics differ from the population with degenerative aortic stenosis we currently see in our clinical practice.
Several groups have attempted to investigate the natural history of ASAS6–13 (table 1). The fact that most studies combine AVR and death makes it difficult to draw definitive conclusions, since most events were driven by AVR (83.5%). Mortality in asymptomatic patients was 5.7% (between 0.3% and 4.1% per year), sudden death was uncommon (0.97%), and only a few of those studies reported how many patients developed symptoms before death. Three studies in patients with the initial diagnosis of ASAS found a strikingly higher mortality over a period of 3 years in non-operated patients, compared with the AVR group.14–16 Overall, a mortality of 30% (217 out of 709 patients) was found after 2–3.5 years of follow-up. Again, it is not specified how many non-operated patients developed symptoms before death, how many patients refused surgery, how many deaths were of cardiac causes or how high preoperative risk precluding surgery was defined.
Summary of published studies dealing with outcome in asymptomatic severe aortic stenosis
The outcome once symptoms appear is not clear. Symptoms may not necessarily be due to aortic stenosis, even when it is very severe, and not all symptoms have the same prognostic value. Dyspnoea, a frequent symptom in all series, does not equal heart failure, one of the traditional markers of poor outcome.5 In fact, hospitalisation for heart failure identifies patients with a dreadful short-term prognosis.17
From a practical perspective, it is often difficult to differentiate dyspnoea related to aortic stenosis from deconditioning, fatigue or frailty in an old patient. The presence of dyspnoea can be considered normal after a certain amount of exercise, and the role of exercise stress test in this setting is unclear.
It may be argued that in patients with severe aortic stenosis and dyspnoea at effort, a strategy of limiting daily activities can be as good as or even better than AVR, particularly in older patients with comorbidities, such as chronic obstructive pulmonary disease. Different, more disease-specific parameters measured during exercise, such as pulmonary pressure12 or peak pulmonary artery oxygen saturation,18 seem promising in detecting high-risk patients, but lack evidence. Importantly, exercise stress testing may help uncover symptoms. Besides, a positive test identifies patients who, despite being asymptomatic, have a high likelihood of sudden death7; this association has not been confirmed in other studies though. Das et al 19 performed exercise stress test in 125 patients and did not find a single death after 1 year. In that study, markers found in exercise stress testing were inconsistent and even less reliable in patients older than 70 years, who constitute the majority of patients with severe aortic stenosis. Another group found that many patients with a positive test did not develop spontaneous symptoms in the medium term.20
Angina in a patient with severe aortic stenosis may be related to concomitant coronary artery disease, and it is conceivable therefore that a percutaneous coronary intervention might render asymptomatic a previously symptomatic patient. In practice, however, both valve replacement and revascularisation are usually performed.
Syncope, particularly in the elderly, can be secondary to many causes other than aortic stenosis, and its prognostic impact in each particular patient may vary widely. In the series by Ross and Braunwald,5 syncope was present in some patients for as long as 18 years. Interestingly, syncope as a symptom of aortic stenosis identifies a group of patients with poorer outcome even after AVR.21
Finally, the incidence of sudden death in patients with ASAS is around 1% per year.20 22 Taken together data from studies dealing with the natural history of ASAS6–13 (table 1), a similar incidence of 0.97% was found. Although sudden death after AVR has been reported to be around 1% over 3 years,23 it seems a much lower risk than 1% per year until an asymptomatic patient develops an indication for AVR.
The role of AVR
The role of AVR in ASAS is unsettled. Taniguchi et al 24 studied the long-term outcome of initial AVR versus a conservative strategy in patients with ASAS. All-cause death and heart failure hospitalisation were lower in the AVR group. They concluded that the prognosis of ASAS might be improved by an early AVR strategy. Apart from the limitations inherent to a retrospective multicentre registry and to a propensity score analysis, many patients had already accepted indications for AVR and should have been excluded from further analysis, and others who developed symptoms during follow-up did not undergo surgery, which biased the results in favour of AVR. The authors reinforce the strategy of early surgery by the fact that 41% of their patients managed conservatively required AVR within 2 years, and suggest that there is little gain from waiting. This is arguable. Even assuming a 0% mortality with AVR, the authors have to keep in mind incidences of 2.4% per patient-year of disabling stroke,25 0.41% per patient-year of prosthetic endocarditis26 and 1% annual risk of permanent pacemaker implantation,27 which represents a gain of nine severe complications avoided in 118 patients in these 2 years of the ‘wait for symptoms’ approach.
A meta-analysis comparing intervention versus symptom-driven approach in ASAS included four studies.28 Patients with ASAS had a 3.5-fold higher rate of death with a ‘wait for symptoms’ strategy than with an AVR strategy. Nevertheless, patients included in the first strategy were older and sicker, no stress tests were performed to know their true clinical status, no systematic follow-up was done, and the studies included have substantial heterogeneity.28 Above all, surgical ineligibility was not captured in their database. Another recent meta-analysis,29 also including four studies (two included in the previous meta-analysis), showed a trend towards a reduction in mortality with early AVR, but no significant difference in cardiac mortality or sudden death was found. The authors suggest an individual risk stratification.
Mortality in isolated AVR is 3.7% in patients older than 70 years,30 although several centres now claim lower mortality rates. It is currently unclear whether less invasive surgical approaches as mini-sternotomy and sutureless bioprostheses will have a positive impact on prognosis. Recent trials demonstrate that transcatheter techniques offer at least similar short-term results to surgery in low-risk symptomatic patients, which opens an opportunity for this therapeutic alternative in ASAS.25 31 The lower mortality32 and short-term risk of stroke25 with percutaneous approaches make them particularly attractive in asymptomatic patients.
The role of the ‘wait for symptoms’ approach
If AVR does not offer a clear-cut benefit, one should follow the old principle primum non nocere (first, do no harm). But several factors make this assertion not so simple. First, sudden death is infrequent but not negligible, with rates higher than those found in the general population. Besides, patients may underestimate symptoms because they unconsciously limit daily activities, and the report of symptom onset is frequently deferred. In a series of 103 patients with ASAS followed up in a dedicated heart valve clinic, the first symptoms were severe in 32 of them, thereby increasing operative and late mortality.33 Lastly, different structural and functional alterations of the heart, particularly of the myocardium, may worsen prognosis despite patients being asymptomatic. In this regard, looking for high-risk markers has been an area of intense research for the last two decades, but it is debatable whether research is aiming at the correct target. Any marker that identifies an increased risk of death is yet far from ideal. An optimal high-risk marker, either circulating, structural or functional, should predict symptom onset and post-AVR outcome.
Looking for high-risk markers
Several studies have found severe calcification of the valve,6 rapid progression of peak velocity,6 abnormal blood pressure response during exercise stress test,7 brain natriuretic peptide (BNP) elevation34 and other markers to be related to outcome. With this in mind, the European guidelines35 advocate AVR in an asymptomatic patient with normal left ventricular function when any of the following is present: abnormal exercise stress test, very severe aortic stenosis (peak transvalvular velocity >5.5 m/s), severe valve calcification and a rate of peak transvalvular velocity progression ≥0.3 m/s per year, markedly elevated BNP levels, or severe pulmonary hypertension, as a class IIa recommendation, but a C level of evidence. The more conservative American guidelines36 give a IIa recommendation for abnormal exercise tolerance and very severe aortic stenosis (peak transvalvular velocity >5 m/s), IIb for rapid progression, and do not mention BNP levels or severe calcification.
All studies on which the former indications are based have important limitations. The inclusion of variables with different clinical significance and weight as events is questionable. Strikingly, most studies have included both death and AVR as end points, with most events being due to AVR preceded by the development of symptoms.6 8–13 37 Regarding aortic jet velocity progression rate, it was found to independently predict events when death and AVR were combined,6 whereas it was no longer a significant predictor when only mortality was assessed.38 Therefore, these high-risk markers identify the development of symptoms, but may be less useful as predictors of death. In addition, as documented by Otto et al,37 there is a marked individual variability in the rate of haemodynamic progression in asymptomatic valvular aortic stenosis. Other limitations, as pointed out by McCann et al,39 are that clinicians were aware of the tests results, which may have biased their decision, and that it is unknown whether AVR would have prevented death in the non-operated patients.
Imaging is gaining relevance in this setting, as evidence is emerging on structural and functional changes in the myocardium, which could worsen prognosis even in asymptomatic patients with normal left ventricular ejection fraction. In this regard, left ventricular global longitudinal strain evaluated by echocardiography40 or myocardial perfusion reserve assessed by magnetic resonance20 identified patients with ASAS who developed symptoms. Besides, the presence of late gadolinium enhancement as a marker of myocardial scar was associated with mortality in patients who undergo surgical AVR.41
Généreux et al 42 proposed a staging classification with strong prognostic power in ASAS,42 which includes cardiac damage beyond that secondary to aortic stenosis (left ventricular, left atrial, mitral, tricuspid and right ventricular damage). This classification was predictive of hard events (all-death and cardiovascular death) after AVR and in ASAS.43 This approach seems promising and could give the definitive answer to the adequate management in ASAS: an ‘individualised strategy’. With this aim, parameters predictive of death must be identified in prospective studies and AVR has to improve outcome in randomised trials. If this is the case, an earlier timing for AVR than that accepted by the guidelines should be adopted (figure 1).
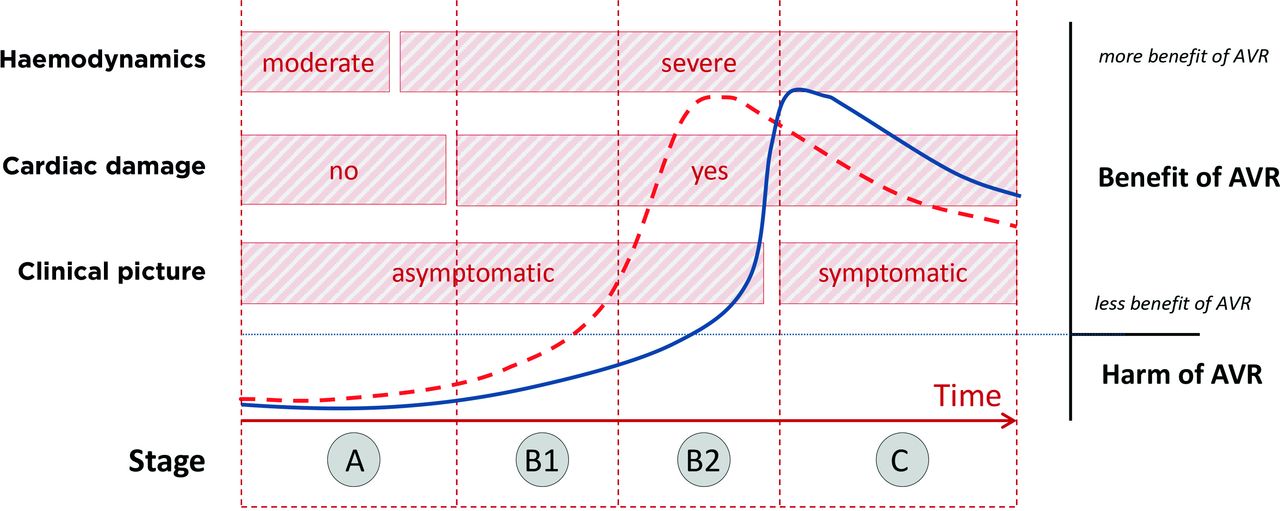
Initially, a patient with ASAS does not have cardiac damage (stage A). With time, the burden caused by severe obstruction of the aortic valve provokes cardiac damage, but the patient is still asymptomatic (stage B). Finally, the patient develops symptoms (stage C). Cardiac damage (stage B) can be demonstrated by the presence of left ventricular hypertrophy, elevated filling pressures, left atrial enlargement, atrial fibrillation, mitral regurgitation, systolic pulmonary hypertension, tricuspid regurgitation, and left or right ventricular dysfunction.42 In the initial phases, the left ventricle, the left atrium and/or the mitral valve show alterations (stage B1), but do not affect prognosis43; in advanced phases, the pulmonary vasculature, the tricuspid valve and/or the right ventricle show alterations (stage B2); at this stage, the patient may remain asymptomatic but outcome may be worsened.43 The blue line represents the current evidence: AVR does not affect prognosis in asymptomatic patients (stages A and B); only after the patient develops symptoms (stage C) a benefit is obtained with AVR since it improves outcome. The red dashed line represents the hypothesis supporting the concept that cardiac damage identifies patients with poor prognosis despite the absence of symptoms. In stage B1, there is still no benefit of AVR, but when imaging shows parameters of cardiac damage related to poor outcome (stage B2), AVR is indicated. Once the patient becomes symptomatic (stage C), AVR improves the outcome but to a less extent than if performed in stage B2. ASAS, asymptomatic patients with severe aortic stenosis; AVR, aortic valve replacement.
Left ventricular dysfunction: an exception?
Systolic left ventricular dysfunction accompanying ASAS is an indication for AVR accepted by the guidelines.35 36 Non-randomised studies show that ejection fraction and symptoms improve after AVR,44 45 which should favourably affect prognosis, although most patients were symptomatic and many had coronary artery disease.44 45 The guidelines infer that an increase in left ventricular ejection fraction in asymptomatic patients would be of prognostic benefit as well. A randomised study focused on this specific topic could be considered unethical and is not expected.
Recently, it has been shown that a left ventricular ejection fraction between 50% and 60% in moderate aortic stenosis is strongly related with further deterioration and impairs prognosis even after valve replacement.46 The authors propose that an ejection fraction under 60% in moderate aortic stenosis should be considered abnormal.
Very severe aortic stenosis: different outcome?
A preliminary study suggested that early AVR decreases mortality in patients with asymptomatic very severe aortic stenosis, defined as a valve area <0.75 cm² with a peak aortic jet velocity >4.5 m/s or a mean transaortic pressure gradient >50 mm Hg.38 The main strength of this study is that only mortality was regarded as event. Nonetheless, it was not randomised and some patients refused AVR despite being symptomatic; thus, this work should be taken as hypothesis-generating only.
A prospective study including 116 patients with very severe aortic stenosis (maximal jet velocity >5.5 m/s) showed that transaortic gradients may have stronger implications than the valve area in this setting and that the outcome of medical treatment is poor.11 Mortality without AVR (six patients; 5.1%) was quite high compared with other series dealing with severe aortic stenosis,9 10 which suggests that the natural history of very severe aortic stenosis may be worse. However, early mortality in those who underwent AVR was also quite high (six patients: one in the perioperative period and five within 3 months after surgery),11 suggesting that AVR in patients with very severe aortic stenosis may have worse results than in patients with severe aortic stenosis.
Kitai et al 47 reported on the clinical outcomes of non-surgically managed patients with severe aortic stenosis versus very severe aortic stenosis (maximal jet velocity >5 m/s, mean pressure gradient >50 mm Hg or aortic valve area <0.6 cm²). It was shown that the latter had poorer survival and valve-related event-free survival at 3 years. Remarkably, the outcome of asymptomatic very severe aortic stenosis was comparable with that of symptomatic severe aortic stenosis but worse than ASAS. Several pitfalls, particularly its retrospective nature, preclude definitive conclusions to be drawn. Moreover, it is striking that among the 90 symptomatic patients, 52% refused surgery and in 30% surgery was not recommended due to ‘physician’s unrecognition’.47 Besides, we suspect that management of symptomatic patients is very different in most Western countries.
Lancellotti et al 13 reported on data from an international registry and found peak aortic jet velocity >5 m/s to be an independent determinant of cardiovascular mortality. This association remained when peak aortic jet velocity was taken as a continuous variable and this parameter retained its negative effect on outcome after AVR.
Finally, a randomised trial comparing the ‘wait for symptoms strategy’ with surgical AVR in 145 patients with asymptomatic very severe aortic stenosis showed better outcome with surgery48 (mortality rate after 8 years: 15% in the conservative group vs 1% in the early surgery group), driven by a high rate of sudden death in the conservative arm (4% at 4 years and 14% at 8 years). Operative mortality was zero, even in patients in the conservative group who needed urgent AVR. The low mortality rate after a follow-up of at least 4 years is unusual. The high rate of sudden death in non-operated patients suggests that follow-up was inadequate to detect onset of symptoms. Moreover, patients older than 80 years were excluded (mean age was 64±9) and more than 50% had bicuspid valves; both criteria preclude generalisation of conclusions. Having said that, investigators have to be congratulated because this trial has opened a new era of randomised trials in ASAS.
A randomised study is eagerly awaited
A randomised study in patients with ASAS and high-risk markers is eagerly awaited by the scientific community. The hypothesis would be that AVR improves outcome in patients with ASAS compared with a conservative therapeutic strategy (medical treatment and AVR only if the patient becomes symptomatic). Mortality should be considered the primary end point, but outcomes related to disability and quality of life are key in this aged population. Patients assigned to the ‘wait for symptoms’ arm would be treated medically; AVR would be undertaken if symptoms appear, and this would not be regarded as an outcome. Follow-up must be extended to at least 1 year, and probably not less than 3; shorter follow-up would include perioperative deaths but not deaths in the long run in the conservative arm. There are five clinical trials ongoing fulfilling the aforementioned criteria, comparing the ‘wait for symptoms strategy’ as the control group with surgical or percutaneous AVR (table 2). All are randomised, with parallel assignment and open-label. Primary outcomes comprise death or cardiovascular death in all, and other major adverse events in some. Secondary outcomes differ but most include renal failure, endocarditis, major bleeding and stroke. The EVOLVED and EASY-AS trials consider disability and quality of life measures as well. The ESTIMATE trial has been interrupted due to insufficient recruitment.
Randomised clinical trials in severe asymptomatic aortic stenosis
Conclusions
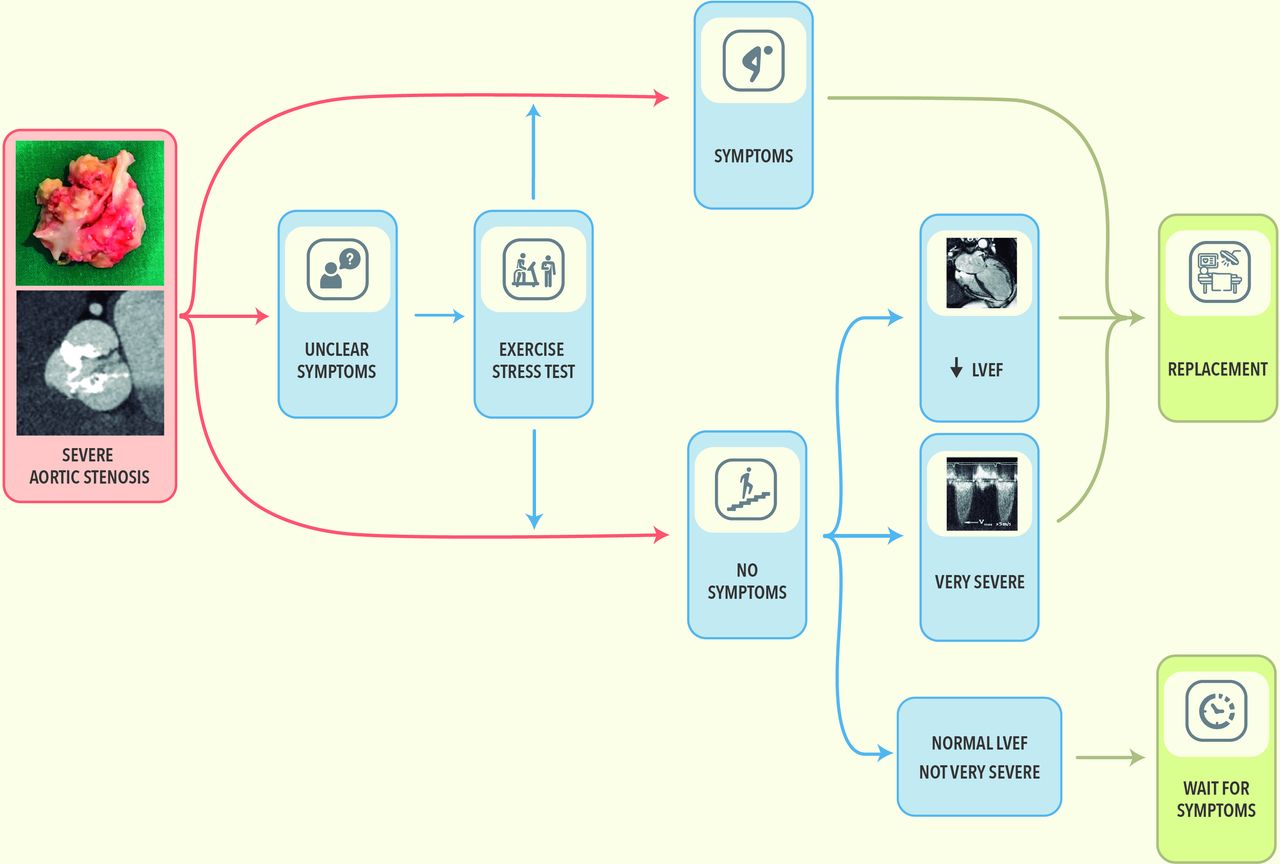
In summary, bearing in mind all the evidence herein presented and taking into account the European guidelines,35 we propose a simple strategy to decide the best option for a patient with ASAS (figure 2). We believe that while waiting the results of the ongoing randomised trials, the ‘wait for symptoms’ strategy should remain the standard approach in these patients. We acknowledge that the benefits shown by a single randomised trial tip the balance in favour of aortic replacement in highly selected asymptomatic patients with very severe aortic stenosis.

{kind=link}
{kind=link}
Management of a patient with asymptomatic severe aortic stenosis based on the evidence available. It could change if the ongoing randomised studies demonstrate that aortic valve replacement is better than the ‘wait for symptoms’ approach in terms of mortality or if the ‘individualised strategy’ shows to be of benefit (see text). Pictograms freely available at www.flaticon.com and humanpictogram2.0; LVEF: left ventricular ejection fraction.
References
Footnotes
Contributors All authors provided critical feedback and helped shape the research, analysis and the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.